INTRODUCTION
Grandparents are an important source of safety and support to grandchildren. More and more parents opt for this type of support: grandparents are perceived as a trustable and reliable source, ensuring a family circle of caring [1-4].
In developed countries, morbidity and mortality are declining among older adults. As a result, grandparents have more healthy years with their grandchildren than formerly [5]. Also, on average, a child has three or four living grandparents through childhood [6]. These factors help both generations to build stronger relationships while helping with family dynamics, including childcare.
In the United States, children with 1 or 2 years of age spend more time at grandparent’s care than at day care centers. In this context, 25% of preschool children are regularly cared by their grandparents [7]. In Europe, a study based on the Survey of Health, Ageing and Retirement (SHARE) showed that almost 50% of the grandparents look after their grandchildren of which 15% provided intensive grandchild care (almost daily or at least 15 hours per week) [8].
There are several factors related with the need of grandchildren care, such as: poverty or economic problems, culture, mother’s employment, father-only family, divorce or migration, among others. Frequently, both grandparents and parents, contribute with their time, labor, money and childcare in these situations [1,7].
Regarding the association between grandparental childcare and health, the SHARE study also concluded that there is a positive association between grandchild care (intensive and non-intensive) and better physical health among grandmothers [8]. Based on the same survey, other study showed better health with grandchild care, even if previous health or life events were taken into account [8].
Although the apparent benefit of grandchildren care, some studies suggest the opposite [2,4,9,10]. Women that become grandmothers earlier, married or with many children, may have higher mortality. On the contrary, taking this role after 50 years of age lowers mortality [9]. A recent systematic review 4 pointed out some negative consequences in grandparents’ life who have custodial care: loss and grief, loneliness, depression, social isolation, financial difficulties, disruption of social activities, alternation of family relationships and physical well-being decline. In Portugal, the rate of houses with co-habiting grandparents is high (6.5-11%) and in most of those, also live children [11]. Culture can be an explanation for this fact, since Portuguese society has a tradition of familism and family members rely on each other throughout life. However, the three generational houses have worst finances, even if one grandparent has a job [11,12].
Nowadays, fertility is being postponed, career goals are different, and grandparents achieve this role later in life [5,12]. With aging there is a prevalent increase of some diseases such as dementia: 5% to 10% of adults with more than 65 years of age [13]. Several studies tried to understand the influence of caring for grandchildren in the mental health of grandparents [8,14-17]. A longitudinal study [16] described a positive effect of grandchildren care regarding older persons’ loneliness and depression. Even though, depressive symptoms would worsen if there was a time when they took care of their grandchildren and then stopped.
As a bridge to social engagement, contact and activities, grandchildren care can be protective and associated with lower risk of dementia. Several studies [18,19] show this protective effect of social activities on cognitive function and dementia. Even in people with severe levels of pathology on autopsy, cognitive function was higher if they had a larger social network size [20]. An active and stimulating life style can also be protector and grandparenting can be a form of daily activity and exercise [13,21,22]. However, not all studies point on the same direction, with some [22] suggesting that a negative impact on cognitive performance can be associated with grandparenting.
Nowadays there is an increasing concern about cognition and its decline, especially in older persons. Consequently, searching for factors that may influence this function is pertinent. One of the social activities frequently associated with this age group is taking care of grandchildren. Assembling these two facts, it seems important to review the actual scientific knowledge about grandparenting and grandparent’s cognition.
This systematic review aims to evaluate the relationship between grandparenting and the cognitive impairment of older persons. The authors aim at answering the following questions:
1) When compared to other older persons, do grandparents who care for grandchildren have more, less, or the same cognitive impairment?
2) For question 1, what factors can explain the differences found?
3) Regarding mental health, specifically cognition, should physicians have specific advises for older persons on grandchildren care?
METHODS
Protocol and registration
We elaborated a protocol that complies with the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-p) 2015 checklist [23]. Our systematic review protocol was submitted to the International Prospective Register of Systematic Reviews (PROSPERO), registration number: CRD42018105849.
Ethics approval was not required for this systematic review. The present review complies with the PRISMA checklist [24].
