INTRODUCTION
Problematic Internet Use (PIU) is characterized by excessive distraction and poor self-control regarding Internet use, leading to problems in multiple areas including at school, at work, family life, as well as in other domains [1-4]. PIU has been reported in approximately 3-4% of high-school students and may become an increasingly significant public health concern given the increasing use of digital technologies in the modern world and the current trends in online content [5-7]. It has been suggested that adolescents are an at-risk population when it comes to Internet-use problems [8], because of their developmental immaturity especially in terms of self-control and boundary-setting skills [9,10].
PIU has been associated with negative psychological factors and comorbidities in retrospective and cross-sectional studies. It may have classically been associated with male teenagers [11], especially introspective males [12,13], however, similar numbers of females may also experience PIU [5], although the types of Internet-use problems (gaming and pornography viewing for males, social networking for females) may vary by gender [14]. One of the major factors linked to PIU is the amount of time spent on the Internet [15-17]. However, other factors, such as depression [18] and impulsiveness [19,20] (though not consistently by age or sex [21]), have also been found to be associated. PIU has been linked with a decreasing amount of time spent in personal relations/interactions and has been positively associated with depression, anxiety, impulse-control disorders, attention-deficit/hyperactivity disorder (ADHD), and substance-use disorders [10,22-24]. Adolescents with PIU may neglect school work, exhibit low academic achievement, demonstrate increased absenteeism [19], and have poor social support [25]. Cyberbullying behaviors have been linked to PIU [26], and negative psychological features have been observed in the victims, perpetrators, and victims-perpetrators of cyberbullying [27]. Furthermore, PIU may have a negative impact on identity formation [28], brain development [29,30], and cognitive functioning [31], which may lead to low academic performance, engagement in risky activities [32], unhealthy dietary habits [33], low quality of interpersonal relations [34], and self-injurious behavior [35] in adolescents [36,37], although there are few studies investigating the direct effects.
PIU has been proposed as a behavioral addiction with a formal psychiatric diagnosis, with Internet-gaming disorders having been introduced into section III of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) [38]. Nonetheless, the existence of ŌĆ£Internet addictionŌĆØ remains a matter of debate [39], with gaps in understanding existing with respect to the biological etiology, standardized diagnostic tools, and optimal treatment and preventive approaches. Importantly, it has been suggested that questions regarding which factors (psychological, diagnostic co-occurrences) are causes and which are consequences of PIU may hinder diagnostic and classification efforts, and that longitudinal data are needed to address these questions [40,41].
Retrospective and cross-sectional research suffer from potential recall bias and do not provide direct insight into changes over time [42]. Prospective studies may help elucidate factors associated with disease progression and remission, as well as provide data on the incidence of the condition. Despite the strengths of the prospective research model, few investigations of this type have been conducted on PIU [8,43,44]. Some studies suggest that emotional problems may be a predictor of subsequent PIU [40,41], whereas other studies suggest that changes in problematic gaming are not consistently related to changes in psychosocial and emotional factors [43,45].
The current study was conducted to examine the natural course of PIU in children/adolescents and identify the risk factors associated with transitions in PIU. Numerous studies have reported associations between PIU and psychopathology. As a result of the widespread nature of Internet access, individuals can be constantly connected to a stream of information and can participate in many activities at once. Therefore, individuals afflicted with ADHD, who are easily bored and seek instant gratification, and often have trouble with selfcontrol, may be more vulnerable to Internet addiction. The evidence also indicates that people with ADHD suffer from social [46] and emotional impairments [47], learning disabilities [48], and extreme aggression [49]. These may also be contributing factors influencing the association between PIU and ADHD symptoms. In addition, excessive Internet use may lead to a decrease in communication with those around and depressive symptoms [50]. In fact, depression appears to be the most commonly reported co-morbid psychiatric condition alongside PIU, being observed relatively consistently in case series and community surveys [51-53]. Therefore, we hypothesized that mental health concerns, particularly features of ADHD, and temperamental features, specifically greater ADHD severity, aggression, and anger, would be linked to transitions towards greater PIU severity, and high levels of persistent-PIU severity would be associated with depression and school problems. We also explored other features (e.g., main reasons for using the Internet, time free when not Internet gaming) as possible factors that might importantly relate to transitions in PIU severity.
