INTRODUCTION
Borderline personality disorder (BPD), commonly known as a clinically severe and impairing disorder, is characterized with “a pervasive pattern of instability of interpersonal relationships, self-image, and affects, and marked impulsivity that begins by early adulthood and is present in a variety of contexts” according to the Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-5) [1]. However, the traditional BPD diagnosis showed many limitations including inadequate coverage of personality psychopathology variance, excessive comorbidity, within-disorder heterogeneity, loss of sub-threshold information, and diagnostic instability [2,3].
To solve these issues, DSM-5 proposed an alternative model of personality disorder (AMPD) with dimensional domains [1]. This domain-level trait model is based on dimensional models of personality such as the Personality Psychopathology Five (PSY-5), which includes antagonism, disinhibition, negative affectivity, detachment, and psychoticism as five domains [4]. At the measurement level, PSY-5 scales were developed onto the Minnesota Multiphasic Personality Inventory-2 (MMPI-2) item pool to evaluate the PSY-5 domains [4]. The MMPI-2 PSY-5 scales are aggressiveness (AGGR), disconstraint (DISC), negative emotionality/neuroticism (NEGE), introversion/low positive emotionality (INTR) and psychoticism (PSYC), which are parallel with original PSY-5 domains respectively. Many studies have successfully reported associations between the MMPI-2 PSY-5 scales and personality disorder symptoms [5-9]. Particularly, BPD symptoms were best predicted by PSYC and NEGE [9,10] and/or DISC [8,11] with AGGR [8] among PSY-5 dimensions.
Studies examining relationship between the MMPI-2 PSY-5 scales and BPD utilized various measurements such as the Structured Interview for DSM-IV Personality (SIDP-R) [6], the Personality Disorder Questionnaire-Revised (PDQ-R) [8], the Structured Clinical Interview for DSM-IV Axis II (SCID-II) [6,9], and the Personality Assessment Inventory (PAI) [7]. Among them, PAI proposed borderline features (PAI-BOR) scale which captures maladaptive behaviors of BPD in four core dysfunctional symptoms including affective instability (BOR-A), the identity problems (BOR-I), the negative relationships (BOR-N), and the self-harm behaviors (BOR-S) [12]. The PAI-BOR is one of the best-studied measurement of BPD features and has been used widely in both research and clinical settings [13].
Therefore, the purpose of this study is to understand BPD features with PSY-5 dimensional domains in MMPI-2 in Korean clinical samples.
METHODS
Participants
Participants were in- and out-patients who visited the psychiatry department of a university hospital in Iksan, Korea, from March 2015 to March 2019, and their data were collected anonymously. Individuals with severe psychotic symptoms assessed by clinicians as well as individuals with invalid MMPI-2 results (>80 T-scores on the VRIN and TRIN scales, or >30 points on the “cannot-say” scale) were excluded. Final samples consisted of 101 (64.7%) men and 55 (35.3%) women with a mean age of 34.15 years (SD=15.79). Participants represented a wide range of single and comorbid psychiatric discharge diagnoses, including depressive disorders (40.4%), psychotic disorders (12.2%), anxiety disorders (11.5%), adjustment disorder (11.5%), post-traumatic stress disorder (8.3%), bipolar disorders (3.8%), substance use disorder (3.2%), and other disorders (8.3%). The study was conducted after obtaining the approval of the Institutional Review Board of the Wonkwang University Hospital (IRB No. WKUH 2021-02-003).
Measures
PAI-BOR
The Korean version of PAI-BOR [15] was used to assess BPD features, including affective instability (BOR-A; e.g., “my mood could shift quite suddenly”), identity problems (BOR-I; e.g., “my attitude about myself changed a lot”), negative relationships (BOR-N; e.g., “my relationships have been stormy”), and self-harm (BOR-S; e.g., “I was a reckless person). It consists of 24 items and is assessed with a 4-point Likert scale from 0 (False, Not True at All) to 4 (Very True).
Statistical analysis
Descriptive statistics including frequency, mean, and standardized deviation were performed. Normality was tested for each variable before further analysis. Skewness over 2.0 and kurtosis over 7.0 were considered to reflect a moderately nonnormal distribution [16]. Skewness of AGGR, PSYC, DISC, NEGE, INTR, BOR-A, BOR-I, BOR-N, BOR-S, and BOR-total were 0.571, 0.453, 0.986, 0.011, 0.25, 0.357, 0.039, -0.174, 0.857, and 0.335, respectively. Kurtosis of AGGR, PSYC, DISC, NEGE, INTR, BOR-A, BOR-I, BOR-N, BOR-S, and BOR-total were 2.917, 2.594, 3.856, 1.953, 2.095, 2.706, 2.313, 2.709, 3.282, and 2.996, respectively. Thus, all variables were within the range of normal distribution for further parametric statistics.
