INTRODUCTION
Insomnia is highly prevalent in the general population, with prevalence ranging from 10% to 48%. It is likely to become chronic if insomnia is not dealt with appropriately or immediately [1]. Individuals with chronic insomnia can be affected by adverse health outcomes such as cognitive decline including Print ISSN 1738-3684 / On-line ISSN 1976-3026 OPEN ACCESS dementia, cardiovascular diseases [2], metabolic disease [3], depression [4], and suicidal risk.5 As sleep has a crucial function in memory restoration [6,7], adequate treatment of insomnia could delay or be protective for cognitive decline in the future.
Up to now, therapeutic options for insomnia are limited to medication and cognitive behavioral therapy (CBT). Although CBT is the first recommendation for chronic insomnia [8], CBT requires some time and cost for face-to-face encountering with therapists as well as willingness of patients to participate in the treatment. If CBT for insomnia is not sufficiently effective or is unavailable, pharmacological intervention can be offered. In clinical practice, patients who have suffered from insomnia severely usually report considerable anxiety or worry [9] and they are likely to prefer medications [10]. The most widely used medications for insomnia are benzodiazepines and benzodiaze- pine-receptor agonists. However, long-term use of benzodiazepines is known to be associated with an elevated risk of dependency, development of tolerance, and rebound insomnia on discontinuation and a risk of cognitive impairment such as visuospatial ability, speed of processing, and verbal learning [11]. Thus, pharmacological guidelines for insomnia from American Academy of Sleep Medicine [8], European Sleep Research Society [12], and American College of Physicians [13] have provided a recommendation that prescriptions should be limited to four to five weeks or less. Nevertheless, the proportion of patients receiving long-term prescription of benzodiazepine is not negligible [14,15]. Long-term users can be predicted by early age of insomnia onset, more frequent benzodiazepine use, and higher state-anxiety [16]. A relationship between cognitive decline including dementia and long-term use of benzodiazepine has been reported [17]. However, it remains controversial due to heterogeneity of studies and unknown mechanism. Chronic insomniacs usually worry about their cognitive decline associated with long-time use of benzodiazepines. Complicating issues exist regarding whether insomnia disorder itself is associated with cognitive deficits [18] or benzodiazepine used for treatment of insomnia might change the cognitive function [11,17].
As insomnia becomes chronic, the hyper-arousal phenomenon which represents arousal signs in somatic, cognitive, and central nervous system (CNS) in body is usually observed. The CNS arousal can be measured by the electroencephalography (EEG), and quantitative EEG is an easy to apply and cost-effective method to estimate temporal resolution of functional brain activities by quantifying, as well as has advantages over EEG in the dimensional approach to symptomatology of psychiatric disorders compared to normal value [19,20]. It have been reported that the EEG of patient with insomnia showed increased activities of beta or gamma frequency, and/or decreased activity of theta frequency during sleep period or before sleep onset [21-24]. However, daytime EEG of chronic insomniacs have not been investigated yet although cognitive decline can be usually experienced mostly during the daytime. The aim of this study was to explore whether long-term exposure of benzodiazepine might be associated with cognitive decline in chronic insomnia compared to drug-free insomniacs and healthy controls. In addition to neuropsychological performance, daytime EEG was performed to understand effects of benzodiazepine on brain activity comprehensively.
METHODS
Participants
As a case-control study, we recruited aged 55 years or older with insomnia disorder who were taking medications from the sleep clinic at Seoul National University Bundang Hospital (SNUBH). We collected information related to previous history of medication and insomnia symptom through face-to-face interview by a psychiatrist. Insomnia disorder was diagnosed according to Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition by physicians specialized in sleep disorders. Chronic insomniacs were defined as those who have sleep disturbance and associated daytime symptoms that present for at least three months [25]. Drug-free insomnia patients and age-and sex-matched healthy controls were enrolled by advertisement at local newspapers and subway stations. Those whose duration of insomnia disorder was more than one year were included in the study. None of these participants showed other sleep disorders, major psychiatric disorders, dementia, substance use disorders, neurological disorders, or any history of brain injury. This study was approved by the Institutional Review Board of SNUBH (B-1509/316- 002). All participants were informed of the purpose and procedures of the study. They gave written consent before entering this study.