Eligibility criteria
Study designs
All articles with original evidence using qualitative and/or quantitative research methods, systematic and narrative review articles, metanalysis, short communications and editorials were considered and evaluated for inclusion in this review.
Participants
We included studies with human subjects. No age limits have been applied for study subjects, since the age of becoming a grandparent varies greatly. Adults without grandchildren were included if data from grandparents at the same study is provided.
Interventions
Grandparenting is the main event of this review. No restriction was made concerning characteristics of grandchildren care.
Outcomes
Primary outcome measure considered was cognitive impairment in grandparents. Herein, the cognitive domain affected can vary and be measured by different scales. No restrictions on definition, how cognition was measured, or followup length were applied. Studies without cognitive evaluations were excluded.
Other reported outcomes, after selection for cognitive impairment, were taken into account: employment, education, physical health and depression in grandparents.
Information sources
We searched for studies in the following electronic databases: PubMed (which includes MEDLINE), ISI Web of Knowledge, Scopus, and EBSCOhost platform to access PsycINFO, CINAHL Plus with Full Text, Humanities Abstracts (H.W. Wilson), and PsycARTICLES. Reference lists of included studies or relevant reviews were also scanned to ensure a good literature support.
Search strategy
Our search strategy was defined by two of the authors (A.R., L.S.) and implemented by august 2018. Several keywords combinations were tested to ensure that the strategy would retrieve a high proportion of eligible studies. When the platform allowed, we selected human subjects and the previous referred types of study. We present the search strategy in the Protocol referred above.
Study selection
Retrieved citations from the search were uploaded and End-Note X8® was used as reference management software. There was a first screening stage and, based on the title and abstract, studies moved to the second screening stage if they met all eligibility criteria or if there was uncertainty about their eligibility. In the second screening stage, the full text was assessed. Reasons for excluding citations in the second screening stage were recorded.
Data collection process
Eligibility assessment for selecting studies was performed independently by 2 reviewers (A.R., L.S.) to reduce the possibility of rejecting relevant reports, at both screening stages. In case of disagreement between the two reviewers, a third member of the team was consulted (L.F.). Data was extracted and confirmed by the 2 reviewers. Statistical analyses were not performed.
Data items
We present a systematic review with information presented in the text and in a table to summarize and explain the characteristics and findings of the included studies. The results will be presented first by characteristics of the studies, and then in order of scientific findings, from main to additional outcomes.
Information was extracted from each included study on: 1) characteristics of the study (authors, year, country, study design, setting, aim; research questions and time of follow-up) 2) characteristics of participants (age, gender, grandparents, not grandparents, sample size), and inclusion/exclusion criteria; 3) cognitive impairment (type of measurement, level of impairment) and other outcomes of interest measured; 4) grandparenting (custodial/occasional, reasons for grandchild care, time of caring, family context). Once the age of becoming a grandparent is highly variable, an assumption of searching only for aged persons was not made.
Risk of bias in individual studies
The quality of included articles was evaluated by two reviewers (A.R., L.S.) independently. Disagreements were resolved by discussion. It was used the Downs and Black [25] checklist for randomized and non-randomized studies. Our search did not retrieve any qualitative studies.