The Pearson’s partial correlation analysis was performed with MMPI-2 PSY-5 scales and PAI-BOR subscales while controlling for the effect of age and gender with 1,000 times of bootstrapping process.
Based on the correlation results, the hierarchical multiple regression analysis was performed to discover predictors for PAI-BOR among PSY-5 scales. The enter method was used with 1,000 times of bootstrapping process for the hierarchical regression analysis. Age and gender were included as covariates to control for the contaminating effect.
In addition, path analyses were performed to discover predictors of PAI-BOR subscales among PSY-5 scales using maximum likelihood estimation. Age and gender were also included as covariates. Chi-square test (χ2), comparative fit index (CFI), normed fit index (NFI), Tucker-Lewis index (TLI), and root mean square error of approximation (RMSEA) indices were used to examine the goodness of fit of the path model. Cutoff points of indices were: CFI, NFI, TLI >0.90 and RMSEA <0.08 [17]. All statistical analyses were conducted by SPSS 25.0 (IBM Corp., Armonk, NY, USA) and AMOS 25.0 (SPSS Inc., Chicago, IL, USA), and the significant level was set at p<0.05 (two-tailed).
RESULTS
Descriptive statistics and correlation analysis
The demographic characteristics of participants are provided in Table 1.
The correlation analysis was performed with all variables including demographic characteristics. Since age and gender were significantly correlated with the BOR-total score (r=-0.295, p<0.00; r=-0.170, p=0.034, respectively), the partial correlation analysis was performed to control the effect of age and gender on the BOR score. Correlation coefficients, mean, and standard deviation of all variables are presented in Table 2.
The BOR-total score was significantly correlated with all MMPI-2 PSY-5 scales even after controlling for the effect of age and gender. BOR-A and BOR-N showed significant relationship with all PSY-5 scales. On the other hand, BOR-I showed significant correlation with PSYC, NEGE, and INTR, but not with AGGR (r=0.122, p=0.132) nor DISC (r=0.072, p=0.037). BOR-S also showed significant correlation with AGGR, PSYC, DISC, and NEGE, but not with INTR (r=0.137, p=0.089).
Regression analysis
Based on the correlation analysis, hierarchical multiple regression analysis was performed to discover significant predictors of BOR-total score among PSY-5 scales. Age and gender were entered at step one as covariates, and all PSY-5 scales were entered at step two. The result of hierarchical multiple regression is shown in Table 3.
The hierarchical multiple regression revealed that at step one, age and gender contributed significantly to the regression model (F(2,153)=8.09, p<0.001) and accounted for 10% of the variance in the BOR-total score. Adding PSY-5 scales at step two explained an additional 57% of variance in the BOR-total score and this change in R2 was significant (F(7,148)=67.24, p<0.001). When all seven variables were included in step two of the regression model, neither gender nor the PSYC scale were significant predictors of the BOR-total score (t=-0.418, p=0.677; t=0.628, p=0.531, respectively).