METHODS
Study design and subjects
This study consisted of two sessions. In the first session, 650 students in 7th and 8th grades (age range: 12-14 years) were recruited from one middle school in Chuncheon, South Korea. The participating school was a single-sex school and so all volunteers in the study were male. After gaining approval from the school principals, investigators visited the schools, explained the purpose of the study to the students and teachers, obtained their informed consent (see below), distributed the questionnaires, and collected them after completion. In the second session, the same students as previously questioned, who were by this time in the 8th and 9th grade, were reevaluated one year later using similar methodologies. This study aimed to investigate the transition from one level of PIU severity to another at baseline and at one-year followup. At baseline, causal factors such as the patterns of Internet use, ADHD scale, aggression, and anger scales were evaluated; the one-year follow-up involved evaluating consequent factors such as suicidal ideation, depression, bullied-bullying, and other addictions (e.g., smartphone addiction). The results of the first session came from the previous survey [54] and the protocol of the second session trial was submitted to the Ethical Committee of Chuncheon Sacred Heart Hospital (IRB No. 2014-113). Each participant submitted a written informed consent form after receiving a full explanation of the studyŌĆÖs purpose and procedure. Before this process, letters were sent through the school to parents informing them of the survey method and purpose and outlining the procedure by which they could deny permission for their child to participate in the survey if they wished their child to be excluded [5].
Instruments
Demographics and patterns of internet use
Respondents completed self-reported questionnaires for demographic information (age, academic year) and patterns and main reasons for using the Internet.
Internet addiction proneness scale for youth test (KS-II) [55-57]
The KS-II scale has 15 items that are scored on a fourpoint Likert scale (1: Not at all to 4: Always). According to the KS-II scale total and subscale scores, students were classified into those with a high risk of PIU, those with a potential risk, and those in a low-risk group, as described previously.56 High-risk PIU (HRPIU) was defined as a total score of above 44. At-risk PIU was defined as the presence of one of the following: a total score between 41 and 43; a disturbance of adaptive function score of above 14; a withdrawal score of above 12; or a tolerance score of above 12. The low-risk PIU group included those not meeting the above criteria for high-risk or at-risk PIU. In this study, the at-risk/high-risk PIU (ARHRPIU) group included both the high-risk and at-risk groups. The internal-consistency test result (CronbachŌĆÖs alpha) for the KS-II was 0.83.
Scales at baseline
ADHD scale: the short form of the conners well-adolescent assessment self-report scale (CASS) [58]
This is a 27-item self-report instrument derived from the long form of the CASS and includes a 12-item ADHD index used to assess probable ADHD. Questions use a four-point Likert-type scaling, ranging from 0=not true at all to 3=very much true. This measure has been shown to be a valid and reliable self-report tool when used with adolescents [59,60]. The items include the highest loading items of the long form of the CASS and three generated factors with six items each: conduct problems (high scores indicate a likelihood to break rules and to engage in antisocial activities), cognitive problems (high scores indicate having problems organizing and completing tasks), and hyperactivity problems (high scores indicate having difficulty sitting still or doing the same task for very long). The internal-consistency test result (CronbachŌĆÖs alpha) for the CASS was 0.92.
Buss-perry aggression questionnaire [61,62]
This questionnaire measures aggression and hostility. The questionnaire consists of 29 items that are scored along a five-point Likert scale. The questionnaire provides an overall score, and has four subscales: physical aggression, verbal aggression, anger, and hostility. We only considered the total score in this study (the higher the total score, the greater the severity of the aggression). The internal-consistency test result (CronbachŌĆÖs alpha) for this questionnaire was 0.92.