Measurements
Sleep and mood-related questionnaires
For evaluating insomnia severity and daytime sleepiness of participants, insomnia severity index (ISI) [26] and Epworth sleepiness scale (ESS) [27] were used. Additionally, Beck Depression Inventory (BDI)-II [28] was used because depressive symptoms could affect cognitive function. Subjects with BDI-II Ōēź20 were excluded from final analysis.
Neurocognitive function test
We used the Korean version of the Consortium to Establish a Registry for AlzheimerŌĆÖs Disease Assessment Packet Neuropsychological Assessment Battery (CERAD-K-N) to evaluate cognitive function of all subjects [29]. The CERAD-K-N consisted of nine neuropsychological tests, including 1) general cognitive function: the Mini-Mental State Examination (MMSE), 2) memory function: the Word List Recall Test, the Word List Recognition Test, the Constructional Recall Test, and 3) executive function: the Categorical Fluency Test, the Constructional Praxis Test, and the Trail Making Test A (TMT-A), and Frontal Assessment Battery. Clock Drawing Test for visuospatial abilities and Digit Span Test for attention were additionally administered to subjects. Scores of CERAD-K-N were used as Z-scores after adjusting for subjectsŌĆÖ age and education. In case of participants who had abnormal cognitive function, cognitive disorder specialists in the Division of Geriatric Psychiatry clinically evaluated for confirmative diagnosis of mild cognitive impairmant (MCI) based on stand criteria for MCI [30] by means of a face-to-face standardized diagnostic interview.
Quantitative electroencephalography
EEG at waking state was performed at fixed times around 9 am or 4 pm and it was set at a time period during which alertness was maintained, neither right after mealtime nor being too sleepy. Test was recorded in a sitting position for 15 min. For the first 7 min, subjects kept their eyes closed. For the next minute, subjects opened their eyes. For the last 7 min, subjects kept their eyes closed. All subjects were observed by an examiner to check and prevent drowsiness. EEG electrodes were placed according to the international 10-20 system at FP1, FP2, F3, F4, F7, F8, C3, C4, P3, P4, T3, T4, T5, T6, O1, and O2, with an average reference. Recording of EEG started when electrical impedance of all electrodes was below 5 k╬®. EEG signals were sampled at 1,000 Hz and digitalized. The high pass filter was set to be 100 Hz with the low pass filter set to be 0.3 Hz. An artifact-free 120-s EEG recording with eyes closed (24 epochs of 5-s EEG segments) was selected by visual analysis. Artifacts comprised muscle activity, small body movements, eyelid movements, and micro-sleep. Spectral analysis for EEG data was done by the fast Fourier transform. Absolute power values of five bands at each electrode were computed: delta (1.0-4.0 Hz), theta (4.0-8.0 Hz), alpha (8.0-12.0 Hz), beta (12.0-25.0 Hz), and high beta (25.0-30.0 Hz). Relative power values were computed as the percentage of absolute power and grouped into five cerebral regions: frontal, central, parietal, temporal, and occipital areas.
Benzodiazepine exposure
As an independent variable, information of benzodiazepine exposure before the index date was collected through a medical chart review of SNUBH, retrospectively. Starting age of benzodiazepine use and duration of exposure over the followup in SNUBH were obtained. We also calculated total duration of exposure by including duration of previous exposure before coming to SNUBH depending on the participantsŌĆÖ report. Long-term benzodiazepine users were defined as receiving BDZs for more than 180 days within one year period [31,32]. Defined daily dose (DDD) was defined as the assumed average maintenance dose per day for a drug used for its main indication in adults according to World Health Organization (zolpidem, 10 mg; zolpidem CR, 12.5 mg; alprazolam, 1 mg; clonazepam, 8 mg; lorazepam, 2.5 mg; diazepam, 10 mg; clobazam, 20 mg; triazolam, 0.25 mg) [33]. It is widely used as a dose standard unit per day for drug utilization studies [32]. We calculated DDD as the total amount of benzodiazepine exposure before the index date as follows: First, the total milligrams for each benzodiazepine prescription were calculated by multiplying the number of pills. Second, this sum was divided by assigned DDD for each benzodiazepine. Third, it was divided by the total duration (days) from initial exposure to the index date. An individualŌĆÖs cumulative dose of benzodiazepine was calculated by summing up DDD amounts of all benzodiazepine prescriptions during the follow-up period in SNUBH.