Path analysis
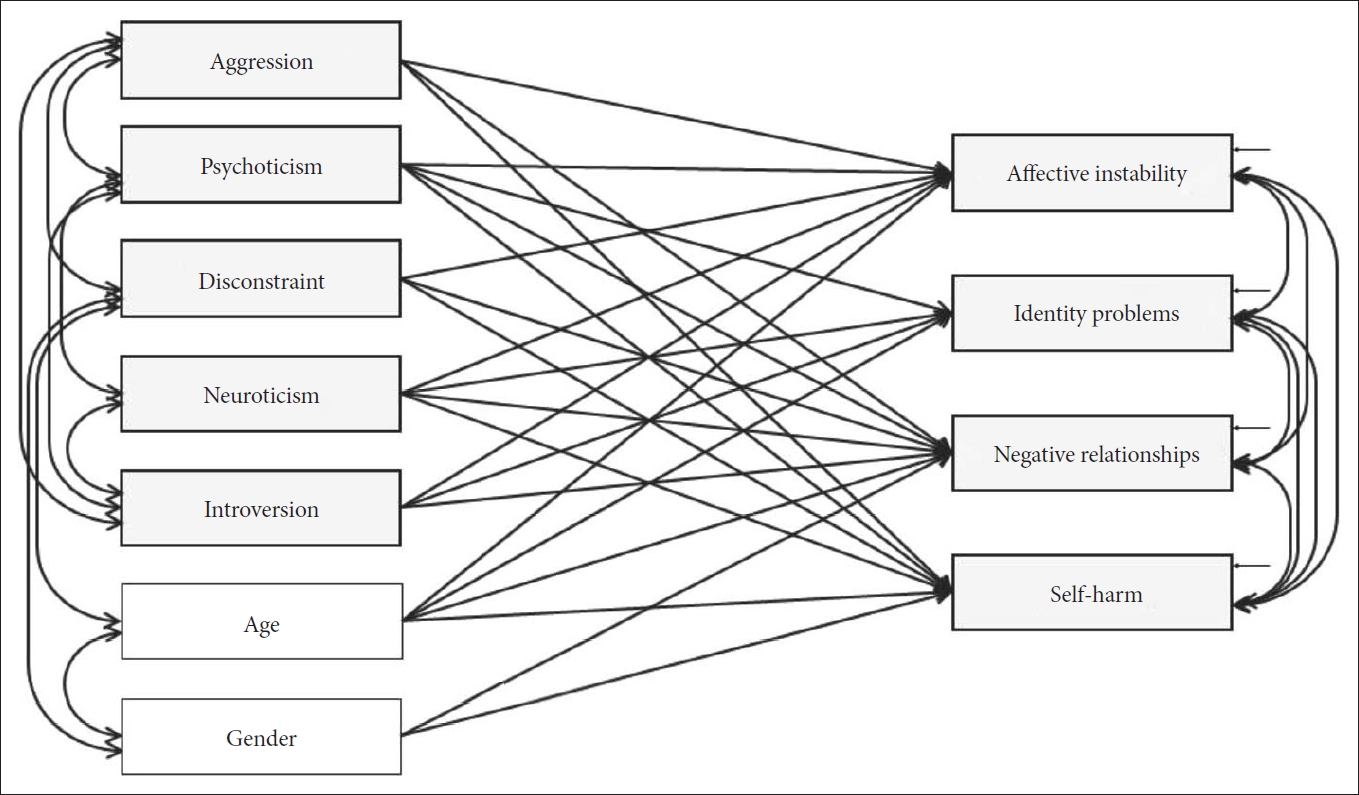
To examine detailed relationships among PSY-5 scales with BOR subscales, the path analysis was performed. A hypothesized model was driven based on the significant relationships from the correlation analysis. Figure 1 presents the hypothesized model based on the correlation analysis.
The result of the path analysis revealed that some paths were not significant in the hypothesized model. The path between AGGR and BOR-N (β=0.136, p=0.073), AGGR and BOR-S (β= 0.007, p=0.922), PSYC and BOR-I (β=0.085, p=0.252), INTR and BOR-I (β=0.100, p=0.106), PSYC and BOR-A (β=-0.015, p=0.831), PSYC and BOR-N (β=0.055, p=0.514), INTR and BOR-N (β=0.137, p=0.076), PSYC and BOR-S (β=0.041, p= 0.583), INTR and BOR-S (β=0.045, p=0.507), age and BOR-A (β=-0.077, p=0.155), age and BOR-N (β=-0.085, p=0.204), gender and BOR-N (β=-0.065, p=0.318), and gender and BOR-S (β=0.008, p=0.895) were excluded from the hypothesized model. In addition, the correlation path between AGGR and NEGE (r=0.146, p=0.072), PSYC and DISC (r=0.141, p=0.079), DISC and NEGE (r=0.086, p=0.262), DISC and INTR (r=-0.144, p=0.063), and the error of BOR-N and the error of BOR-S (r=0.110, p=0.175) were also excluded from the hypothesized model.