Anger and anger expression (STAXI-K) [63]
Anger and anger expression were measured using the state-trait anger expression inventory-Korean version (STAXIK). Responses for both trait anger and anger expression range from 0 indicating ŌĆ£almost neverŌĆØ to 3 indicating ŌĆ£almost always.ŌĆØ Anger expression is measured by three dimensions reflecting introverted anger, extroverted anger, and anger control. Eight items of introverted anger, called anger-in (inhibition), reflect the frequency that one tolerates or suppresses emotions of anger, and another dimension with eight items of extroverted anger, called anger-out (expression), reflects how often one expresses oneŌĆÖs anger to surrounding persons or objects. The other eight items, known as angercontrol (control), reflect how individuals limit or control anger expression. Thus, the anger expression scores range from 0 to 24 in each dimension. The internal-consistency test result (CronbachŌĆÖs alpha) for the STAXI-K test was 0.87.
Scales at one-year follow-up
Reynolds suicidal Ideation questionnaire (SIQ) [64]
The SIQ, a 30-item self-report tool, was used to assess the suicidal ideation of participants. The respondent is asked to assess the frequency of specific thoughts about suicide and death in the past month. Responses are recorded on a sevenpoint Likert scale ranging from 0 (ŌĆ£I never had this thoughtŌĆØ) to 6 (ŌĆ£I have this thought almost every dayŌĆØ). The total scale score can range between 0 and 180. The Korean version of the SIQ was standardized by Shin [65]. The presence of suicidality was defined with higher scores reflecting a greater severity of suicidal ideation [66]. In this study, the internal-consistency test result (CronbachŌĆÖs alpha) for SIQ was 0.97.
Beck depression inventory (BDI) [67,68]
Participants were assessed for depression using the BDI. The BDI consists of 21 items for measuring the subjective severity of depression and the emotional, cognitive, motivational, and physiological symptoms of depression. The Korean version of the BDI was standardized by Hahn et al. [69] In this study, the internal-consistency test result (CronbachŌĆÖs alpha) of the BDI was 0.92.
Bullying or bullied scale [70]
Bullying or being bullied was identified using the Korean Bullying or Bullied Scale. This scale is composed of 30 items: 15 for identifying victims (for example, persons who feel left out during recess or lunch time) and 15 for perpetrators (for example, persons who shove and provoke others). Each item was assessed on a five-point scale (0 points: never, 1: 1-2 times/month, 2: 2-3 times/month, 3: at least once/week, 4: 2-3 times/week). In this study, the bullying subscale showed a CronbachŌĆÖs ╬▒=0.914, and the bullied subscale showed a CronbachŌĆÖs ╬▒=0.88.
Smartphone addiction proneness scale (SAPS) [71]
The SAPS consists of 15 items scored with a four-point Likert scale (1: ŌĆ£not at allŌĆØ to 4: ŌĆ£alwaysŌĆØ) and it consists of four subdomains: 1) disturbance of adaptive functions, 2) virtual life orientation, 3) withdrawal, and 4) tolerance. The reliability test of the scale yielded a CronbachŌĆÖs alpha of 0.880. In this study, the internal-consistency test result (CronbachŌĆÖs alpha) of the SAPS was 0.83.
Barratt impulsiveness scale-11 (BIS-11) [72,73]
The BIS-11 assesses impulsivity and uses a four-point Likert scale (1=ŌĆ£rarely/neverŌĆØ to 4=ŌĆ£almost always/alwaysŌĆØ). This instrument includes three subscales: cognitive impulsiveness, motor impulsiveness, and non-planning impulsiveness. The CronbachŌĆÖs alpha coefficient in the current sample was 0.86.
Statistical analysis
For all dimensional variables, analyses of variance (ANOVAs) were calculated, followed by pairwise group comparisons with SheffeŌĆÖs adjustment for multiple testing. The frequencies of the categorical variables were described for the four Internet-use groups of the one-year follow-up (see below). For each categorical variable, comparisons between the one-year-follow-up PIU-severity groups were calculated with binary logistic regressions followed by hierarchical selection for multiple testing. All statistical analyses were performed with SPSS 22 (IBM Corp., Armonk, NY, USA). A significance level of p<0.05 was chosen.
