INTRODUCTION
According to the United Nations International Children Fund, there were about 535 million children and adolescents exposed to traumatic events worldwide in 2016 alone [1]. Traumatic exposure has been shown to be associated with shortand long-term negative mental health consequences among children and adolescents [2,3], and depression is one of the most common stress responses among youth survivors [4-6]. Considering the following reasons, itŌĆÖs necessary to focus on depression among post-traumatic children and adolescents. Firstly, there is a high prevalence rate of depression (ranging from 7.5% to 44.8%) in this population [7]. Secondly, depression has some negative impacts on both physical (e.g., obesity, pain and cerebrovascular disease) [8-10] and psychological (e.g., substance abuse/dependence, major depressive disorder and anxiety disorder) characteristics [11-13]. Thirdly, an episode of depression in adolescence is associated with a series of mental disorders in adulthood [14-16], not only influences the quality of life [17] but also increases the risk of suicide [18] and is one of the leading causes of disability globally [19].
Besides negative psychological outcomes (e.g., depression), traumatic events also can result in some positive psychological changes, such as resilience [20,21]. Traditionally, psychological resilience was described as an attribute-like personality characteristic, for the reason that some people are overwhelmed by certain hazards while others manage to overcome them [22]. But now, more and more researchers take resilience as a multidimensional, dynamic capacity [23-25] which may change over time and under different circumstance [26]. Specifically, resilience is the ability to recover from traumatic events [27]. Thus, in this study, we conceptualize resilience as the process of adaptation that follows traumatic events [28-30].
Thus, what is the relationship between those two different psychological outcomes caused by experiencing traumatic events, depression as well as resilience? Previous studies have found that resilience can reduce the risk of depression among individuals with adverse childhood experience [31,32], and low resilience to trauma events during adolescence was related to an increased risk of lifelong use of antidepressant [33]. Although variable- centered approaches had yielded much insight into the relations between depression and resilience, person-centered approaches (latent profile analysis, LPA) have the potential to extend depression and resilience by identifying how different profiles. A person-centered approach allows for distinguishing subpopulations to be identified that differ in the level (quantity) and shape (quality) of the profile indicators, which is not possible with variable-centered analyses [34]. Furthermore, the person-centered approach contributes to explore the coexisting patterns of depression and resilience among young survivors.
We conducted an LPA study in an epidemiological sample of Chinese youth earthquake survivors. The first aim was to identify the patterns of depression and resilience among children and adolescents exposed to an earthquake; It is well demonstrated that the severity of trauma exposure [35], demographic characteristics [36,37] and sleep quality [38,39] are associated with depression and/or resilience. Accordingly, the second aim was to investigate whether latent classes with different symptom features could be identified by several factors (e.g. trauma exposure, demographic and sleep quality).
METHODS
Participants and procedure
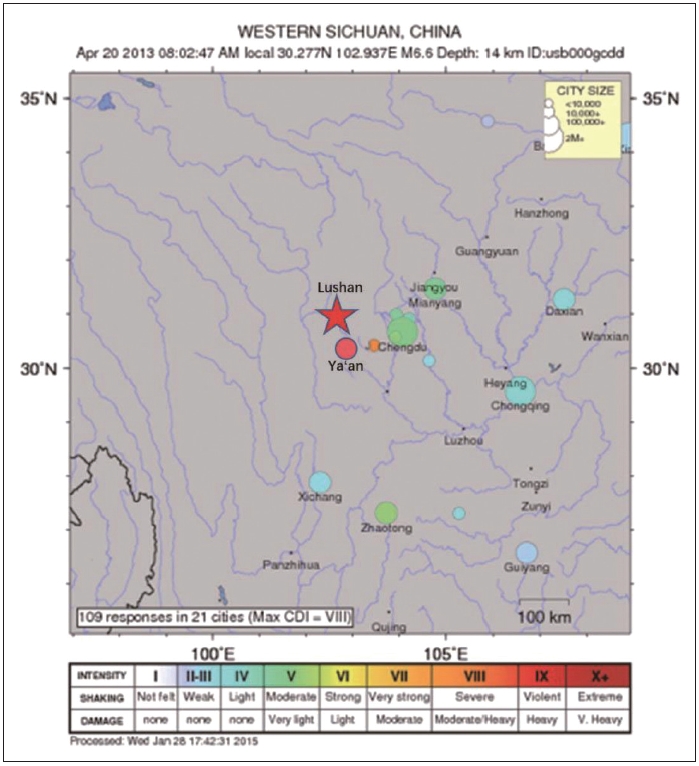
Students were recruited from 21 primary and secondary schools located in Lushan County, Sichuan Province, where was hit by the 2013 Lushan Earthquake (Figure 1). The Lushan earthquake, placed at 7.0 on the Richter scale, occurred on April 20, 2013, resulting in 21 missing, 196 deaths, and 11,470 injured [40]. The epicenter located in Lushan County, Sichuan, near the Longmengshan Fault, which has the formation with the potential to cause super strong earthquakes [41].