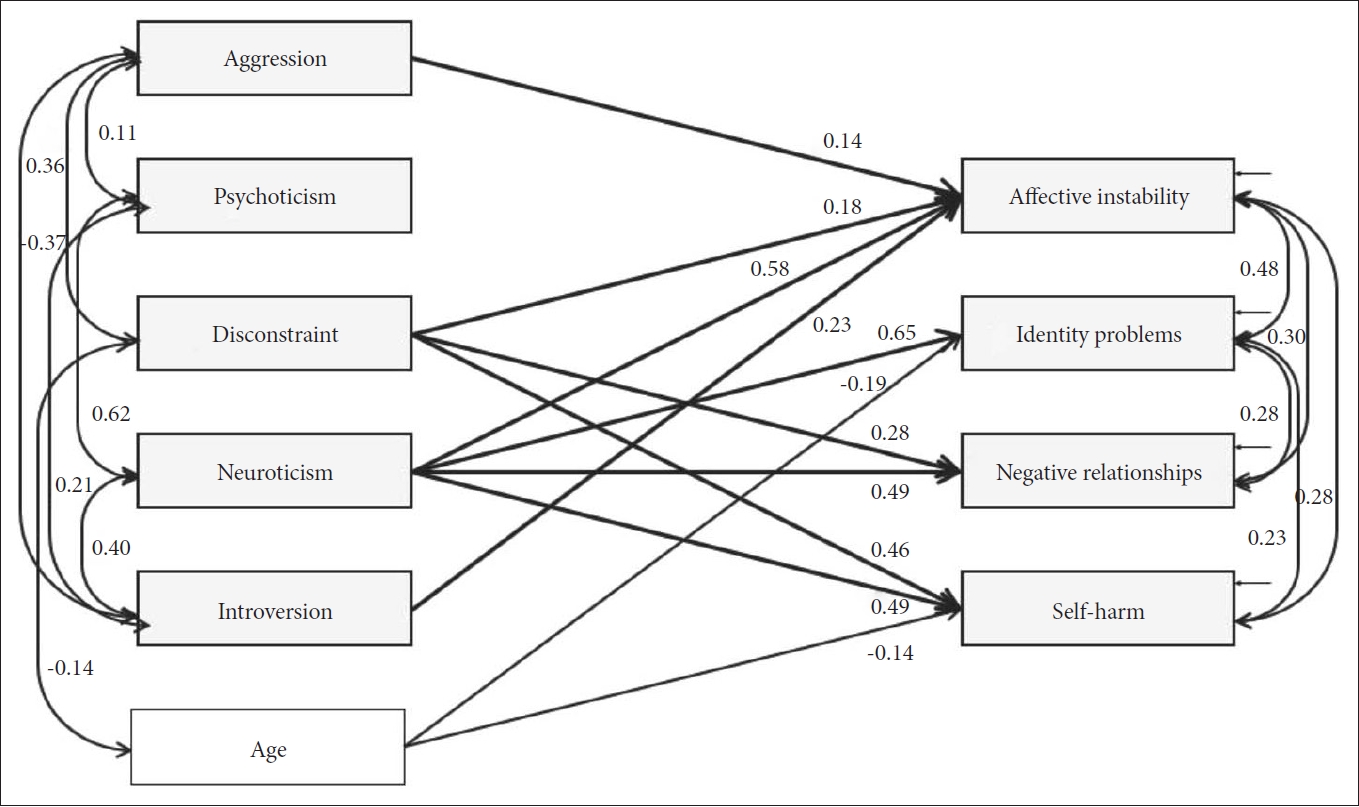
The final model with significant paths and correlations was analyzed. This model showed great fit since χ2 (22)=31.032, p=0.095, CFI=0.986, NFI=0.955, TLI=0.971, and RMSEA=0.051. Figure 2 presents the final model with significant paths and standardized parameter estimates and Table 4 shows standardized regression weights and standard errors of the model. BOR-A was significantly predicted by AGGR, DISC, NEGE, and INTR. BOR-I was significantly predicted by NEGE and age. BOR-N was significantly predicted by DISC and NEGE. BOR-S was significantly predicted by DISC, NEGE and age.
DISCUSSION
Based on the PSY-5 domain theory, this study aimed to predict BPD features by utilizing MMPI-2 PSY-5 scales as an extension of the AMPD. Therefore, this study employed MMPI-2, which is commonly used in clinical practices, and PAI-BOR, which is a reliable indicator reflecting BPD features.
The findings indicate that AGGR, DISC, NEGE, and INTR were significant predictors of the PAI-BOR total scores. Moreover, NEGE was the most significant predictor of the BOR-total (β=0.569, p<0.001), followed by DISC (β=0.237, p<0.001), INTR (β=0.189, p=0.001), and AGGR (β=0.132, p=0.001), whereas PSYC did not significantly predict the PAI-BOR total score (β=0.039, p=0.531). These results are in line with previous findings [6,7,11].