RESULTS
Prevalence and characteristics of PIU at baseline and at one-year follow-up
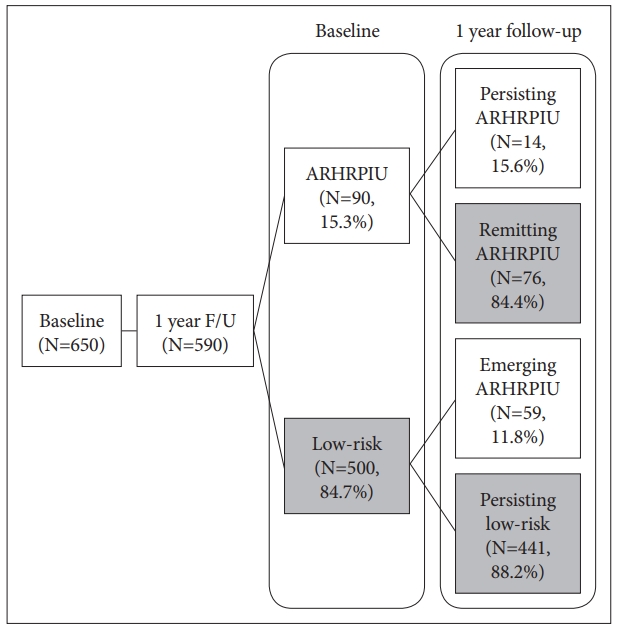
The following results refer to the one-year longitudinal study of 590 students (with a 90.8% one-year follow-up rate) who participated and provided proper information in the study at both time points. Among the total sample, 15.3% at baseline and 12.4% one year later met the criteria for ARHRPIU. Of those with ARHRPIU at baseline, 15.6% continued to have ARHRPIU (persistent ARHRPIU) and 84.4% did not (remitting ARPIU group). Among the low-risk students at baseline, 59 students (11.8%) demonstrated ARHRPIU at one-year follow-up (emerging ARHRPIU). Four hundred and forty-one students (74.7% of the entire sample, 88.2% of the low-risk at baseline) maintained low-risk use after one year (persistent low-risk Internet use) (Figure 1).
At baseline, the persistent-ARHRPIU group had the highest KS-II, ADHD, and anger-expression scores and the lowest Internet-game-free days per week. The emerging-ARHRPIU group showed higher KS-II scores than the group transitioning to low-risk Internet use (remitting-ARPIU group), although the scores on the withdrawal and tolerance subscales were similar between groups (Table 1).
At one-year follow-up, both the emerging-ARHRPIU and persistent-ARHRPIU groups revealed more depressive, motor impulsive, and smart-phone-addiction tendencies than the remitting-ARHRPIU and persistent low-risk groups. Bullying problems were more severe in the emerging-ARHRPIU group, and the persistent-ARHRPIU group demonstrated the highest levels of suicidal ideation (Table 2).
Longitudinal analysis
The stepwise hierarchical binary logistic regression analysis was used to determine the contributing factors including hours of continuous Internet use, days-free-from-Internet-gaming, and the ADHD total, ADHD cognition, ADHD hyperkinetic, Aggression hostility, and Anger expression scores which had statistical significance in the four groups and was also used to predict transitions to remittance from ARHRPIU and the emergence of ARHRPIU.
The factors that linked statistically to the transitions included the ADHD hyperkinetic subscale score for ARHRPIU remittance, and the ADHD cognitive subscale score and Internet-free days for ARHRPIU emergence (Table 3). The findings indicate that individuals exhibiting a higher hyperkinetic ADHD score were less likely to remit from ARHRPIU and that individuals exhibiting a greater ADHD cognitive dysfunction and reporting fewer Internet-free days were more likely to demonstrate an emergence of ARHRPIU.
DISCUSSION
The current study sought to examine the factors associated with the prevalence in transitions from low-risk Internet use to ARHRPIU and from ARHRPIU to low-risk Internet use in a group of middle-school boys. Our a priori hypothesis regarding the involvement of ADHD features was supported. There was also some evidence to support a potential role for temperamental features relating to anger and aggression, albeit not in the predictive models. Internet-game-free days was identified as a factor linked to emerging ARHRPIU. Taken together, these findings suggest potential targets for interventions aimed at limiting the emergence and promoting the remittance of ARHRPIU.
