INTRODUCTION
Suicide is a problematic social phenomenon globally, and the incidence rate is steadily increasing [1,2]. It not only claims the lives of individuals, but also emotionally traumatizes the family members of those who complete suicide3 and causes significant social loss nationally [4,5]. The severity of the suicide problem has created a new perspective which considers suicide to be an independent mental health problem or disease status, rather than simply an outcome of mental illness, such as depression, as reflected in the existing view [6,7]. Middle-aged adults are an economically active group [8], and suicidality in this age group can have an especially devastating effect. Therefore, identification of factors affecting suicidality in this age group is considered important for prevention.
Marital and occupational status are also known to be associated with suicide. Some studies found high suicide risks among divorced, widowed, never married, or cohabiting individuals compared to currently married individuals [9-11]. Contrarily, others reported lower suicide rates among widowed and divorced individuals, compared to married persons[12,13].
Furthermore, previous ecological research indicated that the national rate of male suicides correlated with the unemployment rate [14,15]. Moreover, job insecurity was also shown to trigger depression and suicidal ideation [16,17]. However, other studies have contradicted these findings [18,19]. In a study conducted in Korea, manual workers experienced more suicidal ideation than non-manual workers. Therefore, it appears that not only the status of employment, but also the quality of and satisfaction with the job are related to suicidal ideation [20]. These results suggest that marital and occupational status may act as risk factors for suicide; however, other factors may also mediate or interact with this association, such as personality. In the meantime, marital and occupational status are data that can be investigated relatively easily at the national level, and confirming their influence on suicide, either independently or in interaction with other factors, could help establish overall measures for suicide prevention.
Personality has been examined in various studies using several measurement tools. The widely used Five-Factor Model (FFM) quantifies personality characteristics in five dimensions: openness, conscientiousness, extraversion, agreeableness, and neuroticism [21]. Openness means “friendly/compassionate vs. critical/rational,” conscientiousness is “efficient/organized vs. extravagant/careless,” extraversion is “outgoing/energetic vs. solitary/reserved,” agreeableness is “friendly/compassionate vs. critical/rational,” and neuroticism is “sensitive/nervous vs. resilient/confident.” [22] These five personality factors are known to represent basic dimensions of human personality in various languages and cultures [23-26]. Also, the FFM has strong predictive validity [27,28], interrater agreement [29], and heritability [30]. The relationship between the FFM personality traits and suicide has been well-researched in various prior studies. High neuroticism is consistently reported to be related to suicide [31-33]. Extraversion and conscientiousness have yielded controversial results [34-36]. Some studies suggested that openness may be associated with increased suicidal ideation [37,38]. However, in most studies, agreeableness was not associated with suicide [39,40]. These inconsistent results may indicate the possibility of interaction or mediation by other risk factors in the relationship between personality and suicide. For example, social support or isolation could play an important role in this relationship.
As suggested above, marital status, occupational status, personality, and sex directly or indirectly affect suicidality, and a complex interaction between each factor is thought to exist. This interaction can be explained through the “diathesis-stressor model.” According to this model, suicidality is the result of an interaction between an acute negative condition (stressor) and the corresponding vulnerability trait (the diathesis) [41]. In this study, occupational status and marital status were considered stressors, with personality and sex considered the diatheses, and the effect of their interaction on suicidality was explored.
Hence, the present study aimed to investigate how marital status, occupational status, and personality influence suicidal ideation and behaviors among a group of middle-aged Korean people. The findings may help establish an intervention model by identifying the independent and interacting influences in this relationship.
METHODS
Data collection and participants
The data used in this study were taken from the 2011 Korean Epidemiologic Catchment Area (KECA) study, which is a nationally representative survey. The KECA evaluated the prevalence of major psychiatric disorders using the structured interview manual based on the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) [42,43]. The participants were selected from the 2010 population census data using a stratified, multi-stage, and clustered sampling design. The household residents aged between 18 and 74 years, excluding institutionalized individuals, were chosen. For representative sample extraction, a total of 246 sampling units were selected from 61 subdivisions extracted from 12 catchment areas. Out of a total of 14,204 households, at least one household was nominated from each sampling unit, and one individual per household was randomly selected. After eliminating those who did not meet the study criteria or refused to participate, 6,022 participants were included [42]. Among them, 2,464 males and females between the ages of 40 to 59 years who had responded to the questionnaire about suicidality in the past year were included in this study. All procedures of the study protocol were approved by the Institutional Review Board of Seoul National University College of Medicine (IRB No. C-1104-092-359). All participants were fully informed of the study objectives and written informed consent was obtained from them before their participation. Furthermore, all methods were carried out in adherence to relevant guidelines and regulations. The dataset is available upon reasonable request to the corresponding author.
