INTRODUCTION
Probation is a criminal policy and measure to promote rehabilitation within society and to prevent recidivism. Those on probation live as others do in society, while being supervised and supported by probation officers, crime prevention committees, or community services to correct delinquent and criminal behavior. Thus, probation eliminates the need to detain these offenders and restrict their freedom in correctional institutions. The ultimate purpose of probation may be not only to reduce costs associated with the detention of offenders and to prevent the sequelae of crimes, but also to prevent recidivism via systematic, professional supervision and avoid severance from family, school, and the workplace, which then minimizes impacts on human rights and promotes smooth social adjustment.1
In South Korea, 12 probation offices and 6 branch offices nationwide were established on July 1, 1989, to offer probation to young offenders. Coverage was later expanded to include the probation of sex offenders, adult criminals, and domestic violence offenders. Currently, 16 probation offices and 40 branch offices nationwide offer probation for 200,000 or more offenders.2
Individuals on probation are known to experience a higher prevalence of mental illness compared to the general population. In England and the United States, 39% and 27%, respectively, of those on probation had mental health problems.34 Other research has indicated that depression, anxiety, and drug abuse were the most frequent mental health problems among those on probation.56
The association between mental illness and crime has long been the subject of social attention. The deinstitutionalization of mental patients and changes in community-based treatment improved individual patients' self-regulation; however, it has led to their increased interaction with the criminal justice system.7 Existing research in the United States reported that 8 to 29% of prisoners had a mental illness that could result in substantial functional impairment and another 15 to 20% required psychiatric intervention during detention.8910
One study that systematically analyzed 62 reports from 12 nations (western countries) found that 3.7% of male prisoners were diagnosed with psychotic disorders, 10% with major depression, and 65% with personality disorders (47% with antisocial personality disorder); 4.0% of female prisoners were diagnosed with psychotic disorders, 12% with major depression, and 42% with personality disorders (21% with antisocial personality disorder). Compared with the general American.1112 or British13 population of similar age, prisoners have about a two-to-four-fold rate of psychotic illnesses and major depression. In particular, the prevalence of antisocial personality disorder was almost ten times greater than the prevalence in the general population.14 A recent study reported that the prevalence of adult attention-deficit hyperactivity disorder in long-term prisoners reached 40%.15
In South Korea, although the number of offenses committed by individuals with mental illness has been low for the last decade, the number of offenses committed by individuals with mental illness rapidly increased to around 9,000 cases in 2004 after 3,600 cases in 2000.16 The upturn has continued since then, with between 5,000 and 7,000 cases each year. The proportion of violent crimes among those committed by individuals with mental illness increased from 9.8% in 2000 to 30.8% in 2011. Murder (7.5%) and arson (7.9%) showed the highest proportions among crimes committed by those with mental disorders in 2014; thus, the severity of crimes committed by these individuals has been seen as increasing significantly.16
According to a report using national statistics in 2012 by the Supreme Prosecutor's Office on first offenses compared to recidivism in offenders with and without mental illness, the ratios were 1,816 out of 5,379 cases (33.8%) and approximately 440,000 out of 1,900,000 cases (23.3%), respectively, indicating that the proportion of first offenses was higher for those with mental illness.17 Based on a crime analysis by the Supreme Prosecutor's Office in 2013, 65.7% of criminals with mental illness had one previous conviction while 17.0% had nine or more convictions; these proportions were higher compared to those for offenders without mental illness (41.7% and 8.5%, respectively).18 Thus, chronic recidivism among offenders with mental illness is considerably high.
In this context, the rate of recidivism should not be regarded as a personal issue. In order to achieve the ultimate purpose of probation-social adjustment and prevention of recidivism among offenders-greater institutional and systematic interventions from a mental health and medical perspective may be required.
The study purpose was to investigate the prevalence of mental illness among adults in South Korea who use probation offices and to analyze prevalence rates based on first and repeat offenses. The aim was to provide evidence for the effective prevention of recidivism.
METHODS
Participants and procedures
Study participants were 206 adults on intensive, major, and general probation who visited the probation office in Seoul between August 6 and November 19, 2014, and who provided voluntary, informed consent. Those sentenced to their first probation were classified into the first offense group, while those who had been on probation two or more previous times were classified into the recidivism group.
Participants answered a self-report questionnaire (including demographic information) and underwent a clinical interview. These were conducted using a structured clinical interview form for diagnosing mental illness composed by psychiatrists and clinical psychologists specifically for this study.