Statistical analysis
Results are reported as means┬▒standard deviations (SDs). The Kolmogorov-Smirnov test was used to confirm normality of all data. Comparisons of demographic characteristic, sleep variables, and mood variables among three groups were performed using the Žć2 test or analysis of variance with post hoc. Results (Z-scores) of neuropsychological tests were compared by multivariable analysis of covariance (ANCOVA) after adjusting for confounders including ESS, BDI, and exposure of other psychotropics. For estimating statistical power strictly, BonferroniŌĆÖs correction for multiple comparisons was performed to compare Z-scores. Group-band interaction and between group-differences in relative EEG power were assessed by two-way ANCOVA for each cortical region, with group as an independent factor and five frequency bands as repeated measures. Confounding factors of EEG such as age, sex, ESS, and BDI were adjusted. In addition, we performed subgroup analysis only for insomnia with benzodiazepine group. Spearman correlations were computed to examine the relationship between benzodiazepine exposure and the change of cognition or EEG. All significance tests were two sided and p-value was set at <0.05. SPSS version 22.0 for Windows (IBM Corp., Armonk, NY, USA) was used for all analyses.
RESULTS
Figure 1 shows a flow of the present study. Forty patients with insomnia disorder who were taking benzodiazepine, 33 benzodiazepine-free patients with insomnia disorder, and 35 age and sex-matched controls were enrolled at baseline. After excluding 24 subjects whose BDI Ōēź20 or EEG with artifact, a total of 84 participants were included in the final analyses: insomniacs using benzodiazepine (n=29), drug-free insomniacs (n=27), and age- and sex-matched control (n=28). Ages (mean┬▒SD) of the participants were 68.03┬▒8.38, 64.89┬▒6.94, and 64.56┬▒6.48 years in insomniacs using benzodiazepine, drug-free insomniacs, and controls, respectively. Insomnia severity was significantly different among three groups (ISI scores of drug-free insomniacs [18.11┬▒5.13] vs. insomniacs using benzodiazepine [11.66┬▒7.13] vs. control [4.89┬▒4.98], p< 0.001). Drug-free insomniacs reported more severe symptoms than insomniacs using benzodiazepine (p<0.001). Sex ratio, daytime somnolence, and mild cognitive disorder were not significantly different among the three groups. In insomniacs using benzodiazepine, mean age at onset of benzodiazepine use was 61.9┬▒8.6 years and duration of benzodiazepine exposure was 11.8 (median) years (range, 0.54-30.24 years). The DDD was 0.72┬▒0.52 mg (reference is 1) in insomniacs using benzodiazepine (Table 1).
When we compared Z-scores of neurocognitive function among the three groups (Table 2), insomniacs using benzodiazepine showed a decreased executive function than drugfree insomniacs and controls in alteration of Trail Making Test A (insomniacs using benzodiazepine [0.73┬▒0.66] vs. drugfree insomniacs [1.27┬▒0.38] vs. control [1.09┬▒0.47], p<0.001) and categorical fluency (insomniacs using benzodiazepine [-0.01┬▒ 0.99] vs. drug-free insomniacs [1.26┬▒0.97] vs. control [0.77┬▒1.08], p=0.002) than drug-free insomniacs after adjusting for score of BDI, ESS, and exposure to other medications. Although we also conducted subgroup analysis with only subjects prescribed benzodiazepines for more than 5 years to ex- clude a reverse causation in which cognitive decline usually preceded insomnia symptoms as a prodrome, overall results were not changed.
Especially in insomniacs using benzodiazepine, we tried to examine effects of characteristics in benzodiazepine usage on cognitive function (Table 3). Start the use of benzodiazepines at an older age was associated with a decrease of executive function (Trail Making Test A: rho=-0.468) and a decrease of attention/concentration (digit span backward: rho=-0.412) with a large effect size. Longer duration of benzodiazepine exposure was associated with decreases of executive function (frontal assessment battery: rho=-0.444) and global cognition (MMSE: rho=-0.454). However, DDD and cumulative dose of benzodiazepine were not associated with any cognitive function.
