Introduction
Panic disorder is characterized by occasional panic attacks, anticipatory anxiety and frequent development of agoraphobia. The lifetime prevalence of panic disorder is 1 to 4 percent, with 6-month prevalence approximately 0.5 to 1.0 percent, and 3 to 5.6 percent for panic attacks.1 Women are two to three times more likely to be affected than men.2 Patients with panic disorder often have comorbid conditions with other anxiety disorders and mood disorders, personality disorders and substance-related disorders.
Abnormal brain neurotransmitter regulation is implicated in the pathophysiology of panic disorder. The major neurotransmitter systems such as norepinephrine, serotonin, γ-aminobutryic acid (GABA) are involved in panic disorder. Especially, serotonergic dysfunction is quite obvious in panic disorder.3-7
Two opposing hypotheses could explain the relationship between panic symptoms and serotonergic dysfunction8: 5-HT excess or overactivity and 5-HT deficit or underactivity. 5-HT excess hypothesis suggests patients with panic disorder either have an increased level of 5-HT release or hypersensitivity in postsynaptic 5-HT receptors.9-11 On the other side, 5-HT deficit hypothesis implies 5-HT has a restraining effect on panic behavior and 5-HT deficit may facilitate panic symptoms.12 Various clinical studies have proved that postsynaptic serotonin hypersensitivity could cause increased rates of anxiety and panic attacks.11 Coplan showed that selective serotonin reuptake inhibitors (SSRIs) might exacerbate anxiety symptoms during the initial treatment due to possible oversensitivity of postsynaptic 5-HT receptors.4 However, findings of numerous studies about the anti-panic effect of 5-HT supported the 5-HT deficit hypothesis.13 Moreover, it was reported panic disorder patients gained relief after administration of 5-HT precursor, 5-hydroxytryptophan.
One of the most abundant subtypes of 5-HT receptor genes expressed in the mammalian brain is the serotonin 1A (5-HT1A) receptor. 5-HT1A receptor is known to be the major autoreceptor of serotonergic raphe neurons.14 Neumeister et al.15 reported 5-HT1A receptor binding is reduced in anterior cingulate cortex, post cingulate cortex and midbrain raphe only in panic disorder patients by analyzing positron emission tomography (PET) study. Nash et al.16 also reported reduction in postsynaptic 5-HT1A receptor binding in amygdala, temporal cortex and orbitofrontal cortex in patients with untreated panic disorder. Therefore, 5-HT1A receptor regarded as vulnerable source in panic disorder patients.
Several single nucleotide polymorphisms have been described for 5-HT1A receptor gene.16-25 Especially, Wu and Comings26 reported a C(-1019)G polymorphism in the promoter region of the 5-HT1A receptor gene. This locus is identified as C(-1019)G polymorphism because of the presence of an extra base pair in the human genome sequence of the 5-HT1A receptor gene. The subsequent study showed that 5-HT1A C(-1019)G polymorphism is located in a transcriptional regulatory region and the sequence is within a 26-bp palindrome.27 G allele and/or G/G of 5-HT1A C(-1019)G polymorphism genotype was found to be associated with major depression and suicide.14
Up to date, many studies have focused on the serotonergic system to determine the vulnerable gene of panic disorder.23-25, 27-36 However, association studies between the C(-1019) G polymorphism and panic disorder have shown inconclusive findings.37 Huang et al.21 reported no association of panic disorder with the G allele. Rothe et al.25 showed no association between C(-1019)G polymorphism and all patients with panic disorder. On the other hand, in a subsequent study, Rothe et al.25 showed significant association between the G allele and panic disorder with agoraphobia. Maron et al.32 revealed an association between the C allele and panic disorder. The recent study showed G allele associated with significantly reduced anxiety-related amygdala reactivity.38
So, we investigated if C(-1019)G polymorphism of 5-HT1A receptor could be associated with panic disorder in a Korean population. To our knowledge, this is the first study to explore the relation between 5-HT1A receptor gene and panic disorder in a Korean population.