This study was approved by the Institutional Review Board of Inje University Sanggye Paik Hospital (IRB FILE No. SGPAIK 2015-03-010) and was performed in accordance with the ethical standards of the 1964 Declaration of Helsinki and its later amendments.
Measurement instruments
Korean version of the Mini-International Neuropsychiatric Interview (MINI)
The MINI is a diagnostic tool for mental illness for use during structured interviews. The current version (MINI 5.0.0) was developed to diagnose Axis I disorders based on the DSM-IV and ICD-10 criteria.19 The interviewer read the MINI questions to the respondent who answered ŌĆ£yesŌĆØ or ŌĆ£no.ŌĆØ Then, the MINI algorithm is used to reach a diagnosis based on the responses. Disorders that can be diagnosed by the MINI include major depressive episode, dysthymic disorder, manic episode, panic disorder, agoraphobia, social phobia, obsessive-compulsive disorder, post-traumatic stress disorder, alcohol dependence, schizophrenia, delusional disorder, generalized anxiety disorder, somatoform disorder, and adjustment disorder. A previous South Korean study investigating clinical diagnoses by psychiatrists and the Korean version of the MINI showed that the consistency of most diagnoses was sufficient.20
Diagnostic criteria of Diagnostic and Statistical Manual of Mental Disorders-5 (DSM-5)
The DSM-5 presents criteria for the classification and diagnosis of mental disorders by the American Psychiatric Association.21
In this study, the author used the diagnostic criteria of the DSM-5 for gambling disorder and Internet gaming disorder to investigate the prevalence of these disorders among individuals on probation.21
Adult ADHD Self-Report Scale (Version 1.1)
This was developed based on the DSM-IV diagnostic criteria for attention deficit hyperactivity disorder (ADHD) by the World Health Organization (WHO).22 In this study, six of the scale's questions that are known to best predict ADHD symptoms were used.22 The frequency of experiencing symptoms for the last six months was measured for each question, and words or phrases aimed at adults were used (i.e., words such as play and school were excluded).23
Statistical techniques
Data were analyzed using SAS 9.2 (SAS Institute Inc., Cary, NC, USA). Regarding statistical significance, the chi-squared test was conducted with a 95% confidence level. When 25% or more of the data had expected frequencies of less than five, the Fisher's exact probability test was used for analysis.
RESULTS
Probation frequency
In total, 206 individuals were on probation and agreed to participate; 202 described their history of probation (4 were excluded because they didn't respond). Among these 202 individuals, most were on their first probation (63.86%). Repeat offenders accounted for 73 individuals (36.41%), and proportions for those with previous probations were as follows: 2 (16.83%), 3 (8.42%), 4 (7.92%), and 5 (2.97%) times.
Sociodemographic distribution
The average age of the participants on probation was 39.13 (┬▒12.30) years for the first offense group and 41.88 (┬▒11.65) years for the recidivism group; there was no statistically significant difference between the two groups. The proportion of males (82.9% for the first offense group and 87.7% for the recidivism group) was significantly higher than that of females (17.1% and 12.3%), but the sex ratios were statistically similar between the two groups. Regarding the participants' education level, 43.3% of the first offense group and 23.6% of the recidivism group had at least 12 years of education, indicating that the education level of the first offenders was significantly higher (p=0.021). The proportion of those living alone was slightly higher in the recidivism group (26.1%) compared to those in the first offense group (19.8%), but the difference was not statistically significant. Household income was similar between the two groups (Table 1).