RESULTS
Study selection
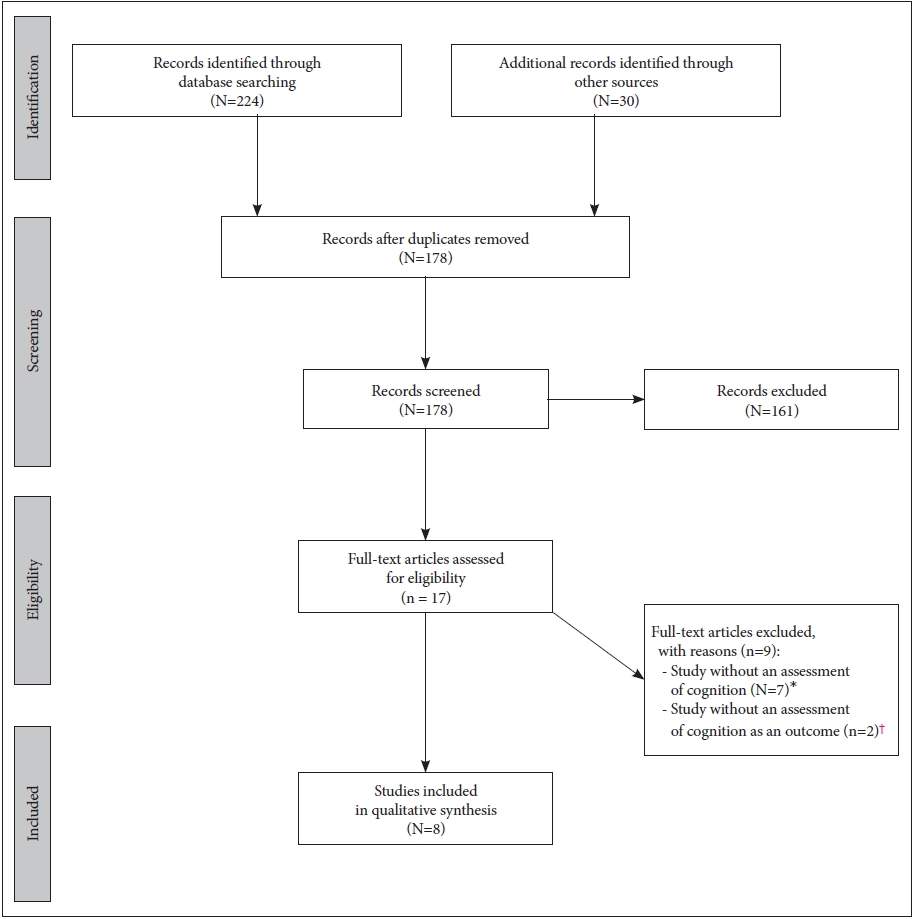
Our search identified a total of 224 records. 30 additional records were found at data platforms, when similar studies were suggested by the platforms, and through snowballing process. After exclusion of duplicates, 178 records were considered for further analysis. Of those, seventeen records entered the second phase. The title and/or abstract of excluded records on the first phase showed these didn’t fulfil the inclusion/exclusion criteria to the present study.
After applying eligibility criteria to select the studies, nine were excluded on the second phase. Seven studies [16,26-31] were excluded for not having an assessment of cognition. Two studies [8,32] were excluded once cognition was not an outcome.
Study characteristics
As previously stated, five of the eight selected studies were original articles. All the original studies were published in English and had an observational and retrospective design. Key features are summarized in Table 1.
The overall number of participants was 38,002, from different countries but all from community dwelling. The most frequent inclusion criteria were adults, women, and have grandchildren. As exposure, all the studies evaluated taking care of grandchildren and their primary outcome was cognition. Secondary or additional outcomes were not present in all studies. The characteristics of each original study regarding population, sample, type of grandparental child care, tests used to evaluate cognition and other relevant variables are presented next.
Arpino and Bordone [33] conducted a repeated cross-sectional study, retrieving their sample form the successive waves of 2004/2005 and 2006/2007 from SHARE, a multidisciplinary longitudinal survey, representative of noninstitutionalized population aged 50 and over. Data retrieved was from the following countries: Austria, Belgium, Czech Republic, Denmark, France, Germany, Greece, Ireland, Israel, Italy, Netherlands, Poland, Spain, Sweden and Switzerland. Participants were women and men (5,610 and 4,760, respectively), with one or more child and with 50 to 80 years old. Those who were permanently sick or disabled, with history of stroke/Parkinson’s disease or cancer, grandparents with co-resident grandchildren, and outliers for the outcome variable or missing values were excluded. Grandparental child care evaluated was supplementary care (i.e. complementary to parental care) in the previous 12 months; primary or co-residing child care categories were excluded. High (>2.5 hours/day), moderate (0.8-2.5 hours/day) or low (0.25-0.8 hours/day) care was compared to very low (0-0.25 hours/day) or none care (including not having grandchildren). Cognition was evaluated through the following tests: verbal fluency, numeracy, immediate recall and delayed recall. Several covariables were included: country, age, education, partner, activity status, social activities, health (limitations on activities of daily living, self-reported health, depression), physical inactivity, smoking and alcohol consumption.
