INTRODUCTION
Suicide in Korea
Currently, South Korea’s suicide rate is the highest among Organization for Economic Cooperation and Development (OECD) countries. In 2017, Korea’s suicide rate was 24.3 cases per 100,000 population, which is about twice the OECD average [1]. Of particular importance is that suicide rates per 100,000 positively relate to age: 70.0 among those aged 80 or older, 48.8 among those aged 70-79, and 30.2, 30.8, 27.9, 24.5, and 16.4 among those aged 60-69, 50-59, 40-49, 30-39, and 20-29, respectively [2].
Risk factors of suicide
Suicidal ideation (SI) is more strongly related to completed suicide among older persons than younger, because older persons employ methods that are more likely to be fatal, such as firearms, drowning, and suffocation [3-5]. SI is a key independent predictor of completed suicide [6]; preventing SI is therefore considered one of the most effective ways to prevent suicide completion, and is a key aspect of the suicide intervention process [7]. Previous studies have identified various factors that increased the risk of SI among older adults, including physical health [8-12], psychological health [13,14], stress/distress [12,15,16], financial concerns [12,17], social networks, satisfaction with social support, and loneliness [18-20] and socio-demographic characteristics [21-23]. Among various risk factors of SI, physical and psychological illness have been noted as significant predictors of SI in many previous studies [8-14]; these factors are especially related to older adults, because their health condition might be worse than for other age groups. In addition, a policy to find high-risk suicide groups in Korea, has focused on depression among the elderly and an increase in the number of older adults living alone [24]. In other words, mental problems such as depression and stress in the elderly can be expected to be closely linked to suicide. Therefore, it would be necessary to identify associations of SI with self-rated health, and mental health-related variables such as self-rated stress and depression.
Depression and suicide risks
Previous studies showed divergent results on the relationship between depression and suicide. First, Goldney [25] reported that the prevention of seasonal depression has dramatically reduced suicide mortality as shown after performing a psychological autopsy on all suicide deaths in Finland. According to the report from the U.S department of Health and Human Services, about 60 percent of people who committed suicide had a mood disorder (e.g., major depression, bipolar disorder, dysthymia) [26]. Contrary to the aforementioned findings from previous studies, Joo et al. [27] reported that depression disorder was not significantly associated with suicidal ideation, and rather than stress, difficulty concentrating and social isolation were significantly associated with suicidal ideation among 753 adults living in the U.S. Furthermore, according to another survey conducted in the U.S., two-thirds of older Korean Americans without minor or major depressive disorder (diagnosed by the Korean version of the Patient Health Questionnaire) reported SI (64.0%), which was higher than the proportion of those with comorbid SI and depressive disorder (36%). Overall, based on the literature review, we hypothesized that even though depression may be a risk factor, a large proportion of older adults who were not diagnosed with depression might be at suicide risk.
Health-related quality of life (HRQoL)
Previous studies found that low levels of HRQoL strongly influenced SI, particularly among older adults who had the lowest score scope on the EQ-5D by EuroQoL (<0.7) and whose likelihoods of SI and SA (Suicidal Attempt) were higher than those of older adults with higher scores [28,29]. Some studies on the relationship between HRQoL and suicide in Asian samples focused on older adults [30,31]. Previous studies have examined how HRQoL affects SI and SA however, little is known about how the five dimensions of HRQoL associated with SI. Here, we aimed to systematically investigate the interplay of various HRQoL indicators and predictors of SI in older adults.
We hypothesized that the five HRQoL dimensions (EQ-5D) would be critical independent predictors of SI. These dimensions cover a broad range of individual-level health characteristics, such as functional ability, emotional state, and overall health measured using self-report items assessing expectations and achievements [32].
The study objectives were as follows:
1) Identify the socio-demographic characteristics of older adults with and without SI.
2) Assess the proportions of older adults with and without depression in the SI group.
3) Analyze the proportions of predictors for SI among the four groups based on the presence/absence of SI and depression.
4) Investigate the strength of the associations between the hypothesized predictors and HRQoL with SI by performing a multiple logistic regression analysis.
METHODS
Sample
The data used in this study were derived from the Korea National Health and Nutrition Examination Survey (KNHANES V, VI, and VII; 2012-2016), a nationally representative cross-sectional survey conducted by the Korean Centers for Disease Control and Prevention and the Ministry of Health and Welfare. This survey targeted non-institutionalized Korean individuals; respondents were selected to represent the Korean population using complex sampling with a stratified, clustered, and multistage probability design. In addition, this survey is based on a rolling sample survey method, which divides the entire country into 192 clusters and targets an average of 20 households per cluster to ensure the representativeness of the collected data. Selected participants received a notice of selection before data collection began, and written informed consent was obtained after receiving information on the survey’s purpose. This study was conducted with approval from the Catholic Medical Center’s Research Ethics Committee (IRB No. MIRB-20190719-001).
