INTRODUCTION
Alzheimer’s disease (AD) has been regarded as the most common cause of neurodegenerative cognitive disorders [1,2]. The absence of specific biomarkers for the definite diagnosis of AD causes AD to remain defined as a disease with certain clinical manifestations [2,3]. Major approaches for managing AD, such as acetylcholinesterase inhibitors and memantin, are not only symptomatic measures, but also unlikely to affect a late stage of AD [3,4]. This situation implies that the early detection of its risk factors and subsequently early interventions thus far remain one of the most practical treatment options [3,4].
Alteration of the thyroid hormonal state has been reported to constitute a risk factor for developing dementia at a later stage of life [5,6]. The Apolipoprotein E (APOE) gene has also been hypothesized to be a risk factor for late-onset AD [7,8]. As a result, research has been conducted to elucidate how these risk factors are correlated with cognitive function, since cognitive impairment was reported to be one of initial symptoms of AD [9].
Thyroid hormones are essential for the development and metabolism of the brain [10], ranging from cellular- to geneticlevel processes [11-13]. Indeed, epidemiologic studies have identified subclinical hyperthyroidism or a decreased level in TSH was significantly associated with cognitive impairment [14-16], while others have failed to ensure this correlation [17-19]. Similar inconsistent results have also been identified in specific cognitive domains primarily affected by thyroid function. Recent publications, for instance, revealed that lower TSH levels profoundly influenced executive function rather than memory [20,21], whereas other investigators did not reproduce this outcome [18,22]. These contrasting outcomes might be ascribed to characteristics of sample, types of thyroid-related hormones, and neuropsychological tools that each study had implemented.
Aside from TSH, the APOE gene has been also investigated in light of its influence on cognitive performance. Even though etiologies of AD have not been fully identified, carriers of the APOE ε4 allele are more predisposed to developing AD in a dose-dependent manner [23]. This allele has been reported to be correlated to cognitive impairment across cognitively-normal (CN) and cognitively-impaired elderly over the age of 60 [7,23,24]. In particular, prior studies have revealed that the ε4 allele of APOE was correlated with poor memory performance in nondemented participants [25], although others have not shown any significant association between the ε4 allele and decreased scores in memory tests among this group [23,25].
Incorporating with aforementioned research on TSH, these studies regarding the influence of APOE on memory performance lend a perspective concerning the association between thyroid hormones and APOE in the memory system. Previous studies relevant to these variables have tended to conducted across individuals with demented or mild cognitive impairment (MCI), primarily because these parameters are believed to be correlated with developing AD and one of initial symptoms of AD have been reported to be memory deficit. With the consideration of these two parameters as risk factors of AD, our study was designed to scrutinize their interplay in far earlier stages of MCI which can refer to a premorbid stage of AD, that is, cognitively-healthy state of elderly population. In light of these perspectives, our study aimed at investigating the hypothesis that these two factors and their interaction are more associated with memory performance than other domains in cognition among CN individuals.
METHODS
Selection criteria of participants
Participants were recruited from 2011 to 2018 as a part of Dementia Screening Program organized by Korean Ministry of Health and Welfare, all of whom were elderly over the age of 60 and dwelled in Chungcheongbuk-do, Korea. After being evaluated by Korean version of the Consortium Establish a Registry for Alzheimer’s Disease (CERAD-K) and Clinical Dementia Rating (CDR), subjects whose CDR score was zero were only included in the study. Modified Hachinski Ischemia Scale was also calculated by a senior psychiatrist so that individuals whose score was below 3 could enter the study. Based on Diagnostic Statistical Manual of Mental Disorders, fourth edition, test revision (DSM-IV_TR), only subjects not diagnosed with major depressive disorder were included. In order to minimize confounding factors, we excluded participants who manifested any sign of altered consciousness, as well as severe neurovascular pathology and neurological diseases. Moreover, we did not employ data from individuals who not only had medical illnesses including thyroid diseases, but also were receiving medications which may be able to alter cognitive function. All participants underwent hematologic tests to measure the serum concentration of free thyroxine (fT4) and TSH, and the identification of the APOE ε4 after obtaining an informed consent. This research was approved by Institutional Review Board of Konkuk University Chungju Hospital (KUCH 2019-12-044) and all researchers abided by its ethical codes of conduct.
Identification of APOE
Whole blood cell was obtained via an ethylenediaminetetraacetic acid tube, white blood cell being segregated to extract Genomic DNA. It was analyzed through Polymerase chain reaction-restriction fragment length polymorphism to identify the APOE ε4 allele [26].