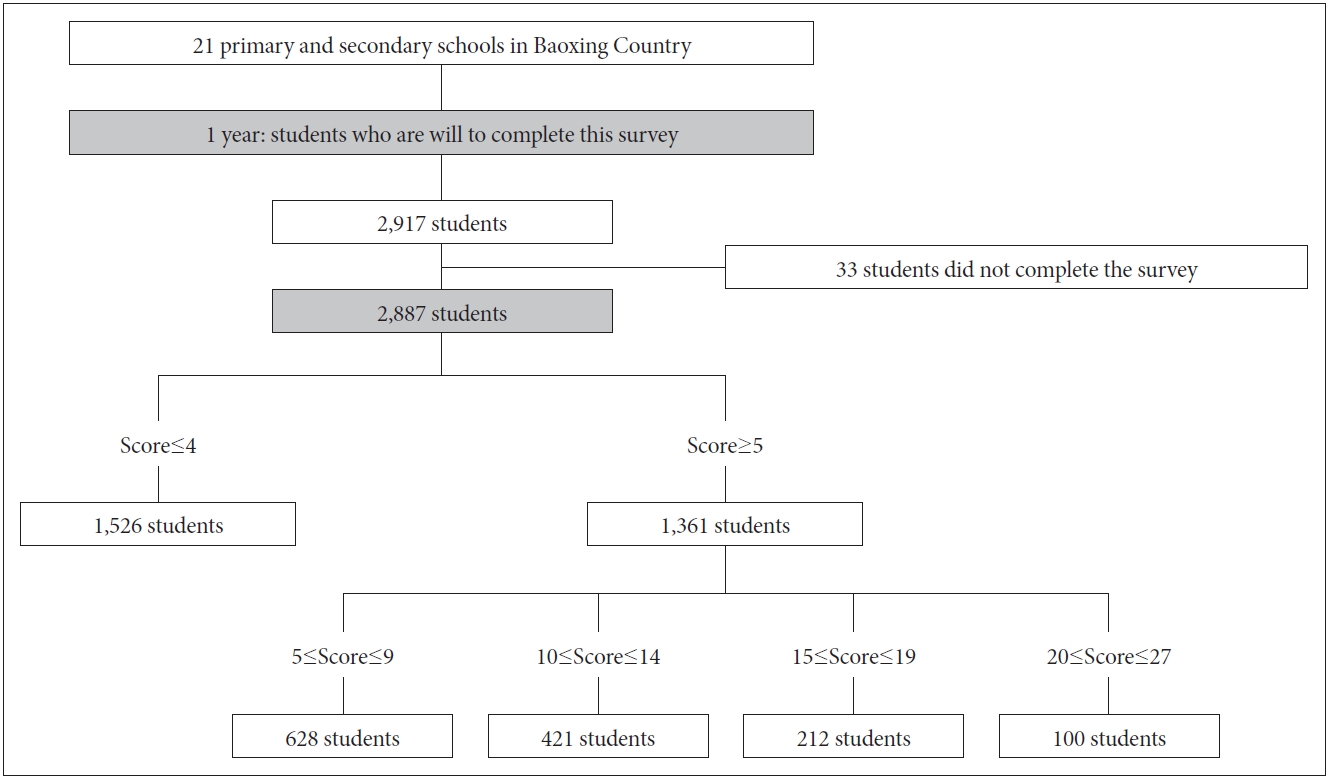
Data collection was conducted at 1 year after the Lushan earthquake. We used a paper-and-pencil questionnaire and conducted the assessment by well-trained researchers with masterŌĆÖs degree in psychology in each class to supervise participants when they filled the questionnaire. Included participants were the students who consented to participate in the survey. Excluded individuals were those who refused to participate or hadnŌĆÖt the ability to complete the investigation. In total, 2,917 children and adolescents agreed to participate. Due to that 33 students hadnŌĆÖt completed the assessments, we finally included 2,887 students in our analysis. The response rate for the assessments was 98.97% (2,887/2,917). Details about sampling strategy showed in Figure 2.
We selected Baoxing County for two reasons: 1) there were 21 primary and secondary schools in this region, satisfying the needs for a large sample; and 2) the directors of the Education Bureau and teachers of these schools paid close attention to the mental health of students. They were willing to sustain this survey. The research protocol was approved by the Ethics Committee of the University of Sichuan and the Education Bureau of Baoxing Country in China and was consistent with the latest version of Helsinki Declaration [IRB approval number: 2017 (103)] and was consistent with the latest vision of Helsinki Declaration. In the present survey, we only attained informed consent from participants and teachers. Because in China, if the local education institution (e.g., the Education Bureau of Baoxing Country) supports a survey as a mental health service to the students, parental consent is not required [42]. It was also made clear to the students that they could choose whether to participate in the survey or not [40]. More detailed information was published in a previously paper [43].