Of the 39,156 respondents to the KNHANES in 2012-2016, 7,807 individuals aged 65 or older were included in the initial sample. Of them, we excluded 543 individuals who did not respond to the question on SI and 491 individuals with missing data on other important variables, yielding a sample size of 6,773. Respondents with missing data on HRQoL (n=1,169) were also excluded; thus, the final sample comprised 5,604 respondents (participation rate=71.8%) aged 65 years or older with complete data on the analysis variables.
Variables
Dependent variable: SI
SI was assessed using the response to the following question: “Have you ever thought about committing suicide during the past 12 months?” The response options were “yes” or “no.” The respondents who answered “yes” were assigned to the SI group; those who responded “no” were assigned to the no-SI group. This was the primary question to verify the suicidality of respondents. Two other related questions were asked, namely “Have you ever made a plan to commit suicide during the past 12 months?” and “Have you ever attempted to commit suicide during the past 12 months?” If respondents answered ‘no’ to the first question, they might respond ‘no’ to the rest of two questions.
Risk factors and control variables
The KNHANES assesses mental health status (regarding depression, stress/distress, and counseling used for psychological problems) and physical health (including self-reported status). Depression was diagnosed by clinicians. Stress/distress was assessed using subjective self-rating; the question, “How much stress do you feel in your daily life?” was answered on a 4-point Likert-type scale (1=very high, 2=high, 3=moderate, 4=minor). Counseling received during the past year was measured using the question, “Have you received counseling within the past year due to your psychological problems?”; the response options were “yes” or “no.” Self-rated physical health status was assessed with the question, “How do you rate your physical condition?”; responses were provided on a 5-point Likert-type scale (1=very good to 5=very poor). Data on age, gender, educational level, marital status, and financial status were collected as control variables [9,12].
HRQOL
The KNHANES includes the Korean version of the EQ-5D by EuroQoL group [33] to measure HRQoL. The EQ-5D is among the most widely evaluated HRQoL measures [34] and comprises five dimensions: physical activity, self-control, daily activity, pain, and anxiety/depression, each rated based on three grades of severity: no problems, some problems, and severe problems. Previous studies found that the Korean version of the EQ-5D was valid and stable over time [35-38]. In this study, the scores on the five EQ-5D dimensions were summed to provide an index following the recommendation of the Korean Centers for Disease Control and Prevention [39,40]. This makes it possible to convert each score of the five dimensions into a single score. Details about this calculation are provided in Supplementary Material (in the online-only Data Supplement).
Statistical analysis
First, differences in socio-demographic characteristics between the SI group and NoSI group, as well as any differences in psychological health, physical health, and the five EQ-5D dimensions between the four SI/depression groups were evaluated using a chi-square test. The four subgroups were: 1) SI with depression (“SI-Depression”), 2) SI without depression (“SI-NoDepression”), 3) no SI with depression (“NoSI-Depression”), and 4) no SI with no depression (“NoSI-NoDepression”). Then, a binomial multiple logistic regression analysis was used to calculate the odds ratios (ORs) and 95% confidence intervals (CIs) of the effects of the five EQ-5D dimensions, psychological health, and self-rated physical health on SI. SAS (ver. 9.2; SAS Institute, Inc., Cary, NC, USA) was used to perform all the statistical analyses, which employed sampling weights for nationally representative prevalence estimates.
RESULTS
Socio-demographic characteristics of SI group and no-SI group
In Table 1, about 11.5% (n=640) of the respondents reported experiencing SI, and 88.5% (n=4,964) of the respondents reported that they had not experienced SI during the past year. Twice as many women as men reported experiencing SI. More than half of both the SI group (n=395, 61.7%) and no-SI group (n=3,194, 64.0%) were in the youngest age group (65-74 years), and the age distribution was not significantly different between the groups. Regarding education, elementary school graduate was the most common in both groups (SI: n=483, 74.6%; noSI: n=2,985, 61.5%), but there were about twice as many college graduates in the no-SI group as in the SI group (8.7% and 4.4%, respectively), and this difference was significant (p<0.0001). There was also a significant difference in both groups’ monthly income, with almost two-thirds (n=405, 65%) of the SI group and less than half (n=2,289, 46%) of the no-SI group falling under the low monthly income category. The proportions of widowed (n=264, 42.6%) and divorced (n=43, 7.5%) respondents in the SI group were significantly higher than in the noSI group (widowed: n=1,432, 30.7%; divorced: n=167, 3.1%). There were no differences in employment rates between the two groups (Table 1).