Serum fT4, serum TSH and classification of thyroid function
Subjects were encouraged to visit clinics in the morning while maintaining a fasting state wherever possible, in order to collect serologic samples. Serum fT4 and TSH were assessed using a chemiluminescent immunoassay in the department of laboratory medicine, Konkuk university Chungju hospital. Laboratory reference ranges of serum fT4 and TSH record 0.70-1.48 ng/dL and 0.35-4.93 μIU/mL respectively. For the convenience of statistical analysis, TSH levels were evenly divided into three tertiles, resulting in tertile 1 (<2.0), tertile 2 (2.0-3.0), and tertile 3 (>3.0). In detail, in terms of a number of subjects belonging to each tertile, this numerical-based tertiles led to relatively more even-distribution rather than a group based on serum levels of hyper-, eu-, and hypothyroid states.
Neuropsychological assessment tool
Cognitive function was assessed by CERAD-K [27] comprising Verbal Fluency Test (VFT), Modified Boston Naming Test (mBNT), Mini-Mental State Examination in the Korean version of CERAD assessment packet (MMSE-KC), Word List Memory Test (WLMT), Construction Praxis Test (CPT), Word List Recall Test (WLRT), Word List Recognition Test (WLRcT), and Construction Recall Test (CRT). It was conducted by research nurses who were trained for this study and supervised by a senior researcher and psychiatrist.
Clinical Dementia Rating
A psychiatrist recorded CDR scales by interviewing family members of participants regarding six domains constituting CDR, including memory, orientation, judgment and problem solving, community affairs, home and hobbies, and personal care. Subjects rated CDR=0 were only included in the study.
Depression
Korean version of Geriatric Depression Scale (GDS-K) consisting of 30 questions was employed as a self-reporting format to assess depression. Illiterate subjects completed the form by answering original questions read by a research nurse. This scale was utilized to exclude the impact of depression on results.
Statistical analyses
Demographic profiles and clinical characteristics were compared via χ2 and t-test depending on categorical and continuous features of variables respectively. Further analysis was performed by Multivariate Analysis of Variance (MANOVA).
We divided the TSH level into three strata to identify the TSH level that primarily affects neuropsychological test scores. The TSH tertiles and APOE ε4 positivity were used as fixed factors, whereas age, education, and gender were treated as covariances to make Model I. An interaction effect between TSH tertiles and APOE ε4 was explored while controlling for confounding factors which were covariances to make Model II. The difference in mean neuropsychological test scores was investigated among TSH strata using the general linear model (GLM) analysis with post-hoc tests using the least significant difference (LSD) method. Data were analyzed using SPSS 24.0 software (IBM Corp., Armonk, NY, USA).
RESULTS
The demographic profile revealed subjects mean age and the average year of education recorded 74.48 and 6.81 respectively. The proportion of participants in each tertile was composed of 26.2% (Tertile 1), 30.0% (Tertile 2), and 43.6% (Tertile 3). The APOE ε4 was detected in 100 participants (19.7%). The analyses of clinical characteristics of subjects based on the TSH concentration demonstrated no significant correlation of TSH level with each characteristics excluding fT4 level. Particularly, GDS-K was also found to be not correlated with TSH level among CN participants (Table 1).
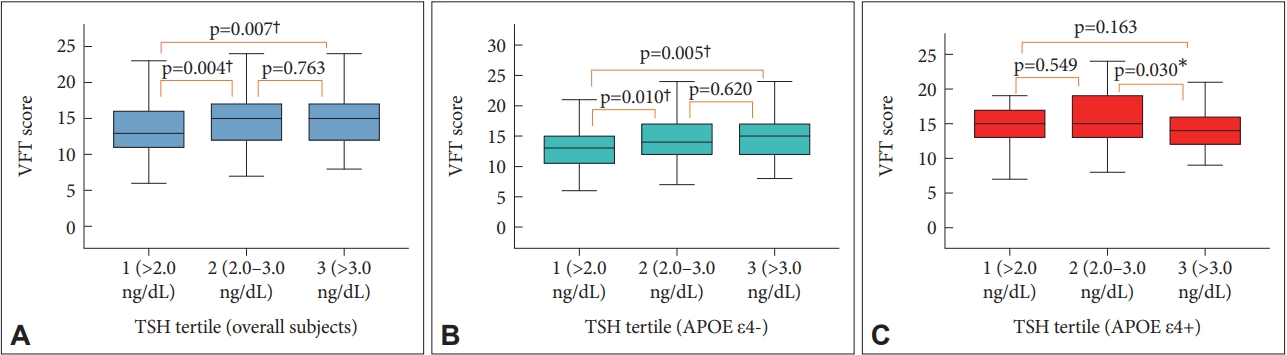
The analyses of neuropsychological variances revealed the presence of the APOE ε4 gene was significantly associated with the WLMT and WLRT scores, while the increased level of TSH was also correlated with the elevated score of VFT as well as those variances (Table 2, Model I). The further investigation of individual neuropsychological components in relation to the TSH level by introducing the interaction effect of APOE ε4 discovered that VFT recorded the only variance significantly associated with this interaction (p=0.026). On the contrary, there was no significant association between fT4 levels and scores of neuropsychological tests (Table 3).