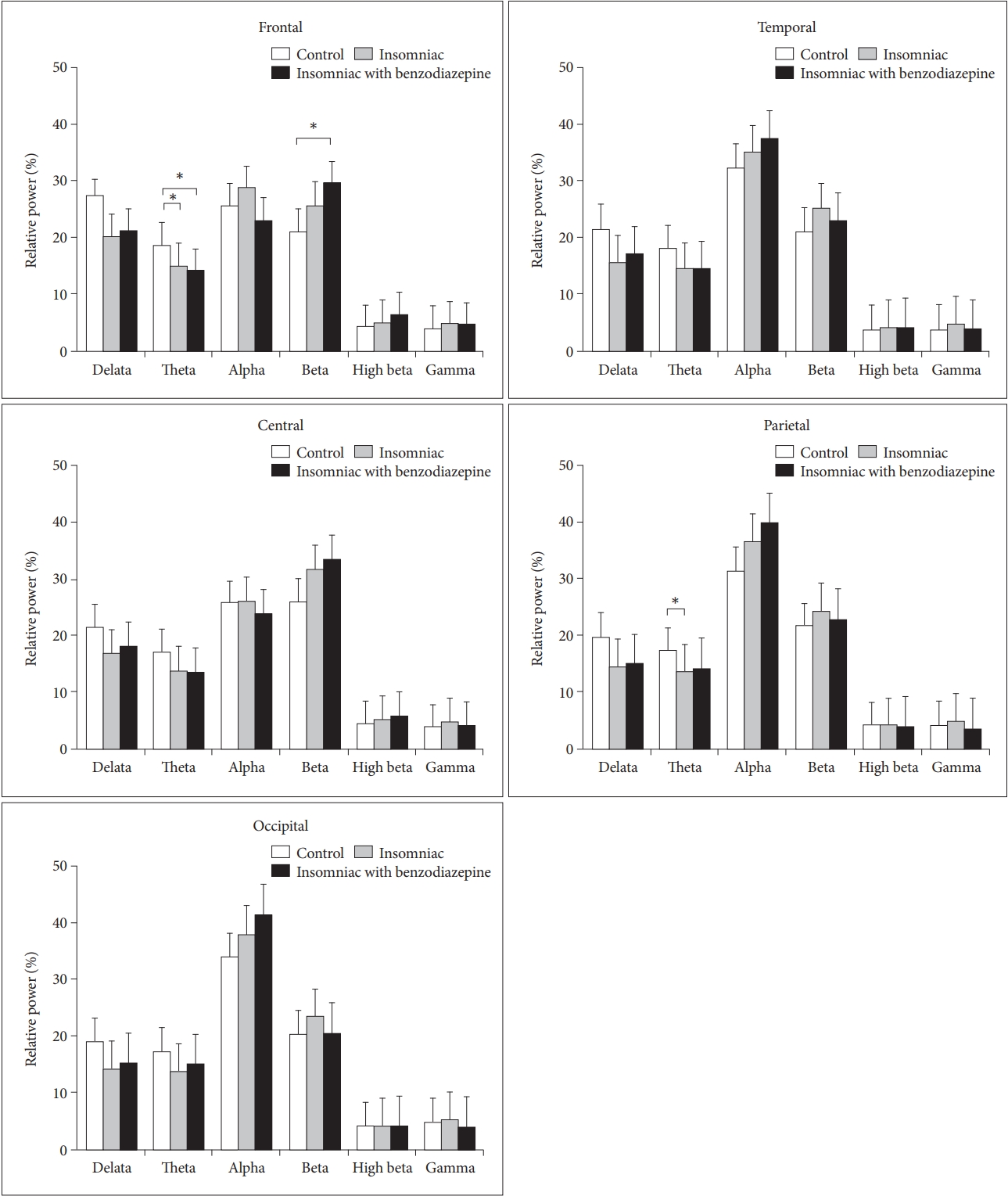
When we compared quantitative EEG in three groups after adjusting for age, sex, and scores of BDI and ESS (Figure 2), significant group-band interaction (F=3.099, p=0.01) in frontal area and between-group difference (F=3.608, p=0.032) in parietal area were found. In post-hoc analyses, a significant difference between insomniacs using benzodiazepine and drugfree insomniacs was not found. Instead, insomniacs using benzodiazepine showed low relative theta power (insomniacs with using benzodiazepine=14.1% vs. control=18.5%, p=0.014) and high relative beta power (insomniacs with using benzodiazepine=29.3% vs. control=21%, p=0.045) in frontal region than controls. Drug-free insomniacs showed low relative theta power in frontal region (insomniacs=14.8% vs. control= 18.5%, p=0.021) and parietal region (insomniacs=13.4% vs. control=17.2%, p=0.039) than controls.