Mental health prevalence
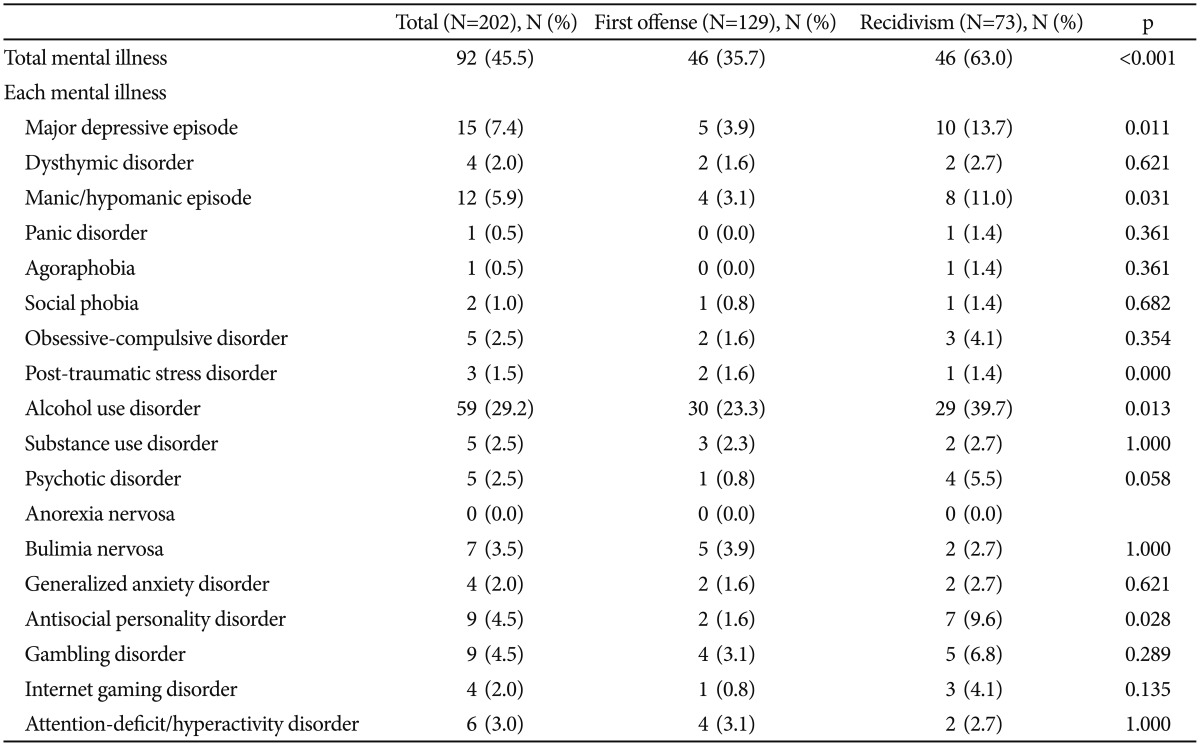
The prevalence of mental illness was 35.7% in the first offense group and 63.0% in the recidivism group; this is a statistically significant difference (p<0.001); the most common disorder between the two groups was alcohol use disorder (23.3% and 39.7%, respectively). The next most frequent disorders in the first offense group were, in order, major depressive episode (3.9%), bulimia nervosa (3.9%), manic/hypomanic episode (3.1%), gambling disorder (3.1%), and ADHD (3.1%), while those in the recidivism group, in order, were major depressive episode (13.7%), manic/hypomanic episode (11.0%), antisocial personality disorder (9.6%), and gambling disorder (6.8%).
When comparing prevalence rates between the two groups, major depressive episode (p=0.011), manic/hypomanic episode (p=0.031), alcohol use disorder (p=0.013), and antisocial personality disorder (p=0.028) showed statistically significant differences. All disorders showed higher prevalence rates in the recidivism group compared to those in the first offense group (Table 2).
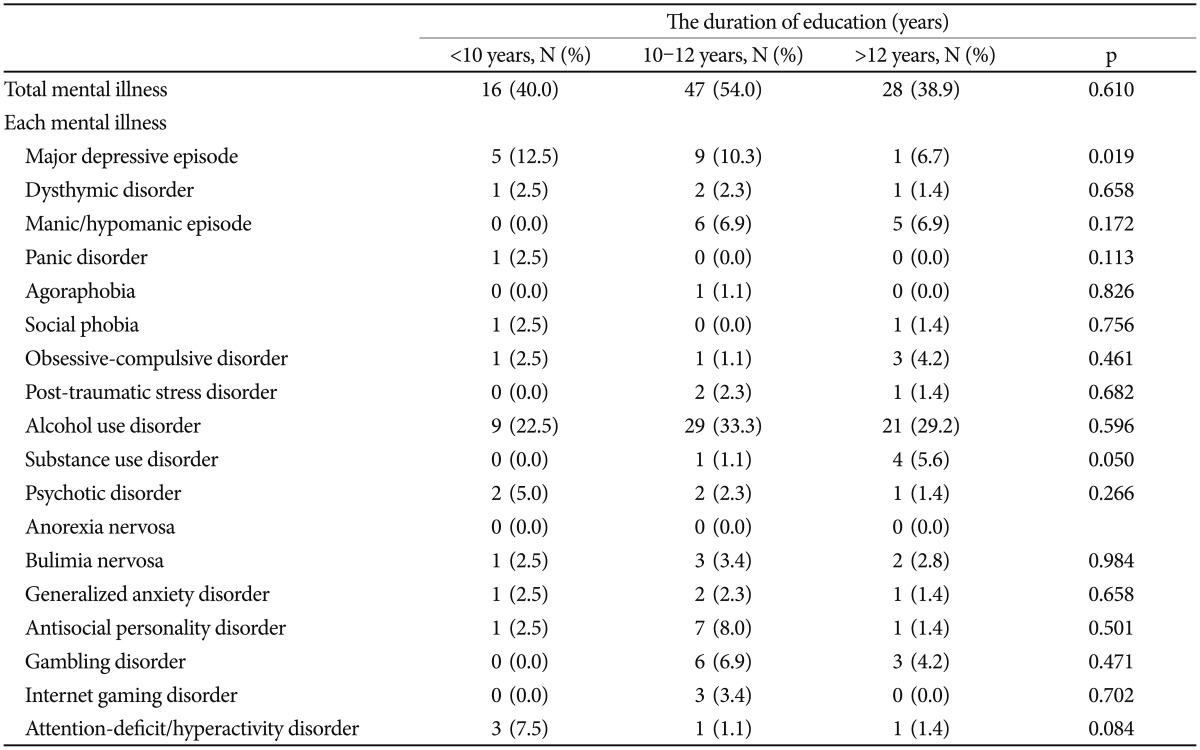
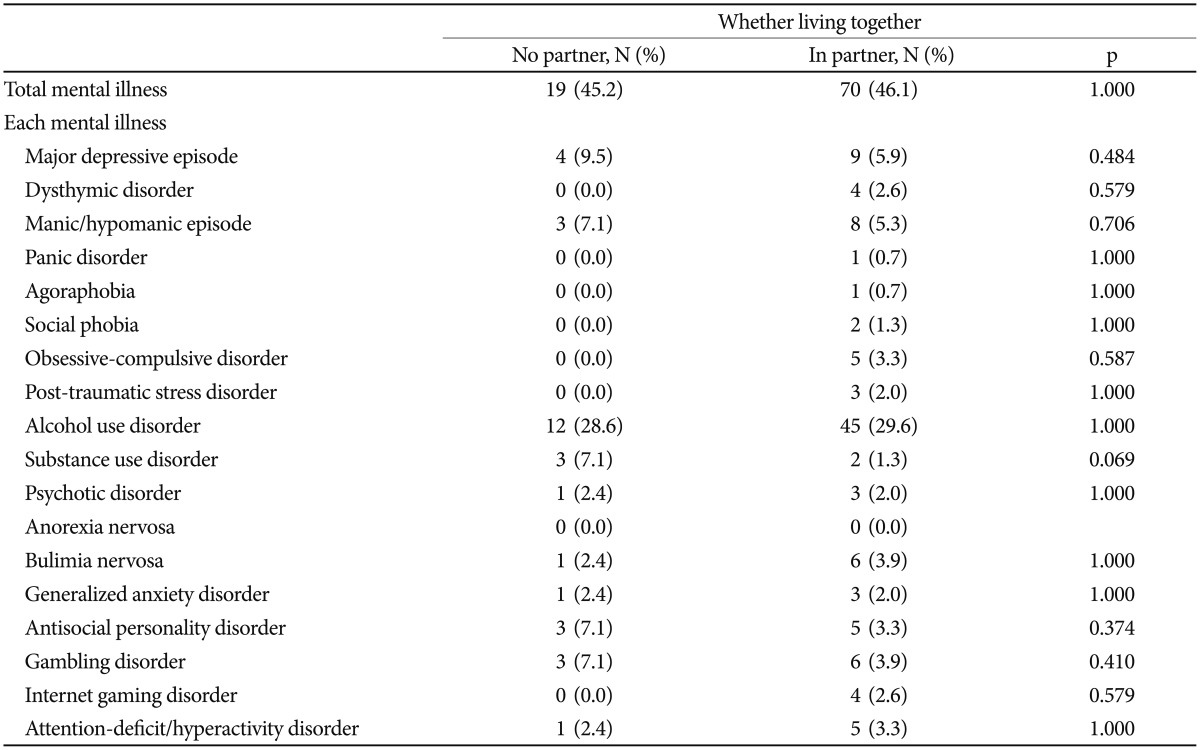
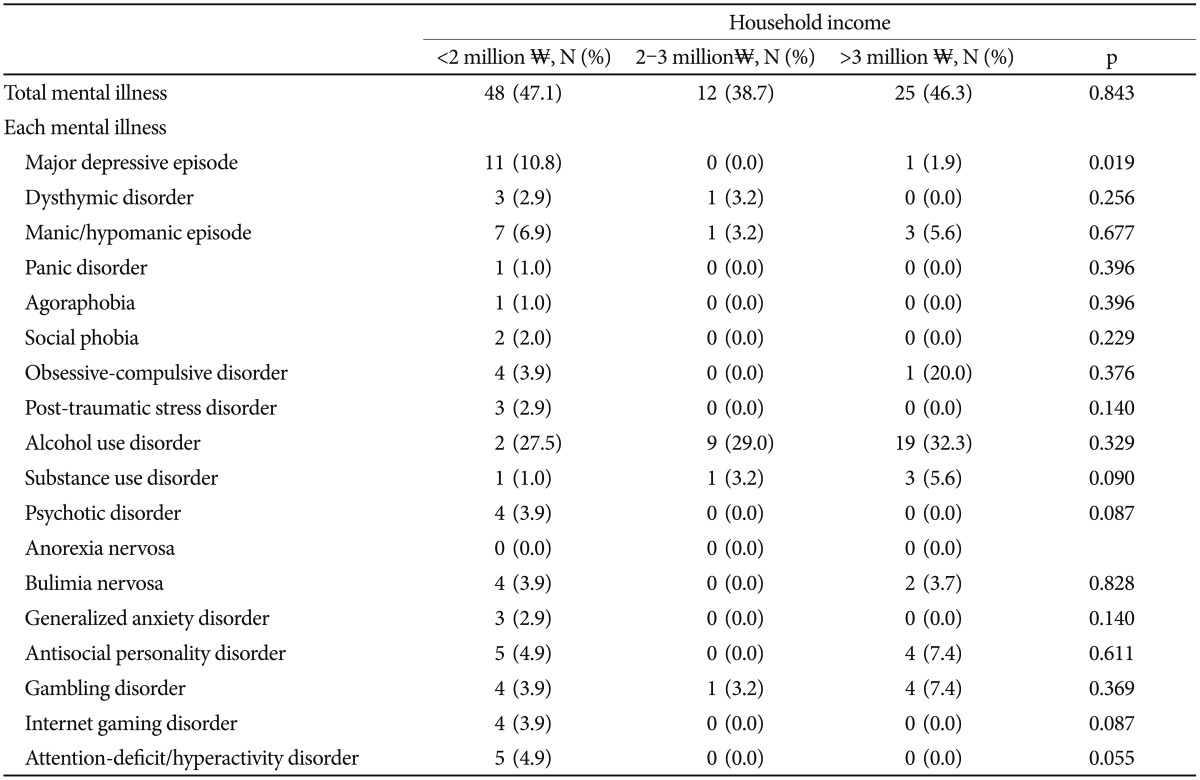