Figure 1 illustrated this outcome in which the existence of APOE ε4 significantly tended to decrease the VFT score despite the increase of the TSH level among participants, while the absence of APOE ε4 led to the elevation of this score accordingly.
DISCUSSION
The major findings of this present study revealed that the main effect of the TSH level was significantly correlated with the VFT, WLMT, and WLRT among CN elderly individuals. The further analysis resulted in the identification of a significant interaction between APOE ε4 and the TSH concentration in the VFT. As depicted in the Figure 1, this implies that the elevated level of TSH could not contribute to higher score of VFT in the existence of the APOE ε4 allele. Incorporating with the fact that VFT task of CERAD-K is designed to assess semantic memory (SM) as opposed to WLMT and WLRT representing episodic memory (EM), this could imply that the interaction between the APOE ε4 and TSH significantly affected SM of CN subjects, in comparison with the episodic component of memory.
Since the alteration of a TSH level tends to occur in accordance with aging process and cognitive decline often accompanies aging concomitantly [15,28], the correlation between TSH and alteration in cognition has been studied [14]. Indeed, one study demonstrated low concentration of TSH was a risk factor of developing dementia [28], and it was also reported that low TSH was significantly associated with cognitive decline among the elderly population [29], which corresponds to our outcomes.
The mechanism underlying the relation between TSH and cognitive function remains uncertain. Experimental research revealed thyroid hormones play a part in the development of glial cells, proper synaptogenesis and myelination of nerve cells [30,31]. Elevated TSH in response to decreased thyroid hormones can elicit oxidative stress and subsequently trigger apoptotic neuronal cell death [15,29]. Additionally, as thyrotropin-releasing hormone (TRH) has been reported to modulate in acetylcholine synthesis and release, a decreased level of TRH induced by elevated secretion of thyroid hormones may result in disturbance in brain acetylcholine metabolism, which is believed to be related to dementia [15,29]. Particularly, TSH has been reported to be associated with regional cerebral blood flow in the bilateral temporal and hippocampal areas [32], which have been thought to contribute to the formation of explicit memory [32,33]. Similarly, our study found the positive correlation between the concentration of TSH and scores in VFT, WLMT, and WLRT. A similar pattern was also illustrated in an epidemiological study reporting that decrease in TSH was related to decline in verbal fluency among CN elderly participants aged over 75 [22].
Our findings indicated the presence of the ε4 allele could affect memory performance across CN elderly. CN middle-aged individuals carrying APOE ε4 allele were reported to show diminished volume of hippocampus, alongside decreased cerebral metabolic rates of glucose in both parietotemporal, prefrontal and posterior cingulate areas using FDG PET [32]. These areas have been well-established to be involved in memory performance. As implied in this connection, a recent study reported older participants carrying the APOE ε4 allele demonstrated poor performance in VFT, while this correlation did not exist after the exclusion of cognitively-impaired participants [8]. Other studies illustrated that APOE ε4 allele influenced an episodic memory test as compared with a semantic counterpart [34]. This is consistent with our results displaying the significant association between the presence of the APOE ε4 allele and scores in WLMT and WLRT. Interestingly, further analysis illustrated only VFT was significantly influenced by the interaction of APOE and TSH, as opposed to WLMT and WLRT. In other words, our results demonstrated that VFT representing SM was negatively influenced by the concurrent presence of the APOE ε4 and TSH, while the existence of APOE without its interaction with TSH did not significantly affect the VFT score. In light of the well-acknowledged association between the ε4 allele and AD, our findings are supported by a prior study illustrating significant impairment in SM relative to EM among AD patients [35]. Another recent study also revealed potential interplay between the ε4 allele and TSH regarding cognitive function as implied in our study [36].