DISCUSSION
Benzodiazepine users with chronic insomnia showed impaired executive function without memory decline compared to drug-free insomniacs and controls, although they showed relatively decreased severity of insomnia symptoms. The EEG of chronic insomniacs seemed to show a hyper-arousal manifestation regardless of benzodiazepine exposure compared to controls, which had low relative theta and high relative beta power in fronto-parietal regions.
The main outcome of this study was the significant relationship between a long-term use of benzodiazepines and a decline of executive function. Our result seems to be in line with previous findings regarding cognitive function which is affected by long-term benzodiazepine use (e.g., decreased visuospatial ability, speed of processing, verbal learning, and prospective/ retrospective memory) [11,17]. In previous systemic reviews, long-term cognitive impacts of benzodiazepine in all-aged adults were associated with impairments in processing speed, divided attention, visuoconstruction, working memory, recent memory, and expressive language [34]. Another systemic review on the elderly population has reported that the process speed (examined by digital symbol test) is significantly impaired, while global cognition (examined by MMSE), memory (examined by auditory verbal test), and executive function (examined by Stroop color and word test) are not significant or show high heterogeneity throughout selected studies in benzodiazepine users than in controls [35]. These relatively different interpretations or inconsistency can be caused by different types of cognitive measurement when selecting tests by investigators in different studies. For example, Mura et al. [36] have used TMT-A and -B tests for evaluating processing speed while others selected a digit symbol test37 or a block design for the same purpose [38]. Also, one cognitive test does not always reflect one cognitive function, but involves or needs several cognitive functions at the same time. For example, the categorical verbal fluency test which consists of the production of words in a limited amount of time starting within a semantic category needs processing speed as fast as possible. It requires retrieval of the content of semantic memory, in which concepts and words are hierarchically organized by the executive function [39]. Executive function is defined as a supervisory capacity in the overall hierarchy of brain processing and encompasses skills necessary for purposeful, goal-directed behaviors [40]. It is often associated with prefrontal cortical areas. It characteristically includes processes such as goal formation, planning, initiation, preservation and alteration of goal-directed behavior, problem solving, response inhibition, and cognitive flexibility [41]. Therefore, low scores of TMT-A and categorical fluency of subjects in this study might indicate that long-term use of benzodiazepine is associated with a decline of executive function as a superordinate concept of cognition.
However, the decrease of executive function was not proportional to daily dose or cumulative dose of benzodiazepine in this study. Rather, it was associated with duration of benzodiazepine exposure and age at starting medication. Longduration of benzodiazepine exposure also means long-duration of suffering from insomnia without remission. Indeed, a remission rate of chronic insomnia was less than a half in spite of receiving benzodiazepine treatment and sleep disturbance remained and became chronic [42]. Sleep disturbance for long period could cause cognitive problems including memory and frontal lobe function [18]. An activation of the glymphatic system during sleep is associated with a brain clearance system that removes potentially toxic biomolecules such as beta-amyloid protein [43]. Brain damage caused by decreased peripheral brain-derived neurotrophic factor [44,45] has been suggested as a mechanism of cognitive decline or pathogenesis of neurodegenerative diseases. If the duration of suffering insomnia in drug-free insomniacs is much shorter than that of insomniacs using benzodiazepine, the gap of cognitive function between them would become relatively big. Speculation of a relative short duration in drug-free insomniacs not enough to change oneŌĆÖs cognitive function might be an explanation about the nodifference in cognitive function between drug-free insomniacs and controls.