Methods
Subjects
The study subjects recruited 110 panic patients. The diagnosis of panic disorder according to DSM-IV criteria was verified using Structured Clinical Interview for DSM-IV (SCID).39 The interviews and diagnoses were independently made by a psychiatrist without knowledge of the genotypes of subjects. Panic disorder patients who had comorbidity with mood disorders or other psychiatric disorders were excluded. Four patients with comorbid major depressive disorder were excluded. The patients who had a family history of psychiatric disorders were excluded except for anxiety disorders. Two patients who had a family history of schizophrenia and two patients had a family history of major depressive disorder. Also, the patients who had medical diseases were also excluded. Six patients with arrhythmia and one with asthma and another with thyroid cancer were excluded. Finally, this study included 94 patients with panic disorder. Concurrent agoraphobia was present in 70 (74.5%) of the patients.
We assessed the severity of the individual's symptoms using the Spielberger State-Trait Anxiety Inventory (STAI), Panic Disorder Severity Scale (PDSS), Anxiety sensitivity index (ASI), Acute Panic Inventory (API) and Hamilton's Rating Scale for Anxiety (HAM-A).
The healthy volunteers were recruited by advertisements in newspapers. They were interviewed with SCID and were questioned about their personal or family history of psychiatric disorders. Healthy controls that had a personal or family history of psychiatric disorders among first-degree relatives were excluded in this study. Some of them were excluded because of their comorbid medical conditions. Finally, 111 healthy controls were included in this study.
The mean age of panic disorder patients was 40.1±9.5 years, and the mean age of control groups was 38.3±7.3 years. There was no significant difference of the mean age between both groups (t=-1.533, p=0.127). No significant difference was found in gender distribution between the panic disorder patients (male : female=52 : 42) and healthy controls (male : female=52 : 59) (χ2=1.462, p=0.227). Age of onset of panic disorder was 37.2±9.5 years, and duration of panic disorder was 34.8±46.3 months in patients with panic disorder.
DNA analysis
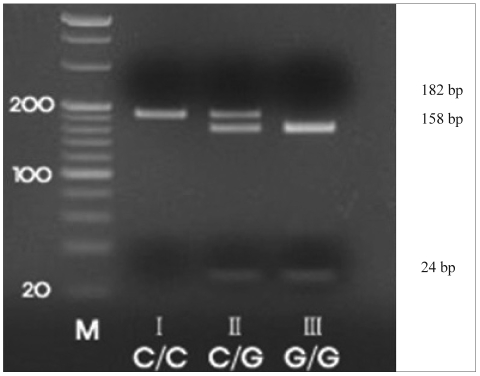
Genomic DNA was extracted from blood leukocytes by using a commercial DNA extract kit, Wizard Genomic DNA purification kit (Promega, USA). Polymerase chain reaction (PCR) was performed with the forward primer 5'-TGG AAG AAG ACC GAG TGT GTC TAC-3' and the reverse primer 5'-TTC TCC CTG AGG GAG TAA GGC TGG-3'. The amplification mixture contained 1 uL of 100 ng/uL DNA, 2.5 uL of 10x Ex Taq buffer, 2 uL of 2.5 mM Ex dNTP mixture, 1 uL primer, 18.375 uL distilled water, and 0.125 uL Taq polymerlase (TaKaRa, Japan). Samples were amplified using a Thermocycler (GeneAmp PCR system 2700, Applied Biosystems, Foster City, CA, USA) for 36 cycles. After an initial 5 min at 95℃, each cycle consisted of 45 sec at 95℃, 45 sec at 56℃, and 45 sec at 72℃. After a final 10 min at 72℃, the reaction was terminated at 4℃. The amplified DNA was digested with the restriction enzyme Hpy CH4IV (New England Biolabs), which cuts at the -1019G site, and the product was electrophoresed in 3% agarose gels and stained with ethidium bromide. Homozygous genotypes were identified by the presence of a single 182 bp band (C/C), or bands of 158 and 24 bp (G/G). The heterozygous genotype had three bands: 182, 158, and 24 bp (C/G)(Figure 1).