One possibility concerning this apparent interaction between TSH and APOE could be attributed to their interplay affecting β-amyloid which plays an essential role in AD pathogenesis [14]. The ε4 allele has been thought to be involved in the accumulation of neurotoxic deposits related to β-amyloid, toxicity of which is believed to have detrimental effects on memory formation process. Furthermore, thyroid hormones are thought to not only regulate the precursor of β-amyloid protein, but also influence the brain metabolism and the modulation of APOE gene expression in the brain [21,37]. Both APOE and alteration of TSH is also believed to influence hyperphosphorylation of tau protein involved in the pathogenesis of AD [14,36], which sheds additional light on likelihoods of the interaction of these parameters.
On the other hand, this phenomenon can also be explained by characteristics of the neuropsychological test used in our study. The VFT of our study needs participants to generate names as many as possible after listening to a cue within oneminute-time frame, which means it requires both effortful retrieval and psychomotor speed pertaining to executive function, as well as semantic processing [33,38,39]. In other words, the score of VFT depending on this method can represent combined effects of these two categories of cognitive function. On the contrary, total scores of WLMT and WLRT did not include interference words generated by participants, which did not exist in original word lists. These scores, therefore, relatively reflected pure episodic components of memory without executive abilities. This could lead to discrepant results between VFT and other tests. This could be supported by a recent study demonstrating that the ε4 allele carriers who were cognitively intact recorded significant decline in executive function, while no statistical association between APOE and verbal fluency was found [8]. Accordingly, our result can help broaden our knowledge about the interaction between the APOE ε4 allele and TSH significantly affecting SM or even executive components embedded in VFT at least across CN elderly population.
While our study illustrated the interaction between the APOE ε4 allele and TSH appeared to interfere with SM performance in comparison with EM tests among CN elderly subjects, several limitations can be noticed.
First of all, as previously mentioned, the score of VFT could be interpreted as the combination of SM and executive function. Consequently, our findings may not ensure whether the influence of the interaction on VFT was confined to SM or executive abilities. Even if the interaction influenced both factors, our outcomes did not still clarify to what extent semantic component was influenced by this interaction. The neuropsychological test, CERAD-K, used in the study contains two types of Trail Making Tests (TMTs) designed to measure an executive compartment of cognitive function. The analysis of our results, however, did not include these tests, since a large proportion of participants were not able to complete TMTs, especially a part B of TMT (TMB) which requires subjects to connect numbers and consonant letters in an alternating sequence. The average year of education of elderly participants (6.81 years) may account for this failure to accomplish TMB, which is supported by one study showing the correlation between age, an education level and the performance of TMT among Korean elderly population [40]. This drawback could be addressed by a future study including additional tests measuring executive function.
Apart from this, this study depended on CN elderly participants residing in the rural area and the mean value of their educational level recorded 6.81, which was below the 9-year-period of mandatory education in Korea. Therefore, further studies recruiting more heterogeneous groups in terms of age, cognitive function, such as, those with MCI and AD, as well as geometrical and educational parameters, could be conducted to ensure if our findings can be replicated. This may help address compounding factors embedded in characteristics of subjects in our study.
In light of biological markers, TSH and fT4 were employed as representatives of thyroid function in this study. Other markers, such as triiodothyronine and thyroid-related antibody titers, were not taken into consideration, so that further studies considering diverse thyroid-related indicators would provide clearer elucidation concerning the interplay between thyroid function and APOE. Moreover, the analysis of APOE in our study did not consider homozygous and heterozygous types of the ε4 allele, indicating that a dosing effect related to APOE could not be identified and thereby future research will be needed to manage this aspect.
In conclusion, despite the limitations embedded in this research, our findings have demonstrated the significant interaction between the APOE ε4 allele and TSH could exist in relation to the impaired performance in SM among CN elderly. Accumulated data have suggested possibilities of the association between the APOE ε4 allele, thyroid function and cognitive performance, although discrepancies exist among investigations and exact mechanisms behind this association has not been elucidated. Impaired or diminished declarative memory is regarded as one of early symptoms in AD and the presence of the APOE ε4 allele is a risk factor of AD as well. Incorporating with the fact that aging accompanies the alteration of thyroid function, the complex interplay between thyroid-related parameters and the APOE polymorphism related to cognitive abilities requires further studies.