Two studies from Burn et al. [34], and Burn and Szoeke [35] with a cross-sectional design, retrieved their sample from the Women’s Healthy Ageing Project (WHAP). This is an Australian project consisting on a follow-up to the Melbourne Women’s Midlife Health Project with postmenopausal women, aged 45 to 55 in 1991, Australian-born, who had menstruated 3 months prior to recruitment, and had not taken oestrogen-containing hormone therapy. Burn et al. [34] selected 186 women who were aged 57 to 68, from the WHAP wave of 2002/2004. The authors included participants who completed all relevant neuropsychological measures and were not missing key demographic data. Regarding grandchild care, the following comparisons were made: having versus not having grandchildren; not having versus not minding grandchildren; and minding versus not minding grandchildren. Time spent minding grandchildren was also evaluated and compared: never, once every few months, once per month, once every couple of weeks, few hours per week; 1, >1, ≥3 or ≥5 days/week. Cognition was evaluated using California Verbal Learning Test (CVLT), with immediate and delayed recall, for verbal episodic memory; Symbol-Digit Modalities Test (SDMT), for working memory and processing speed; and Tower of London (TOL), for executive function. The predictors included were: age, education, employment status and time spent minding grandchildren. The secondary outcome measured was feeling demand in the previous 12 months.
Burn and Szoeke [35] selected 224 women who were aged 64 to 77, from the wave of 2012/2014 of WHAP. The authors excluded participants with neurological impairment, incomplete data on grandparenting or cognitive function, and medical reasons. Regarding grandchild care, the following differences were evaluated: not having grandchildren, having grandchildren and minding grandchildren. Time spent minding grandchildren was investigated as 1 day/week or >1 days/week. Cognition was evaluated using CVLT (with delayed recall and recognition) and Controlled oral word association test (COWAT) for verbal episodic memory; digit span task (DST) and Verbal fluency test (animals and names), for executive function; Rey-Osterreith complex figure test (RCFT), with copy and delayed recall, for visuospatial function. The control variables included were: age, education and time with grandchildren. The secondary outcome measured was feeling demand in the previous 12 months.
Jun [36] conducted a longitudinal study and retrieved their sample form the waves of 2008 (Time 2) and 2010 (Time 3) from the Korean Longitudinal Study of Aging (KLoSA), meaning a follow-up time of 2 years. KLoSA is a nationally representative sample of Koreans with ≥45 years old. In this study, participants were 2,341 women, with 50 to 74 years old. The authors included: women, aged 45 to 74 at Time 2, participation in all 3 waves of KLoSA, living grandchildren at Time 2, grandchildren aged ≤10. The sample was limited to grandmothers who provided more intensive and frequent child care (≥10 hours/week). Cognition was evaluated using the Korean version of the Mini-Mental State Exam (K-MMSE). Several control variables were included: age, marital status, household income, caregiver status, employment status, frequency of participation in social groups at Time 2, general health status and depression (10-item Center for Epidemiologic Studies-Depression scale). Education was considered a moderator in this study.
Reinkowski [37] also designed a longitudinal study, with a follow-up time of 8 years. Their sample originated from the waves of 2004/2005, 2006/2007, and 2011/2012 from SHARE. Data retrieved was from the following countries: Austria, Belgium, Czechia, Denmark, Estonia, France, Germany, Greece, Hungary, Ireland, Israel, Italy, Netherlands, Poland, Portugal, Slovenia, Spain, Sweden, Switzerland. Participants were 29,461 women, with 45 to 90 years old. Besides these two characteristics, were included those with ≥1 grandchild aged ≤16 and who have complete survey records. Grandparental child care evaluated was occasional care (i.e. 200 to 500 hours per year): no care, 0; almost daily, 38.7; almost every week, 11.3; almost monthly, 5.8; less than monthly, 2.4 mean hours/week. Cognition was evaluated through immediate recall and delayed recall tests. Other outcomes measured were: physical health (index) and mental health (euro-D depression index). Control variables used were: age, education, marital status, employment status, wealth, geographic distance and social engagement. Explanatory variables were: number of children and of grandchildren.