Measures
Students completed the following self-report questionnaires in their own classroom: sociodemographic characteristics, Patient Health Questionnaire-9 (PHQ-9), Child and Youth Resilience Measure (CYRM), and two self-constructed questionnaires for trauma-exposure and sleep [44]. Before the investigation was conducted, the purpose and significance of the research were introduced and a psychologist helped interpret some easily confusing items, such as ŌĆ£I solve problems without drugs or alcoholŌĆØ and ŌĆ£I try to finish what I start.ŌĆØ We provided more detailed information in Supplementary Table 1 (in the onlineonly Data Supplement).
Trauma exposure
A self-constructed questionnaire included 6 items used to assess trauma exposure severity: 1) Did your immediate family members injured in the earthquake? 2) Did your immediate family members die in the earthquake? 3) Was your house damaged in the disaster? 4) Was there anyone with you after the earthquake? 5) Did the earthquake cause severe property damage to your family? 6) Did you sleep in a tent rather than your own home last night? All answers were coded as binary variables (1 ŌĆ£YesŌĆØ or 0 ŌĆ£NoŌĆØ), and we calculated the sum score (range from 0 to 6) to reflect the severity of trauma exposure. The total score of the scale was used to assess the severity of the earthquake trauma exposure.
Sleep
A self-constructed sleep questionnaire was used to assess insomnia and 3 items were included: 1) difficulty falling asleep, 2) difficulty staying asleep, and 3) early waking. All questions and answers were coded as binary variables (yes or no). If the studentŌĆÖs answers are all ŌĆ£yes,ŌĆØ then this student is considered to have insomnia symptoms.