In order to additionally identify the association between sociodemographic factors and mental illness, the author analyzed relationship of mental illness with education, presence of domestic partners, and household income among the collected sociodemographic factors of the subjects (Table 3, 4, and 5). Among the types of mental illness, major depressive episode showed significant relationship with education (p=0.019) and household income (p=0.019), while presence of domestic partners was not associated with mental illness.
DISCUSSION
In this study, 202 adults on probation for first offenses or recidivism were investigated regarding their sociodemographic distribution and mental health prevalence. Additionally, the association between recidivism and mental illness was analyzed.
Overall, 71.43% of participants had less than 3,000,000Ōé® (KRW, Korean Won) of monthly household income. As the average income of the second-lowest bracket was around 2,900,000Ōé® in the income quintile statistics of domestic households for the first quarter of 2015,24 the financial situation of those on probation was generally poor. The proportion of those who finished high school education was 36.87%, which is relatively lower compared to South Koreans in 2012 (42%).25 A considerable number of those on probation were in a vulnerable social class, and might have experienced difficulty receiving appropriate medical benefits, including mental health care.
In this study, a significant difference was shown for education level between the first offenders group and the recidivism group (p=0.021). Because people with more education tend to accept social conventions and norms more easily,26 education level may have affected recidivism. This finding is supported by research showing that prisoners with higher education levels showed lower recidivism rates27 and a Korean study reporting that lower educational levels promoted recidivism.28
In this study, the prevalence of mental illness was 45.63% (males=46.82%; females=39.39%). This percentage is considerably higher when compared to the South Korean general population; the lifetime prevalence in the general population is 27.6% (males=31.7%; females=23.5%).29 As the prevalence reported for the general population is the full lifetime, the actual differences between the general population and study participants may be greater than reported. Mental illness prevalence for the first offense group and recidivism group was 35.7% and 63.0%, respectively, with a statistically significant difference between the two groups (p<0.001), indicating that mental illness might affect not only criminal actions but also recidivism.