Statistical analysis
The presence of Hardy-Weinberg equilibrium was tested by a χ2 test for goodness of fit. Differences of clinical variables were examined with t-test. Allele and genotype frequencies in patients with panic disorder and healthy controls were evaluated using the χ2 test. Effect of genotype on symptom severity was examined with t-test, analysis of variance (ANOVA), Mann-Whitney test and Kruskal-Wallis test by comparing the mean scores of each genotype. These analyses were performed using Statistical Package for the Social Sciences (SPSS)(version 12.0; SPSS Inc., Chicago, IL, USA). The level of statistical significance was set at p<0.05. Moreover, the power analysis was performed with using of G-Power 3.1.0 computer software.40
Results
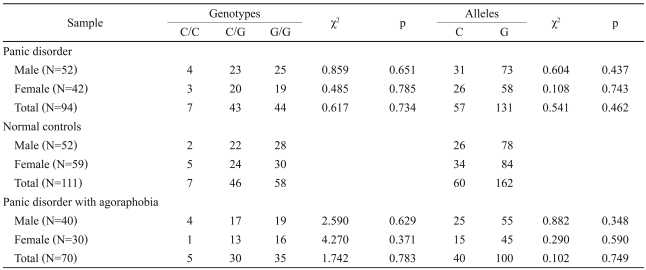
The genotype distributions in the panic disorder patients (p=0.99) and in the controls (p=0.98) were in agreement with the Hardy-Weinberg equilibrium.
No significant association between the C(-1019)G polymorphism and panic disorder was detected in either the allele frequency or genotype distribution (Table 1). There was no significant association between the C(-1019)G polymorphism and panic disorder with agoraphobia (Table 1). The C(-1019)G polymorphism had no significant differences between patients with panic disorder and healthy controls after correction of statistical differences of the gender and agoraphobia.
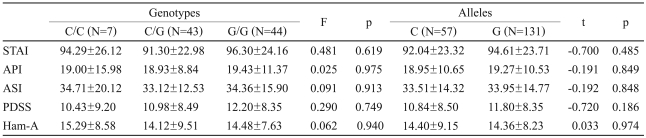
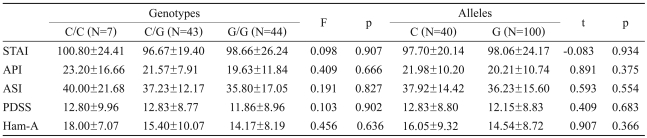
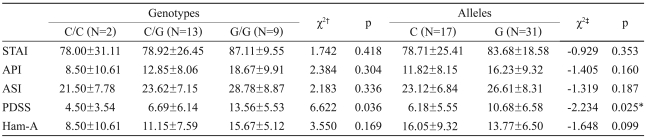
There were no significant differences of scores in panic symptom severity scales between C/C, C/G, and G/G genotype in all patients with panic disorder (Table 2) or between those in patients with agoraphobia (Table 3). However, patients without agoraphobia had significant difference of PDSS score between C/C, C/G, and G/G genotype or between C and G allele (Table 4). The PDSS scores were significantly higher in subjects with the G/G genotype for 5-HT1A C(-1019)G than in those with the C/C genotype (p=0.036). Also, patients with G allele had significantly higher PDSS score than those with C allele (p=0.025).
This study had a power of approximately 0.23 to detect a small effect, and 0.97 to detect a medium effect, and 0.99 to detect a large effect in the genotype frequencies (n=205 for total sample). When given a power of 0.95, we were able to detect an effect size of 0.28 for detecting a significant difference in genotype distributions of total panic disorder. In the allele distributions (n=410 for total sample), the study power were 0.53 to detect a small effect, 0.99 to detect a medium and a large effect, respectively. In this power analysis, effect size conventions were determined according to the method of Buchner et al.40 as follows: small effect size=0.10, medium effect size=0.30, large effect size=0.50 (alpha=0.05).