Patient Health Questionnaire (PHQ-9)
The self-report symptom scale of the PHQ-9 is a widely used screening tool for depression according to the Diagnostic and Statistical Manual of Mental Disorder-IV (DSM-IV) criteria [45]. The scale consists of 9-items and the items are: Over the last two weeks, how often have you been bothered by any of the following problems? 1) Little interest or pleasure in doing things. 2) Felling down, depressed, or hopeless. 3) Trouble falling or staying asleep, or sleeping too much. 4) Feeling tired of having little energy. 5) Poor appetite or overeating. 6) Feeling bad about yourselfŌĆöor that you are a failure or having let yourself or your family down. 7) Trouble concentrating on things, such as reading the newspaper or watching television. 8) Moving or speaking so slowly that other people could have noticed. Or the oppositeŌĆöbeing so fidgety or restless that you have been moving a lot more than usual. 9) Thought that you would be better off dead, or of hurting yourself in some way. The total scores range from 0 to 27, and can be divided into 4 categories: no depression (Ōēż4), minimal (5-9), mild (10-14), moderate (15-19), and severe (Ōēź20). A cut-off point of 10 has been widely accepted for the diagnostic criteria of probable major depressive disorder (pMDD) in different setting [46]. The Chinese version of PHQ-9 has good reliability and validity [47], and in the present study, the CronbachŌĆÖs alpha value was 0.899.
Child and Youth Resilience Measure (CYRM-12)
The CYRM-12 is a self-report instrument to measure youth resilience. The specific items are 1) I have people I look up to. 2) Getting an education is important to me. 3) My parent(s)/caregivers(s) know a lot about me. 4) I try to finish what I start. 5) I solve problems without harming myself or others. 6) I know where to go in my community to get help. 7) I feel I belong(ed) to at my school. 8) My family will stand by me during difficult times. 9) My friends stand by me during difficult times. 10) I am treated fairly in my community. 11) I have opportunities to develop skills that will be useful later in life. 12) I enjoy my cultural and family traditions. Items are rated on a 5-point scale from 1=does not describe me at all to 5=describes me a lot. Higher scores suggest higher levels of resilience [44]. In the present study, the CronbachŌĆÖs alpha value was 0.907, suggesting good reliability.
Data analysis
Statistical analyses were accomplished by Mplus 7.0 (Linda Muth├®n & Bengt Muth├®n, Los Angeles, CA, USA). The number of missing responses on each item of PHQ-9 were 10, 14, 13, 14, 23, 14, 23, 14, 14, 12, and 17 respectively. As for CYRM-12, they were 55, 55, 58, 70, 61, 65, 61, 54, 61, 63, 66, and 63, respectively. Missing values were estimated with maximum likelihood procedures. Considering the difference in scale range between PHQ-9 and CYRM-12, all itemsŌĆÖ scores were converted into standardized Z-scores. The 3-step LPA (R3STEP) approach was conducted via maximum likelihood estimation [48]. In the first step, the LPA model was conducted based on the PHQ-9 and CYRM-12 scale scores. In the second step, latent class membership was calculated according to the latent class posterior distribution. In the third step, trauma exposure, sex, age, ethnicity, and insomnia were treated as independent variables to predict latent class membership. Odd ratios (ORs) were calculated according to the beta values and standard errors.
The evaluation indexes of LPA model fitting degree are Akaike Information Criteria (AIC) values, Bayesian Information Criteria (BIC) values, adjusted BIC (aBIC), Entropy, Lo-Mendell-Rubin likelihood ratio test (LMR LRT) and Bootstrap-based Likelihood Ratio Test (BLRT) [49]. The smaller values of AIC, BIC and aBIC are, the better fit of the model is. Entropy is mainly used to evaluate the accuracy of classification, ranging from 0-1. The closer it is to 1, the higher accuracy of the classification is. The LMR LRT and BLRT indicators are used to compare the fit differences between the n and n-1 categories. For instance, an LPA model with 4 categories, the p-values for LMR LRT and BLRT are used to compare the differences in fit between the 4 categories and the 3 category models. If the p values of all LMR LRT and BLRT are significant, it means that the four categories of models fit better than the three categories; if the p values of LMR LRT and BLRT are not significant, it means that the three categories of models are better than the four categories. If the p values of BLRT and LMR LRT are inconsistent, the actual number of potential categories and the number of samples included in the category should be combined to determine the final number of potential categories.