In addition, decreased executive function was associated with starting benzodiazepine use at an old age. Sleep disturbances including frequent early awakening and decreased sleep quality commonly happen in elderly people and a prevalence of insomnia symptoms generally increases with age [1]. Their poor sleep parameters such as lower sleep efficiency, greater wake after sleep onset, and circadian fragmentation of sleep are potentially correlated with worsening executive function [46]. Elderly people are more susceptible to cognitive impairment caused by benzodiazepine than younger people due to their decreased overall brain capacity and increased pre-dementic lesions in the brain [47]. Benzodiazepine drugs may have more adverse effects in elderly than in adults because of decreasing drug metabolism and changing pharmacokinetics with advancing years [48]. For these reasons, FDA recommends to start zolpidem in the elderly at half the dose used for adults. When starting to take benzodiazepine at a late age, it might be important to note the decrease of cognitive function in the future.
We found no significant difference in EEG between insomnia patients who took benzodiazepine for a long time and those who did not take drugs. Both groups showed a hyperaraousal pattern of EEG compared to the control group. Attenuation of theta and enhancement of beta power can be electrophysiological correlates of sleep state misperception in insomnia such as tendency of patients to overestimate sleep latency or underestimate total sleep time relative to polysomnographic measures [49,50]. Beta and gamma activities are increased after total sleep deprivation but decreased in the morning after sleep as a restoring effect of sleep. Less theta power in insomniacs suggests a decrease in homeostatic sleep propensity [22]. Regarding the long-term effect of benzodiazepines on EEG of brain, benzodiazepine such as lorazepam generally increases beta band but decreases alpha band [51]. More relative beta activity and less relative delta/theta activity compared to controls have been found in benzodiazepine abusers during night time polysomnography [52,53]. Taken together, the hyperarousal phenomenon of the fronto-parietal area in this study might be induced by both long-term of non-restoring sleep (decreasing theta/increasing beta) and long-term of use of benzodiazepine (increasing beta).
This study has several limitations. First, it is difficult to generalize our results due to a relatively small sample size. Second, the information about total duration of insomnia among drug-free insomniacs was not collected. As total duration of insomnia could affect cognitive decline, we could not control the effect of insomnia duration on cognitive function. In addition, previous history of benzodiazepine use before starting medication at SNUBH was not included in analyses. However, it might be negligible because previous exposure of benzodiazepine was relatively short. Third, no information of objective or actual sleep time per night in all insomnia patients could limit the interpretation. The absolute sleep time may be more important to influence the decline of memory than subjective dissatisfaction of sleep [45,54]. Forth, there might be a selection bias among study participants. For example, people who remained under the benzodiazepine treatment were only those who tolerated the treatment well while people who complained any side effects of benzodiazepine might have drop-outed the follow-up. To examine and compare effect of benzodiazepines on cognitive function independently of insomnia which also affects cognition, future studies are needed to investigate and try to match several conditions such as age, severity of insomnia, duration of insomnia, and objective sleep time of study participants. The strength of this study was that the effort to adjust various variables such as depression, daytime sleepiness, and drug use history and reduce possibility of reverse causation might have contributed to increased validity of this study.
We found that executive functions of patients with insomnia after a long-term use of benzodiazepine were decreased. Long duration of insomnia and long-term use of benzodiazepine seemed to be causes of the decreased executive function. What we did not know before this study was that patients having insomnia symptoms could maintain the CNS arousal during the daytime regardless of taking benzodiazepine as long as the patient has insomnia. Novel treatment of insomnia such as cognitive behavioral therapy for insomnia, biofeedback, repetitive transcranial magnetic stimulation, light therapy, and exercise could be alternative options in addition to pharmacological intervention [55]. Nevertheless, benzodiazepine could still be one of effective and fast methods to treat severe insomnia. Thus, clinicians should take into consideration advantages and disadvantages of using benzodiazepines for insomnia treatment. When using benzodiazepines, shortening the prescription period of benzodiazepine considering patientsŌĆÖ age may help minimize oneŌĆÖs executive dysfunction.