Five dimensions of EQ-5D by group
Table 2 shows the distribution of the EQ-5D dimension categories [“problems” (including both “some” and “severe problems”) or “no problems”], EQ-5D index categories (range: <0.70 to 1.0), and mean index in the SI and no-SI groups with and without depression. About 20% (n=128) of the SI groups received a psychiatric diagnosis of depression, and about 5.8% (n=291) of the no-SI groups had depression. A pattern emerged regarding EQ-5D indicators in which the highest proportion of those having problems was in the SI-Depression group, followed by the SI-NoDepression group, NoSI-Depression group, and NoSI-NoDepression group. The results regarding EQ-5D, psychological, and physical health in the NoSI-NoDepression group were considered usual for adults aged 65 and older and, since this group had neither SI nor depression, it was used as the reference group.
Within the SI group, those with depression were more likely to have HRQoL problems than those without depression, considering the results on the five EQ-5D dimensions. Interestingly, 47.6% (n=241) of participants who were not diagnosed by a physician in the SI-NoDepression group reported anxiety/depression problems on the EQ-5D. This was higher than in the NoSI-Depression group (n=133, 40.3%). In total, the proportion of participants in the SI-Depression group that reported problems was higher than that in the other three groups for all five EQ-5D dimensions. In particular, there were significant differences in anxiety/depression between the SI-Depression (n=94, 70.1%) and SI-NoDepression (n=241, 47.6%) groups (p<0.0001), and in physical activity problems between the SI-Depression (n=91, 72.2%) and SI-NoDepression (n=324, 60.1%) groups (p<0.0001). Regarding the EQ-5D index, there were significant subgroup differences. The group with the highest proportion of participants with the lowest index level (<0.7) was the SI-Depression group (n=56, 44.9%), followed by the SI-NoDepression group (n=162, 28.8%). At the highest index level (1.0), the SI-Depression group showed the smallest proportion (n=10, 8.1%), followed by the SI-NoDepression group (n=92, 17.5%) (Table 2).
Stress and physical health differences between groups
About 51% (n=327) of respondents in the SI group reported either “very high” or “high” stress, which was significantly higher than the 15% (n=745) reported by the no-SI group. The SI-Depression group was more than four times as likely as the reference group to report very poor physical health (34.5% vs. 8.2%); the SI-NoDepression group was similar (n=166, 31.6%). In contrast, just 11.5% (n=35) of the NoSI-Depression participants considered their physical health to be very poor. About half of each subgroup reported having received no psychological counseling.
The association of EQ-5D, depression, and self-rated physical health with SI
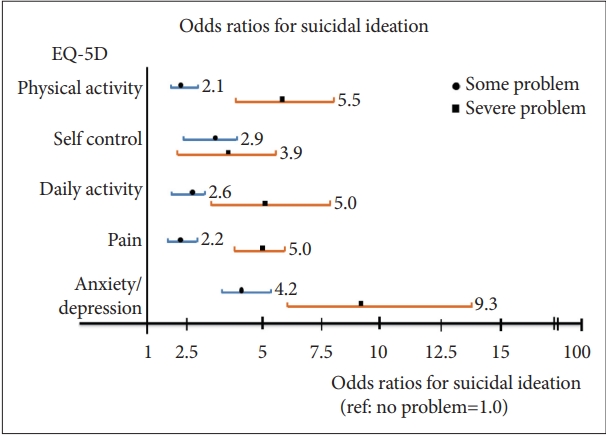
Table 3 shows the analysis results of the four predictors in the adjusted multiple logistic regression model. Self-control, anxiety/depression of EQ-5D, self-rated physical health, and depression scores showed significant association with SI (p< 0.0001). The effects of age, gender, educational level, monthly income, marital status, and financial concerns were controlled for in the final model. Figure 1 illustrates how strongly associated the EQ-5D responses were with having SI (“some” versus “severe” problems). The respondents who reported “severe” problems had twice the risk of SI as those who reported “some” problems. The highest odds ratio was found for EQ-5D anxiety/depression (OR=9.3, CI=6.07-14.35).
DISCUSSION
This study found that older adults with SI had significantly lower HRQoL than those without SI. This was demonstrated by the higher proportions of respondents with SI who reported problems on all five EQ-5D dimensions compared with the no-SI group. The differences in self-control and anxiety/depression were particularly large, with HRQoL being significantly lower on these dimensions among the respondents with SI.