Regarding individual illness, the prevalence of alcohol use disorder (29.13%) was remarkably higher than that of the general population (13.4%), and mood disorders (major depressive episode, bipolar disorder, and dysthymic disorder) was 34.04%, around five times greater than that of the general population (7.5%).29 Alcohol use disorder, major depressive episode, manic/hypomanic episode, and antisocial personality disorder showed significant differences in prevalence between the first offenders group and the recidivism group (p=0.013, p=0.011, p=0.031, and p=0.028).
Alcohol-related problems showed the highest prevalence among the mental illness of participants and affected recidivism, clearly suggesting a relevance to crime. According to a previous study of offenders on probation in South Korea, 29.9% said that their probation was partially related to drinking, and 22.1% indicated a direct relationship. However, only 7.4% of respondents intended to receive counseling for their drinking problem.30 Because Korean culture is relatively accepting of drinking as a tradition, alcohol problems are regarded as an individual illness or a problem of personal will, not a wider social issue.31 This social context may be responsible for the insufficient recognition of the need for professional treatment for alcohol problems, and more systematical treatment services via national policy may be required.
Manic/hypomanic episodes have been a factor in crime historically. The grandiose perceptions, reduced reality testing, impulsiveness, overactivity, and psychotic symptoms of patients with bipolar disorder who experience manic/hypomanic episodes make them vulnerable to antisocial activities.32 A population-based, longitudinal study found that bipolar disorder was associated with violent crimes and risk was higher when accompanied with substance use disorder.33 In the same context, antisocial personality disorder itself is likely to be a factor of crime.34
In this study, major depressive episodes seem to be a factor in crime. There are a number of potential reasons for major depressive episodes showing a higher prevalence in the recidivism group. First, irritability caused by a depressive episode may serve as a factor in crime. Although irritability is included in the diagnostic criteria of the DSM-5 only for young children and adolescents, a considerable number of adults experiencing major depressive episodes show irritability.35 In contrast, crime may also cause major depressive episodes. Legal sentencing may act as a stressor for individuals and repeated sentencing may deepen depression.
When the author additionally analyzed whether sociodemographic factors were associated with mental illness by using information of the factors collected from those on probation in this study and of mental illness, the ratio of major depressive episode of the subjects was reduced more as education years were longer and income level was higher, with statistically significant level (p=0.019 and p=0.019). These results may be significant in such a way that major depressive episode can serve as a factor enabling policy intervention, given that the episode affects recidivism. However, most of the rest of mental illness did not show association with sociodemographic factors and the absolute values of illness of the subjects were low, indicating limitations in interpretation.
This study is significant in that adults on probation voluntarily participated, the prevalence was investigated by psychiatrists, the results of various previous studies were repeated, and the association with individual illnesses was identified. However, there are some study limitations. Among the participants, 83.8% were male. The sex ratio between the first offense group and the recidivism group was similar; however, as sex affects the prevalence of mental illness, the study results may be difficult to generalize to both males and females. There are 200,000 or more offenders and 16 probation offices in South Korea. The sample size is small compared to the national population of probationers. Additionally, the study sample recruitment was undertaken using only one probation office; therefore, they may not be representative of South Korean probationers. Because this study investigated point prevalence rates, it is unclear whether crime is followed by mental illness. As mentioned, it is possible that major depressive episodes may be caused by crimes, and thus it is difficult to establish causal relationships between mental illness and crime. It is clear, however, that the participants on probation were in vulnerable sociodemographic groups and showed higher mental illness prevalence rates. Additionally, a clear difference in prevalence rates existed between the first offense group and the recidivism group. Thus, the study results may be sufficient to indicate the need for systematic mental health services for those on probation. Last, the association between mental illness and type of crime was not analyzed in this study. This may require further research to identify appropriate methods of psychiatric intervention based on the type of crime.
Adults on probation are expected to be in a vulnerable social class and have a higher prevalence of mental illness. As mental illness may affect re-sentencing probation, or recidivism, institutional intervention on a mental health or medical basis may be necessary to achieve the ultimate purpose of probation.