Measures
One-year suicidality
This study used the Korean version of the Composite International Diagnostic Interview (K-CIDI), which is a popular structured diagnostic tool used worldwide [44,45]. We used the KCIDI module on suicide to assess lifetime suicidality. Lifetime suicidal ideation was assessed using the item, “Have you ever seriously thought of committing suicide?” A lifetime suicide plan was examined with the item, “Have you ever concretely planned a suicide?” Lifetime suicide attempts were assessed with the item, “Have you ever attempted suicide?” Moreover, the number of suicide attempts was recorded. Suicidality was defined as either suicidal ideation, planning, or attempts. The participants were also asked about their age at the time of the first and last suicidal ideation, planning, and attempt. In this way, we defined whether participants had “1-year suicidality” over the past year.
Big Five Inventory-11
Personality was assessed using the 11-item version of the Big Five Inventory (BFI-11), with two items for each personality domain, except agreeableness, which has three. Each item is scored on a 5-point Likert scale ranging from 1 (“strongly disagree”) to 5 (“strongly agree”), following the statement “I see myself as someone who….” Items for extraversion are numbered 1R (“…is reserved”) and 6 (“…is outgoing, sociable”). Agreeableness items are numbered 2 (“…is generally trusting”), 7R (“…tends to find fault with others”), and 11 (“…is understanding and kind to almost everyone”). Conscientiousness items are numbered 3R (“…tends to be lazy”) and 8 (“…does a thorough job”). Neuroticism items are numbered 4R (“…is relaxed, handles stress well”) and 9 (“…gets nervous easily”). Finally, openness items are numbered 5R (“…has few artistic interests”) and 10 (“…has an active imagination”). Here, the initial “R” indicates that the item is reverse scored [46,47]. The score for each personality domain was the sum of the points for each item, or, in the case of reverse-scored items, the score was calculated by subtracting six from the point of each personality factor item.
Marital status and occupational status
To evaluate marital status, a questionnaire was administered to determine whether participants were currently married, widowed, separated, divorced, or had never been married. In the subsequent analysis, to ascertain the importance of maintaining a stable marriage, the marital status category was divided into two categories: “maintaining (currently married)” or “not maintaining (widowed, separated, divorced, or had never been married).” Occupational status was categorized into full-time, part-time, and unemployed. This category was applied in the subsequent analysis.
Physical illness
To evaluate the participants’ physical condition, a medical history of diabetes or hyperglycemia, hypertension, hyperlipidemia, stroke, heart disease, and cancer was evaluated. According to the methods of a previous study, if any of the six diseases were present, physical illness was coded “1” (positive). However, cases with no disease history were coded as “0” (negative) [48].
One-year major depressive episode
Major depressive disorder is known to significantly increase the risk of suicide49 and significantly affect marital failure [50] and unemployment [51]. Therefore, major depressive disorder could be a significant confounding factor in this study. Hence, major depressive disorder was added as a covariate among major psychiatric disorders investigated in this 2011 KECA study. The presence of “at least one major depressive episode in the past year” was investigated using a structured interview based on DSM-IV [45].
Other covariates
Self-reported data on demographic characteristics, including age, sex, residential area, years of education, and monthly income, were surveyed in this study. Age was recorded in units of years and subsequently used for analysis as a continuous variable. Other covariates were categorized. Education level was classified into groups including “not formally educated,” “below elementary school,” “below high school,” and “high school and above.” Monthly income was classified as “less than 2 million won,” “more than 2 million won and less than 3 million won,” and “more than 3 million won.” The residential area was classified as “rural” or “urban.”