Risk of bias between studies
We assessed the risk of bias in our five original studies included using Downs and Black [25] checklist and both authors agreed that all those studies had enough quality to be presented. Studies were punctuated with a score considered fair/medium, of 14 to 17 point on a possible total of 27. This result consensual between the two reviewers on three-17 points to Arpino and Bordone [33], 17 to Burn and Szoeke [35], 16 to Burn et al. [34]- and differed on two but maintaining the same level-17 and 14 to Jun [36], 17 and 15 to Reinkowski [37].
Results of individual studies
Grandparenting and Cognitive Impairment
In the study from Arpino and Bordone [33], 14% of grandmothers and 7.52% of grandfathers provided high intensity grandparental care (>2 hours/day). 59.68% of women and 73% of men did not have a grandchild or provided none/little care in previous 12 months. Regarding supplementary grandparental child care, the authors described that grandparents who were more intensively engaged in child care, showed the lowest average cognitive scores in all the four tests performed. However, when considering all the control variables using an instrumental variable with Two-Stage Least Squares (2SLS) approach, for both grandmothers and grandfathers, providing child care had a positive effect on the verbal fluency test, tending to increase with the amount of child care provided (low, p<0.05; medium, p<0.01; and high care, p<0.001). Comparing genders on the same level of engagement, the results were similar. For grandfathers, the “optimal” level of engagement was medium, whereas a high level of engagement seemed to be the best for grandmothers.
Burn et al. [34] presented a sample of 131 grandmothers, with a mean age of 61.93 years old (SD 2.52), and a mean of 4 (SD 3.13) grandchildren. From these, 20 didn’t mind their grandchildren. There were 55 participants who were not grandmothers and who were 1.07 years younger (p<0.01) and had 0.96 more education (p<0.01) than grandmothers. Regarding the comparison of grandmothers/nongrandmothers, no significant differences in cognitive tests were seen. In what concerns the time spent minding grandchildren, the highest cognitive scores for most tests were seen in participants who minded grandchildren for 1 day/week. Using standard multiple regression, the study concluded that minding grandchildren for 1 day/week positively predicted CVLT immediate recall (p< 0.05). Minding grandchildren for ≥5 days/week negatively predicted SDMT performance (p<0.05). The authors suggest that it can exist a limit to the benefits of caregiving.
Burn and Szoeke [35], had a sample with a mean age of 65.55 years old (SD=2.61). Also, 72.2% of grandmothers minded their grandchildren and had a mean of 3.17 (SD 2.04) grandchildren, were 0.94 years younger (p<0.05) and more likely to have ≥12 years of education (p<0.01) than those who didn’t mind grandchildren. Using multivariate analysis methods, authors found that participants who were minding their grandchildren exhibited higher executive function scores than those who were not minding grandchildren or non-grandparents (p<0.05). Minding grandchildren less time (1 day/week) predicted higher executive function scores than minding for >1 day/week (p<0.05).
Jun [36] had a sample with 170 child care providers, and 2,171 nonchild care providers. Using multiple regression analyses and regarding cognition, providing child care ≥10 hours/week to grandchildren younger than 10 years old was positively associated with cognitive functioning (p<0.05). However, child care at that time was not associated with cognitive function two years after. This is against lagged effects on cognition. When including education as a moderator, on Jun [36], child care was both instantaneously (p<0.01) and longitudinally (p<0.01) beneficial to cognition for grandmothers with higher education versus lower education. The authors concluded that grandchild care can have different effects on cognitive function, depending on the educational level of grandmothers.
In the sample analysed by Reinkowski [37], 35.6% of grandmothers did not provide care for grandchildren, while 64.4% did. It was found a positive correlation between grandchild care and cognitive functioning: in Ordinary Least Squares regressions, when controlling for age, education, country and year dummies, and socio-demographic characteristics, grandchild care had a positive and statistically significant effect on cognitive functioning (p<0.01). The same stands for physical health (p<0.01) but not for mental health. However, regarding the 2 SLS estimation, the causality of grandchild care wasn’t significant for neither of them. This is a working paper that shows that occasional grandchild care does not have a significant causal effect on grandmothers’ cognition when using an instrumental variable approach. Also, there were no significant differences in the region-specific care effects for cognitive function in Europe.
The revision included from Burn and Szoeke [22] consisted on a classical narrative review. The author’s focus is the role of grandparenting in cognitive aging. The authors argument that grandparenting can be considered a social role that stimulates cognition, maintaining it. However, based on other studies, they suggest that minding grandchildren to the point of experiencing demand may be harmful to cognitive function.