Prevalence
Prevalence estimates for PIU vary widely from less than 1% to about 50%, depending on the cut-off values, the population being studied, and other factors [5,40,45,74,75]. In the current study, the prevalence of ARHRPIU at baseline and at one year was similar, in the range of 12-15%. The relatively low threshold for defining ARHRPIU in the current study may have generated higher estimates than in other studies, which use more stringent thresholds. The prevalence rates in this study were determined solely by the Internet Addiction Proneness Scale for Youth Test (KS-II) [55-57] which was developed and standardized by the National Information Agency; there are no other validating processes to be found in the literature. Other possible reasons for the higher prevalence rates might be that our sample included only boys, and that Korea may have a higher prevalence of PIU than other countries. Cheng and Li [76] suggested that accessibility of the Internet and quality of (real) life could be used to explain cross-national variations in prevalence estimates of Internet addiction. According to the Organization for Economic Co-operation and DevelopmentŌĆÖs (OECD) 2011 broadband statistics [77], South KoreaŌĆÖs wireless broadband penetration is amongst the highest in the world. This environment, in conjunction with academic stress, may in part promote the use of the Internet as regards behaviors like video-gaming, social networking, gambling, pornography viewing, or other potentially addictive behaviors, consistent with the high prevalence estimates of PIU observed in Korean boys [78].
ARHRPIU emergence
Multiple factors have been suggested to affect the development of PIU, including high impulsivity, low social competence, poor emotional regulation, and spending more time on the Internet. Similar to previous results [40,45,79], the duration of Internet use sessions, gaming days per week, general inattention, hostility and anger expression were higher in those with emerging ARHRPIU than in the persistent low-risk Internet use group. The cognitive features of ADHD and the number of Internet-game-free days predicted transitions to ARHRPIU at one year. These findings suggest that interventions assessing for and targeting ADHD, particularly its cognitive features, may prevent the emergence of PIU in youths.80 Similarly, increasing the number of Internet-game-free days, as might be implemented by caregivers (parents and others), may represent another important mechanism for preventing PIU in young people [80]. At one-year follow-up, the emerging-ARHRPIU group experienced more school problems, depression, smartphone addiction tendencies, and motor impulsivity than the low-risk group. The current findings resonate with prior findings linking ADHD, hostility, depression, and anxiety to PIU [80,81]. In the emerging-ARHRPIU group, school problems, including bullying or being bullied, were notably higher than in the other groups. It is possible that school stress related to bullying or being bullied may motivate adolescents to increase their Internet use in a problematic fashion. Other factors, for example those relating to depression and suicidal ideation, were high in both the persistent- and emerging-ARHRPIU groups, and these findings are both consistent with prior findings and suggest the need for targeting mood and related psychiatric concerns among ARHRPIU youths [82].
ARHRPIU persistence and remittance
The group with persistent ARHRPIU showed more Internet-gaming days per week, higher ADHD scores, and greater anger expression at baseline and after one year; they also had higher depression scores, suicidality, smartphone-addiction tendencies, and motor impulsivity than the other groups. Gentile and colleagues [41] reported that, ŌĆśonce adolescents became pathological video gamers, they began to have poorer grades and poorer relationshipsŌĆÖ. Although only a small portion (2.4%) of our sample showed persistent ARHRPIU, they appeared to have the greatest psychopathology, including higher depression, suicidal ideation, and impulsivity scores. The main factor linking a transition from ARHRPIU to lowrisk Internet use was lower levels of ADHD hyperkinesis. This finding suggests that youths who mature and develop better motor control may simultaneously be better able to control their behavior related to Internet use. Furthermore, these findings raise the possibility that by assessing for and targeting ADHD hyperkinesis, it may be possible to help youths transition to less problematic levels of Internet use.