Data analysis
Statistical analysis was conducted using IBM SPSS Statistics for Windows, version 24.0 (IBM Corp., Armonk, NY, USA) The significance level was based on a two-tailed p-value of 0.05. First, differences in demographic and clinical variables were compared between the groups with and without 1-year suicidality. The t-test was used for continuous variables and the Pearson Chi-square test was used for categorical variables.
Next, a generalized linear model (GLM) analysis was performed, correcting for all the covariates together (age, education, income, region, chronic illness, and 1-year major depressive episode). The five personality traits and marital status (reference: maintaining) and occupational status (reference: full-time) were the independent variables. The dependent variable was 1-year suicidality. Thereafter, interaction terms between independent variables were added to analytic models to investigate the interaction effects. Among the personality traits, variables that had significant association (p<0.10) on initial GLM were selected. Personality×marital status (occupational status), and marital status (occupational status)× sex were assessed for a two-way interaction effect. Furthermore, stratified subgroup analysis was performed on variables whose interaction was significant in the GLM analysis to confirm the interaction effect.
RESULTS
Characteristics of the study sample
Of the 2,464 participants, 96 had a history of suicidality in the past year (1-year suicidality). Suicidal ideas or plans accounted for 3.9% (96/2,464) of the total, whereas suicide attempts represented only 0.3% (9/2,464). Moreover, everyone who attempted suicide had suicidal ideas or plans. There were no significant differences in age, sex, residential area, chronic illness, and marital status in the groups with and without 1-year suicidality. However, participants with 1-year suicidality had lower levels of education, income, and full-time employment, and higher levels of part-time employment and unemployment. The proportion of participants with a major depressive episode was larger in the group with 1-year suicidality (Table 1).
In the five personality domains, neuroticism was significantly higher in the group with 1-year suicidality, and conscientiousness and extraversion were significantly lower. No significant difference was found between openness and agreeableness (Table 1).
Effects of marital status, occupational status, and personality on 1-year suicidality
Marital status was divided into two categories: “maintaining (currently married)” or “not maintaining (widowed, separated, divorced, or had never been married).” Results of GLM analysis, in which each independent variable of interest was added with a covariate (age, sex, education, region, income, chronic illness, and major depressive episode), revealed that marital status (not maintaining: odd ratio [OR]=1.131, 95% confidence interval [CI]=0.644-1.988) and occupational status (part-time: OR=1.874, 95% CI=0.952-3.689; unemployed: OR=1.007, 95% CI=0.531-1.910) were not significantly associated with 1-year suicidality (Table 2). Among the personality domains, a positive association was significant for neuroticism (OR=1.199, 95% CI=1.057-1.360) and openness (OR=1.145, 95% CI=1.004-1.307). A negative association was significant for extraversion (OR=0.840, 95% CI=0.748- 0.944); conscientiousness was statistically not significant but showed a trend for significance (OR=0.882, 95% CI=0.773- 1.007). Agreeableness was not significantly associated (OR=0.938, 95% CI=0.846-1.039); therefore, it was excluded from subsequent analyses (Table 2).
Interaction effect of marital status, occupational status, personality, and sex on 1-year suicidality
The results indicated that marital status (not maintaining: OR=1.181, 95% CI=0.408-3.419) and occupational status (part-time: OR=0.602, 95% CI=0.157-2.298; unemployed: OR=1.970, 95% CI=0.556-6.979) had no significant interaction effects with sex on 1-year suicidality (Table 3). However, neuroticism had a significant interaction with marital status (not maintaining: OR=1.346, 95% CI=1.002-1.808) (Table 4).