The work from Campbell et al. [17] is an editorial paper approaching the current research on grandparents. Articles included were obtained from previous decade review and a PubMed search on the term “grandparent” and “caregiving”, limited to the previous 5 years. Key findings from 25 studies were summarized. Regarding cognition, it included two of the studies on the present study [33,34] and two conference papers, both finding a positive relationship between grandparenting and cognition overall, and negative influence on cognition associated with intense grandparenting.
Other factors evaluated
On Arpino and Bordone [33], the more intensively engaged grandparents were, older, less educated, in worse health, more likely to be retired, and less involved in social and physical activities than the respondents not looking after grandchildren. The authors suggested that the health disadvantages for grandparents might arise from grandparents’ prior characteristics, and not because of providing care to grandchildren.
Burn et al. [34] analysed predictor variables and verified that employment status was a negative predictor of both CVLT immediate and delayed recall (p<0.05), and that education was a positive predictor of SDMT performance (p<0.05). Considering the secondary outcome, 67.6% of the sample did not report feeling demand in the previous 12 months. The amount of time minding grandchildren was positively associated with feeling demand from children (p<0.01).
Regarding the secondary outcome from Burn and Szoeke [35], 44.6% participants reported feeling demand in the previous 12 months. Those who were minding >1 day/week were more likely to report feeling demands but this was not associated with cognitive differences.
Regarding other variables, on Jun [36], grandchild care was positively associated with education (p<0.05) and household income (p<0.001), but negatively associated with age (p<0.01), employment status (p<0.001), and depression (p<0.01).
The revision included from Burn and Szoeke [22] points out that an active lifestyle and social engagement can be associated with higher cognitive function, less cognitive decline and reduce risk of developing dementia. At last, they debate the possible negative influence of carer burden as a physical and mental hard demand, opposite to the sense of purpose and daily activity associated with caring.
On the work from Campbell et al. [17], grandparental care was associated with happiness, purpose, lower stress, greater wellbeing and greater life satisfaction. Living with grandchildren was associated with protection against depression and loneliness. However, grandparents at full-time had higher probability of depressive symptoms and grandparental custodial care was associated with poorer physical and emotional health. The author also demonstrated an increase in the number of studies in the literature about grandparents.
Woods [38] calls attention for the fact that some grandparents look forward for grandparenting and identify themselves with this role. Nevertheless, for others it is a demanding and not expected role, especially grandmothers with custodial care.
DISCUSSION
Summary of evidence
Four studies, Arpino and Bordone [33], Burn et al. [34], Burn and Szoeke [35] and Jun [36], found a positive relationship between grandparenting and different cognition assessment tests: verbal fluency (related with a crystallized component of cognition), CVLT (for verbal episodic memory), DST/verbal fluency test (for executive function), K-MMSE (for global cognitive functioning). However, Burn et al. [34] also suggested a limit to the benefits of caregiving, with more intense grandparental care being associated with worst working memory and processing speed (SDMT). Moreover Reinkowski [37] suggested that grandchild care did not have a significant causal effect on grandparents’ cognition. This is a result approximated to the results of longitudinal study developed by Jun [36] except that here it was stated that grandchild care can have different effects on global cognitive functioning (K-MMSE), when analysing by grandmothers’ educational level.
Considering other outcomes, Burn et al. [34] found a positive association between feeling demand and the time spent minding grandchildren and Burn and Szoeke [35] tested for its association with cognition but it was not significant.
Employment status was a negative predictor for verbal episodic memory (CVLT) on Burn et al. [34] and education was a positive predictor for working memory and processing speed (SDMT). Parallel to this, on Jun [36], grandchild care was positively associated with education (p<0.05) and household income (p<0.001), but negatively associated with age (p<0.01), employment status (p<0.001), and depression (p<0.01). Other outcome evaluated by Reinkowski [37] was mental health (using euro-D depression index) and physical health. Although physical health has been positively correlated with grandchild care and cognitive function, after a more precise statistical analysis, the causal effect was not verified for neither of the two variables.