Discussion
In this study, We did not find a genetic association between the C(-1019)G polymorphism of the 5-HT1A receptor gene and panic disorder in our samples. Furthermore, no association was observed between the C(-1019)G polymorphism of the 5-HT1A receptor gene and panic disorder with agoraphobia.
Our results are consistent with previous studies. Huang et al.21 reported no association of panic disorder with the G allele. Rothe et al.25 showed no association between C(-1019)G polymorphism and all patients with panic disorder. However, Rothe et al.25 subsequently reported the association between C(-1019)G polymorphism and panic disorder with agoraphobia and indicated a significant excess of the G allele in patients with panic disorder with agoraphobia. Nevertheless, that association was regarded as a false positive because the agoraphobia subgroup was made from a consequence of population stratification or multiple testing could not be excluded.25
On the other hand, Maron et al.8 reported an association between the C allele and panic disorder. However, this study regarded panic disorder as comorbidity to affective disorders and did not excluded subjects with comorbid affective disorder. Therefore, this study did not reveal an association between C allele and panic disorder in the strict sense.
Our finding of the negative association between C(-1019)G polymorphism and panic disorder corresponded to those from Inada's study.29 In Inada's study, other locus of 5-HT 1A receptor gene, 294G/A polymorphism, had been examined and there were negative associations in Japanese population.29 Therefore, these findings suggest that there is no association between the 5-HT1A receptor gene polymorphism and panic disorder in non-Caucasian people.
In this study, we found a significant difference of symptom severity between C/C, C/G, and G/G genotype or between C and G allele in our panic disorder patients without agoraphobia. PDSS showed significant higher score in subjects with G allele in panic disorder without agoraphobia. Yoon et al.36 reported the association between the severity of panic symptom and the 5-HT 2A receptor 102T/C and 1438A/G gene. These findings suggest that gene related serotonin system of panic disorder could be explained by vulnerability or severity of panic disorder. One could not yet find exactly associated candidate loci of serotonin related gene because the actual susceptibility locus is within very small area.38
Compared to previous Caucasian studies,21,25,41-44 our results showed that the frequency of the C allele portion was much lower than that of the G allele portion in both panic disorder groups and normal control groups. Such allele distribution might be different from ethnic variability.
There were some limitations in this study. First, the sample size in our study was not sufficient to analyze the association for the subgroups of panic disorder. It is increasingly clear that very large samples are needed to detect robust associations given the modest effect sizes of individual susceptibility loci. As a result, it was likely that our studies was underpowered, raising the risk of false negatives as well. Although we showed a significant association between panic symptom severity and 5-HT1A receptor gene C(-1019)G polymorphism in patients without agoraphobia, the difference is modest and cannot survive correction for multiple comparisons. Therefore, studies of a larger sample of panic disorder are needed to clarify the role of the C(-1019)G polymorphism of the 5-HT1A receptor gene as a risk factor for panic disorder. Second, we examined only one locus of the 5-HT1A receptor gene polymorphism. To get clear data about 5-HT1A receptor gene polymorphism and panic disorder, we should do examined multiple loci related gene in greater sample size of panic-disorder patients in the future. Third, all the patients were evaluated in baseline. Because the patients were under medication, there is room for confounding factor in estimating severity evaluation and needs to be adjusted by medication condition.
In conclusion, we found no association between 5-HT1A receptor gene polymorphism and panic disorder in Korean population. The C(-1019)G polymorphism is possibly a weak candidate that will contribute in establishing the relationship between 5-HT1A receptor gene and panic disorder. Further studies need to evaluate different SNPs in different ethnic groups of panic-disorder patients to clarify the role of the serotonergic receptor gene variant as a risk factor of panic disorder.