RESULTS
A total of 2,887 children and adolescents completed the assessment (1,541 female; 2,375 Han-people and 247 meet the criteria of insomnia) (Table 1). The mean score of age was 12.83┬▒2.58 and total earthquake exposure was 2.62┬▒0.77. Mean scores for the PHQ-9 and CYRM-12 were 6.05┬▒6.25 and 36.9┬▒10.86, respectively. By counting the scores of PHQ-9 that higher than the value of 4, the probable depression diagnosis is 46.73% (minimal depression 21.65%, mild depression 14.34%, moderate depression 7.27% and severe depression 3.46%, respectively).
Fit indicators of the different LPA models are shown in Table 2. The BLRT p-values and LMR p-values were significant for each class category comparison (╬▒=0.50). AIC, BIC, and aBIC tend to keep decreasing as increasing the number of latent classes. Thus, these fit indicators may not help much in choosing suitable models. The 2-class to 5-class model all had acceptable entropy value (>0.90). While, compared with the 3-class model, the 4-class model and the 2-class model showed inappropriate class probability. For the 2-class model, the class probability too simple to reflect symptoms well. For the 4-class model, it has a low proportion of class probability, which is 4.82%. Overall, we choose the 3-class model as the most suitable model, as it was more meaningful and parsimonious.
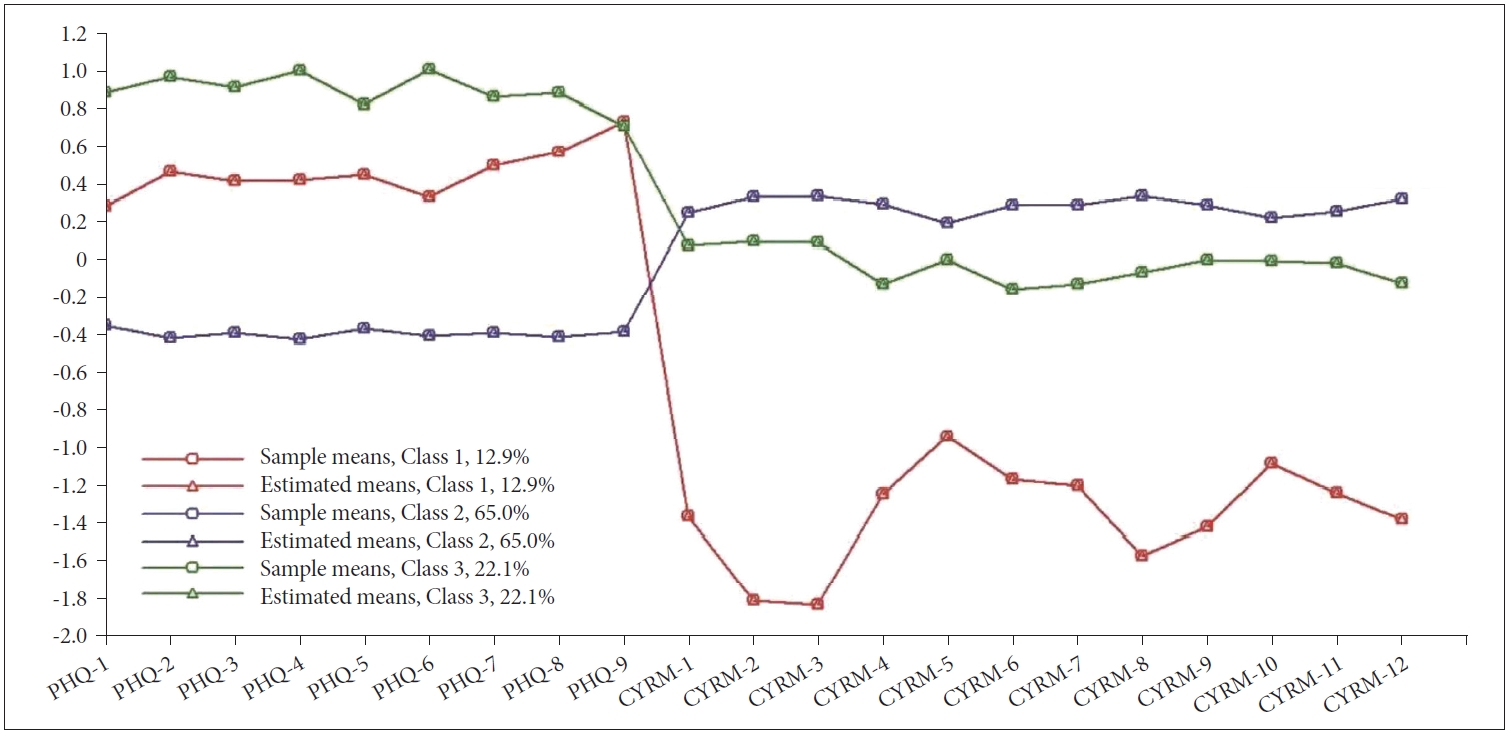
The 3-class model was characterized by severe depression/low resilience (12.90%), severe depression/high resilience (22.11%), mild depression/high resilience (65.00%). The 3-class modelŌĆÖs profile plot of depression and resilience was shown in Figure 3. In the severe depression/low resilience and mild depression/high resilience subgroups, depression symptoms coexisted with the opposite level of resilience. However, in the severe depression/high resilience group, individuals presented relatively high levels of depression and relatively high levels of resilience.