Regarding individual advantages of studies, we consider that those who restricted their sample to a specific type of grandparenting are more accurate once this aspect can have different implications [39]. Arpino and Bordone [33] and Reinkowski [37] evaluated supplementary and occasional care, respectively. The only study that evaluated gender differences was Arpino and Bordone [33]; the other studies evaluated only women and it can be important to consider that cognitive features are modulated in a different way [40]. Also related with sociodemographic characteristics, grandchildren’s age can be important considering different demands on care across different ages. Jun [36] and Reinkowski [37] limited grandchildren’s age to 10 and 16 years old, respectively. Finally, these two studies were the only ones considering social engagement.
Considering health and diseases associated with cognitive impairment, Arpino and Bordone [33] and Burn and Szoeke [35] excluded participants with medical conditions that could affect the outcome. Jun [36], controlled for previous level of grandmothers’ cognition.
Neither of the included studies evaluated what activities grandparents do when they mind grandchildren or whether the care was voluntary or not. All the samples were retrieved from populational longitudinal surveys. Persons who agree to participate on these surveys can be the ones healthier or with more free time than the general population, what can have implications on the outcomes. Also related with the samples sizes, Burn et al. [34] and Burn and Szoeke [35] had significantly smaller samples than the other studies (186 and 224 participants, respectively). In longitudinal studies, Jun [36] had less time of follow-up (two years) than Reinkowski (eight years) [37].
Statistical analysis is also important. Cross-sectional studies can limit the ability to find an accurate relationship between grandparenting and cognition [33-35]. Arpino and Bordone [33] and Reinkowski [37] had an Instrumental Variable Approach as statistic methodology to correct for confounding, what can be an advantage [41].
Lastly, considering our principal question, in all studies there seems to be a trend towards a positive effect on grandparents’ cognition associated with taking care of their grandchildren.
In the studies included, various factors can explain the differences found between groups such as the demand of grandparenting role, employment status of grandparents, educational level of grandmothers, depression and physical health.
Regarding the narrative review and the two editorials, Burn and Szoeke [35] and Woods [38] they were mainly used for snowballing process. The narrative review [22] differs from ours, once our methodology consisted in a more systematic and precise approach, and also more recent. Their findings were based on two of our included articles, and two conference papers that were not included in our review. The latter did not present significantly different conclusions, just adding the importance of differences between genders.
When asking if physicians should have specific advises for older persons on grandchildren care and cognitive impairment, despite the promising results, one should have caution on counselling grandparents regarding the positive effects of grandchild care on cognition since evidence is still weak and it seems that up to a certain level highly frequent grandparenting might as well have some deleterious effects. Also, most of the studies are not restricted to older persons, what can influence the evidence on this subject.
Limitations
There were substantial differences across studies, not only concerning the design of the study or inclusion/exclusion criteria, but also regarding specificities of grandparenting, measures of the outcomes and statistical analysis. There was insufficient similarity for the development of a quantitative analysis of findings across studies. Instead, we described the studies, indicating which differences were statistically significant, without comparing direct measured results between studies. We were not able to present metanalytic measures due to the great heterogeneity regarding study designs and outcome measures. Results must be considered with caution once there are diverse contextual factors that were not taken into account, specially differences between countries, cultures, families.
Implications for futures studies
In future research, more precise inclusion criteria should be established. Definition of the type of grandparental care is important according to differences between levels of care: custodial (i.e. being the primary caregiver), non-caregiver or caregiver (occasional, intermediate or extensive caregivers, according to hours of grandchild care in an average week and overnight care) [39]. Living in the same household can also be considered as a differentiator. The age of grandparents and previous diseases should be considered once mild cognitive impairment and dementia can develop in older persons due to organic and degenerative processes. Also, grandfathers should systematically be included once it was suggested that there can be differences between genders [33]. Number of grandchildren and their age may also be considered as a predictor variable or as a factor for sample stratification, considering the different demands through a child’s development. As a potential social role, it would be interesting to assess what kind of activities do grandparents practice with their grandchildren: play or practice physical activity can be different from feeding or household shores. It would also be important uniformization of outcome measures in future research on this topic. This would allow a more accurate comparison between studies and find more solid evidence about the effect of grandparenting on grandparent’s cognition.