For each PSY-5 scale, the findings from path analyses suggest that AGGR, DISC, NEGE, and INTR predicted BOR-A, NEGE and age predicted BOR-I, DISC and NEGE predicted BOR-N, and NEGE, DISC, and age predicted BOR-S. In other words, NEGE significantly predicted all the PAI-BOR subscales, while PSYC did not significantly predict any subscale. Similarly, DISC significantly predicted three subscales: BOR-A, BOR-N, and BOR-S; however, AGGR or INTR significantly predicted only BOR-A. In summary, PSY-5 domains NEGE and DISC are key predictors associated with BPD features. Neuroticism, represented as NEGE, is the characteristic trait reflecting BPD’s core symptoms [18,19], which reflects emotional instability and a tendency to experience negative emotions [20]. Additionally, disconstraint, represented as DISC, describes symptoms along with the behavioral dysregulation and impulsivity of BPD [21,22]. The results of this study are in line with the existing literature indicating that eight out of nine symptoms of DSM-5 BPD criteria are related to NEGE and DISC [23].
In contrast, PSYC was the only scale that exhibited no significant prediction of BPD features among all PSY-5 domains. Although some studies have demonstrated the association between PSYC and BPD [6,11], other studies have not shown this association significantly [7]. Such discrepancies appear owing to the differences in study methods. Similarly, a significant correlation was found between PSYC and BOR-total in the correlation analysis; however, in the regression analysis and path analysis where all PSY-5 scales were presented, PSYC was not found to be a significant predictor of the BOR-total and subscale scores. This is because NEGE and DISC explain BPD symptoms accurately [23]. Although PSYC is related to the stress-induced paranoia and dissociative experiences of BPD [24], PSYC typically explains bizarre and disorganized features such as disconnection from reality, including unshared beliefs and unusual perceptual experiences [25]. Thus, when accompanied by other PSY-5 scales, its explanatory power weakens. Therefore, in this study, it can be concluded that PSYC is not a core personality domain that explains BPD.
The study added age and gender as covariates to see the pure predictive effects of PSY-5 on BOR-total and BOR scales. As a result, age significantly predicted the BOR-total, which revealed that the younger the patient is, the more intensive is the BPD symptom. Moreover, age significantly predicted BOR-I and BOR-S, which illustrates that the younger the patient, the greater is the intensity with which they experience these episodes. According to previous studies, BPD showed advanced symptoms in early adulthood and they gradually stabilized with aging [26,27]; as such, the results of this study are consistent with those of previous studies and add to the literature. It has been established that BPD patients, especially younger patients, are more vulnerable to identity disturbance [28], along with suicidal and other self-harming behavior [29]. Therefore, this study’s results also highlight the importance of considering the influence of age when predicting BPD.
Gender showed significant correlations with BOR-total and BOR subscales, but not in the regression nor path analyses. In fact, many studies have reported that the gender difference of BPD is not significant [30,31], and gender might not be an appropriate general predictor of BPD since the gender difference could be explained by cultural underpinnings [32]. Likewise, this study supports that gender is not considered preferentially when predicting BPD symptoms.
This study is meaningful in that it attempted to find a personality domain for predicting BPD and various BPD sub-symptoms in South Korean clinical samples. Various problems with existing diagnostic criteria relating to BPD have been reported and they present challenges in making diagnoses in clinical practice [2,3]. Thus, there have been constant efforts to understand BPD features through the PSY-5 domain. This study reveals that the PSY-5 theory can help predict BPD symptoms in South Korean clinical samples, which can also be referenced in understanding patients and determining diagnoses in clinical practice. Furthermore, since the study was conducted using MMPI-2 and PAI, which are widely used in clinical practice, the results of this study can be referenced and applied without great difficulty in clinical practice to help predict and understand BPD features in the early stages.
This study has several limitations. First, different diagnostic groups were represented together. Additional studies to explain the diagnosis and symptoms using PSY-5 by recruiting patients with only BPD should be performed. Furthermore, expanding the study to non-clinical samples could contribute to the early detection and support of BPD vulnerabilities in a community. In addition, since this study used MMPI-2 and PAI, which are self-evaluated tests, it is necessary to attempt to understand BPD objectively using other biological tests such as EEG, biochemical markers, and structural brain indices.
In conclusion, this study sought to determine whether MMPI-2 PSY-5 scales significantly predict BPD features among South Korean clinical samples. The results indicate that NEGE, DISC, AGGR, and INTR significantly predict the BOR-total and BOR subscales, and of these, NEGE is the key predictor that best describes BPD features. Finally, age also predicts the BOR-total, BOR-I, and BOR-S, revealing that young age plays a key role in understanding BPD features.