Depression and suicidal ideation scores were significantly higher in the persistent-ARPIU group than the other groups, followed by the emerging-ARPIU group. Depression and low self-esteem are important considerations in adolescent suicidality, with bullying and PIU possibly contributing to suicidality both directly and indirectly [83]. Young [84] proposed that lonely people may fulfill unsatisfied social needs through virtual means, leading to PIU, greater social isolation, and depression. Bullying may lead to serious mental and physical sequelae, and the victims of chronic school bullying may be at a greater risk of suicidal and aggressive behaviors [82]. In addition, cyberbullying is an important concern and may lead to victims and perpetrators feeling more depressed, lonely, and isolated, thus impairing social relationships and promoting suicidal tendencies. The data suggest that victims and perpetrators of bullying may use the Internet for longer periods of time and with a greater frequency, and so may be more prone to PIU [85]. They may also have higher expectations regarding Internet use and virtual interpersonal relationships, which itself may promote PIU.
The stability of ARHRPIU
Spontaneous recovery has been reported for addictive behaviors including substance-use problems, with 40% of recoveries for alcohol-use problems involving low-risk drinking [86], and the personal history of smokers consuming no more than 10 cigarettes per day being observed to be considerably fluid [87]. Similar to other potentially addictive behaviors and disorders, PIU may have a high rate of spontaneous recovery. King et al. [43] reported that 75% of individuals with PIU ceased to exhibit problematic behaviors at a two-year follow-up, and a recently published study reported that only 1% of pathological gamers remained pathological after two years [36]. In contrast, Gentile et al. [41] found that 84% of pathological gamers were still pathological gamers two years later; other studies have found that about 50% of pathological gamers remained pathological gamers one year later [16,45]. There is no consensus regarding the pathways that might discriminate between those who continue to exhibit PIU and those who do not, or between those who, over time, develop PIU and those who do not. With respect to natural spontaneous recovery, Shaffer and colleagues proposed an adaptation model for gambling: [88-92] individuals adapt relatively quickly after exposure to gambling opportunities are changed and frequently transition between levels of problem-gambling severity, including from more problematic to less problematic levels. In the current study, only 15.6% of individuals exhibiting ARHRPIU at baseline continued to have ARHRPIU one year later, and 11.8% of individuals exhibiting low-risk behaviors at baseline transitioned to having ARHRPIU. Thus, while the overall prevalence of ARHRPIU remained comparable at both time points, the individuals exhibiting ARHRPIU were largely different. Multiple possibilities may explain these seemingly volatile transitions. Firstly, the mean age of the sample was low. Scharkow et al. [45] reported that for adults aged 40 years and older, stability was very high for periods of up to four years; however, adolescents show less stability, and our study included youths between 12 and 15 years old. Secondly, compared with addictive behaviors in adults, adolescent addictive behaviors may be more affected by environmental, psychological, and relational factors. PIU in adolescents may represent a ŌĆśphaseŌĆÖ of development, or a ŌĆśphaseŌĆÖ precipitated by acute or transient stressful situations. The findings, when considered in this context, suggest that proper preventive approaches should be considered, developed, and implemented at this important stage in a young personŌĆÖs development.
Strengths, limitations, and conclusions
In this study, some limitations should be noted. Firstly, the investigation was based on self-reported data, which are subject to recall biases amongst others. Secondly, the sample consisted solely of middle-school boys. A further study of females and other age groups is needed. Thirdly, although it was a prospective study, the follow-up period was one year, and future studies of longer durations are warranted. Finally, except for the Internet addiction scale, different psychological scales were used at baseline and one-year follow-up. The use of a broader range of assessments at both times (which, in our study, was limited by subject burden) may have identified different factors linked to transitions in PIU severity. Furthermore, the Internet Addiction Proneness Scale for Youth Test (KS-II) [55-57] was developed and standardized by the National Information Society Agency, however, there are no other validating processes regarding the KS-II in the literature. Despite these limitations, the present findings support the previous studies in that specific negative-health features are linked to transitions in ARHRPIU. Furthermore, the findings suggest that interventions are needed and may be best targeted at specific groups of youths.