About 11.5% of the sample of older Koreans reported SI, which was more than twice the prevalence found in studies of community-dwelling older adults in the United States (5.4%) [41], Japan (5.6%) [42], or Australia (4.5%) [16]. However, our result was lower than the 14.7% incidence of SI observed in a sample of older Korean Americans [43], and the 14.5% incidence of SI among older adults in a rural Chinese community [14]. Previous studies have found that some socio-demographic characteristics were significantly associated with SI, which was supported by our findings. We found that SI was more likely among females [42], those with lower income [29,32,42] and those who had lower education levels [29], which are known contributors to SI among older adults. We focused on the fact that physical and psychological health can be particularly vulnerable among the older adults who were targeted in this study [24]; thus, we aimed to identify the association of SI and HRQoL which makes it possible to identify both self-rated physical and psychological health level. To the best of our knowledge, this is the first study to analyze the association of SI and each dimension of EQ-5D. This study found significant associations between each dimension of EQ-5D and SI. Therefore, the response results of EQ-5D need to be considered as significant predictors of SI.
A variety of factors associated with SI
The current study found that in the SI group, the proportion of respondents without depression was almost four times as high as the proportion of those with depression, which addresses the second aim of our study. The main finding of this study was that only 20 percent of older Korean adults were diagnosed with depression in the SI group, which is an interesting result. However, the following limitations need to be considered. First, this number was based on an interview about whether participants were diagnosed with depression by clinicians, and it was not possible to identify how the depression diagnosis was made or whether it was diagnosed by psychiatrists/psychologists or not. Second, there is the potential that the symptoms or characteristics of depression were not clearly revealed through clinical interviews even though depression had been diagnosed by psychiatrists/psychologists in the hospital. In addition, respondents may not have recognized a mental disease such as depression if it was acquired as part of a somatization disorder.
According to the results of a white paper on suicide prevention that was released by the Ministry of Health and Welfare and the Korea Suicide Prevention Center [2], the primary reason for older Korean adults to report SI was financial concerns (27.7%), followed by physical problems (27.6%). One study found that about 25% of individuals with high levels of stress reported SI, and high levels of stress led to impaired physical functioning and an increased likelihood of SI [16]. Our results were similar to these findings, as we found that respondents who rated their physical health as “very poor” and those who reported “very high” stress levels had much higher rates of SI than those with better self-rated health and lower stress levels, respectively. As the main findings of our study, self-control, anxiety/depression of EQ-5D and self-rated physical health were significantly associated with SI when adjusting for age, gender, education level, monthly income, marital status, and financial condition.
Implications of group comparisons
We considered different severity levels in each of the five EQ-5D dimensions, as well as the proportion of individuals with SI reporting “very much” stress/distress and “very poor” self-rated health was overwhelmingly higher than those in the no-SI group. Individuals with SI were consistently more likely to report problems in all five EQ-5D dimensions and have a lower-level EQ-5D index as well as lower mean values than those without SI. Based on these results, we believe that the EQ-5D would be a useful screening tool for SI among older adults. In addition, the proportion of individuals with SI reporting “very high” stress and “very poor” self-rated health was overwhelmingly higher than those in the no-SI group.
Respondents in the SI-NoDepression group were not likely to be involved in psychological counseling (3.1%). It is reasonable that people without psychological symptoms, such as depressive symptoms, do not seek psychological counseling or treatment; in addition, a previous study reported that many individuals with SI did not receive any type of intervention or treatment [44].
Strengths and limitations
Our study makes some important contributions. First, it is the first study to analyze the separate associations of the five EQ-5D dimensions with SI among older Koreans. Furthermore, we investigated the differences in SI risk based on the severity of problems (i.e., “some” or “severe” problems) in the five dimensions. Second, we used data collected using proper weighted nationwide sampling, which provided national estimations for older Koreans. Therefore, the results of this study could be generalized to older adults aged over 65 years living in Korean communities.
One limitation of this study is its cross-sectional design, which precludes causal inferences about the relationship between HRQoL and SI. Nevertheless, our findings were in line with previous studies that found negative relationships between quality of life and SI [9,28,29,40]. A second limitation is that most measures were based on self-report data, which might involve recall bias.
In conclusion, we systematically investigated physical and psychological factors as well as the five dimensions of the EQ-5D, which have been shown to play an important role in SI among Korean older adults. Among the investigated factors, self-control and anxiety/depression of the EQ-5D, self-rated physical health, and depression were significant predictors of SI, which was consistent with previous studies [45]. Therefore, effective ways to screen for and treat SI should not be limited to assessing and dealing with psychological problems, such as depression. In addition, the EQ-5D might be a useful screening tool to detect SI among older Korean adults, because it would be possible to find out how severely physical and psychological health were reported in each of the five dimensions of EQ-5D. Thus, depression screening as well as using EQ-5D, to detect SI could contribute to the reduced likelihood that a person progresses toward suicidal plans or suicidal attempts. In a future study, it would be helpful to identify the continued correlations between five dimensions of EQ-5D and SI with longitudinal analysis using cohort data of the community. Thus, it could provide valid evidence that the EQ-5D could be used as a screening tool for suicide prevention.