The final step of the 3-step LPA results was presented in Table 3. Compared with class-2 (mild depression/high resilience), individuals in class-1 (severe depression/low resilience) and class-3 (severe depression/high resilience) were more likely to be older and suffered insomnia symptom, while individuals in class-2 (mild depression/high resilience) were more likely to be male and not Han-people. Trauma exposure was a significant predictor of the class-3 (severe depression/high resilience) compared with class-1 (severe depression/low resilience) and class-2 (mild depression/high resilience).
DISCUSSION
Our study identified 3 latent classes of depression and resilience (severe depression/low resilience, mild depression/high resilience, and severe depression/high resilience) among Chinese youth earthquake survivors, in line with SpahniŌĆÖs founding [50]. Different latent classes can be identified by different sociodemographic features (e.g., sex, age, and ethnicity), trauma exposure severity and insomnia symptoms.
Three latent class of depression and resilience
In presented study, a great proportion of individuals were in the mild depression/high resilience group, which was in accordance with findings of Wenchuan earthquakeŌĆÖs youth sample [51]. We both indicated that most individuals obtained positive psychological changes following the earthquake. Based on a previous longitudinal research, resilience does indeed buffer the negative influences of stressful life events over time [52]. As the positive psychology emphasizes, we should focus on the positive aspects (e.g., resilience and post-traumatic growth) of traumatic experience, not only on the negative side [53,54]. Our results highlight the potential beneficial influences from the traumatic events.
An interesting phenomenon of this study also sheds light on the controversial relationship between depression and resilience. Negative relationship between those two constructs is shown in the mild depression/high resilience and severe depression/low resilience subgroups. While, as for the severe depression/high resilience subgroup, depression and resilience levels were reflective of each other. ItŌĆÖs presented a positive association between depression and resilience. These findings indicate complicated reactions among youth survivors, and individualŌĆÖs heterogeneity should be considered.
Factors associated with the latent class groups
The higher level of trauma exposure was related to the higher probability of being classified into the latent class with a high level of depression (severe depression/high resilience and severe depression/low resilience). A link had been found between trauma exposure and depression, such that individuals who witness the disaster, death/injuries of family members and damage to oneŌĆÖs home are being more prone to depression [42,55]. Meanwhile, other studies also had found that a higher level of trauma exposure was related to a higher level of resilience. When youth survivors have been subject to a traumatic event (such as an earthquake), the experience has led to a positive adjustment [56].
The role of demographic characteristics was also explored. Compared to their counterparts, male and younger survivors were more likely to enter mild depression/high resilience. Female and maleŌĆÖs post-traumatic reactions are markedly different. For example, greater levels of self-esteem and mastery, more common among the male than the female, are positively associated with problem-focused coping, which could reduce the negative impacts of stress [57]. In contrast, females use more emotion- focused coping strategies [58], which may make them at risk of trapping in depression. In addition, females more frequently express fear and shame than do male [59,60]. Fear and shame can cause survivors to have a negative outlook on their surroundings, namely, low resilience. Low resilience can make negative reappraisals of trauma-related cues and considered the trauma as more threatening [61]. For youth survivors, they may attain more support from family and society, which are resources related to better mental health. As a type of stress buffer, instrumental aid, active assistance or emotional support from parents or similar others could help to alleviate the impacts of traumatic events [62]. The previous study also emphasizes the role of supportive relationships with caregivers at preventing children from post-traumatic psychopathology, which could help children dampening the threat processing [63].
The roles of sleep characteristics were also clarified. The results showed that insomnia individuals were likely to enter the severe depression/low resilience subgroup. SeeligŌĆÖs study found that poor sleep is an important factor and related to the construct of resilience [64]. Sleep and resilience can share an underlying neural mechanism and therefore affect one another. Sleep impacted levels of resilience, meaning that greater sleep disturbance could reduce resilience and may potentially predispose individuals to psychopathology such as depression [38].
Clinical implication
The current study also provided potential clinical implications. First, based on the person-centered method LPA, our study promotes the understanding of different psychological reactions (depression vs. resilience) as well as individual heterogeneity among youth survivors. Most individuals were in the mild depression/high resilience group, suggesting that resilience may buffer the influence of trauma experience on depression. Thus, in future, we can provide many types of online psychological services for youth survivors to promote their psychological resilience. Second, in our study, we found some important moderating factors (e.g. sleep disturbance) that can influence the relationship between resilience and depression, and indicated more attention should be paid to older insomnia female individuals. As posited by previous research, the presentation of mental disorders are influenced by culture and social milieu [65], and Chinese population is more prone to report more somatic symptoms instead of depression symptoms [66]. Considering sleep disturbance is a relative modifiable factor and more accept mental disorder among Chinese general population. Thus, we can intervene on sleep symptoms to mitigate the outcomes of depressive symptoms [67,68]. Third, it should be aware that our study was conducted at 1-year after the earthquake, which assessed the long-term psychological effect of earthquake exposure. In consistent with SharmaŌĆÖs study on the Nepal Earthquake [69], we both found a considerable prevalence of depression among youth survivors even after one year of the event. Thus, there is a need for early intervention for youth survivors and we should also pay more attention to the longlasting effects of traumatic event.
Limitations
Several limitations of our study should be mentioned. First, the findings of our study are based on the self-report scales (e.g., PHQ-9) reported rather than the clinic structure interviewed. And the design of our study was just a cross-sectional study. High quality prospective studies are needed. Second, our research targets on the sample of Chinese youth-earthquake survivors after 1-year exposure, which limits the generalization of the findings. Further studies should examine the profile of depression and resilience in various types of traumatic events among different time points to test the robustness of the model. Third, we only focused on depression in this paper. Other important mental health outcomes (e.g., PTSD, generalized anxiety disorder) are relevant to the trauma events and should not be ignored in further study. Forth, whether resilience is a personality trait or dynamic process is controversial in different studies. In future research, we can evaluate positive psychological through the post-traumatic growth (PTG).