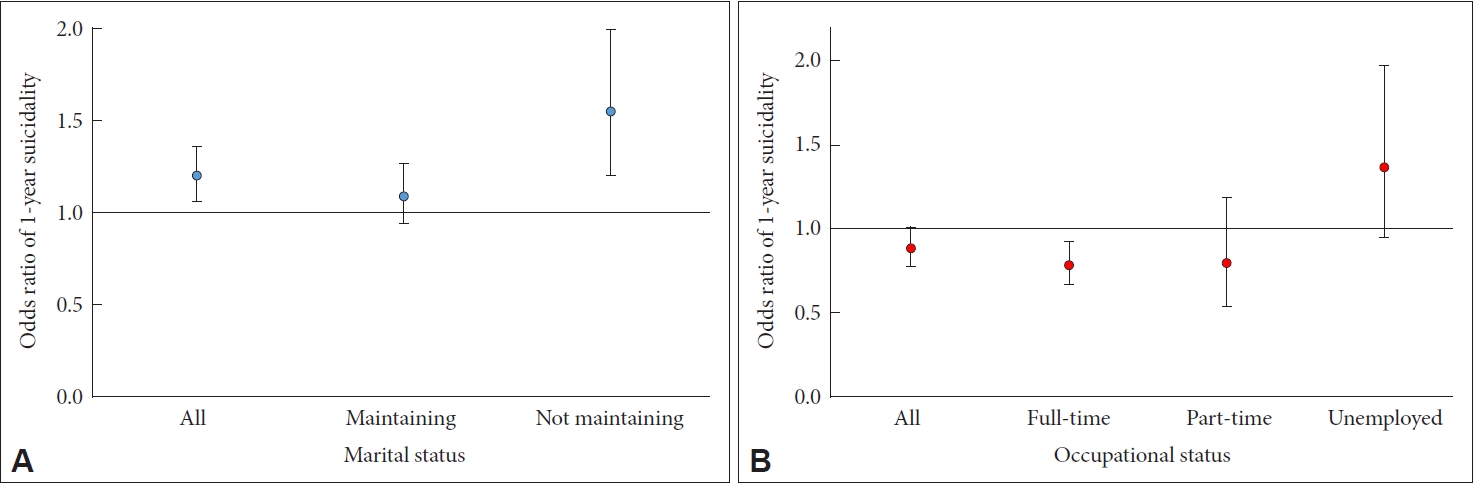
Conscientiousness had a significant interaction with occupational status (part-time: OR=1.122, 95% CI=0.788-1.598; unemployed: OR=1.534, 95% CI=1.074-2.193) (Table 5) Neither extraversion (Table 6) nor openness (Table 7) had a significant interaction with other variables. Subsequently, subgroup analyses of neuroticism×marital status, and conscientiousness× occupational status were performed. Neuroticism was found to be more closely associated with 1-year suicidality in the “not maintaining” group (OR=1.547, 95% CI=1.197- 1.999), but not in the “maintaining” group (OR=1.093, 95% CI=0.941-1.269). Furthermore, conscientiousness was negatively associated with 1-year suicidality in participants with full-time employment (OR=0.784, 95% CI=0.666-0.924). However, no significant association was found between parttime employment (OR=0.798, 95% CI=0.534-1.192) and unemployment (OR=1.371, 95% CI=0.950-1.979) (Figure 1).
DISCUSSION
This study aimed to determine how marital status, occupational status, and personality traits impact suicidality. The results of this study showed two main findings. First, the personality domains of neuroticism, extraversion, openness, and conscientiousness were significantly associated with 1-year suicidality, both in models with various confounders and in the multivariate model including social, marital, and occupational status. Second, marital and occupational status did not solely affect suicidality, and interacted with personality domains as well. The findings that neuroticism is positively associated with suicidality, and extraversion is negatively associated with suicidality, replicate the results of a meta-analysis [52]. While there are conflicting results regarding conscientiousness [53], some evidence implies it is negatively associated with suicidality [39,54]. Interestingly, openness (interest in art, rich imagination) had a significant positive association with suicidality, possibly because people with high openness may be more impulsive when faced with stressful situations [55]. Additionally, according to previous research, high openness accelerates engagement in risky behaviors [37]. Indeed, openness showed a positive association with suicidality in a clinical sample of depressed adults aged 50 years and above [38].
The finding of no significant association between marital status, occupational status, and suicidality can be interpreted in several ways. As mentioned in the introduction, previous research has yielded controversial results regarding the association between these statuses and suicide. This may be attributed to the heterogeneous characteristics of participants, including ethnicity, age, class, proportion of males, and source of control group (e.g., community, clinic, and deceased group). Furthermore, personal factors such as depression and substance abuse may interact with social factors (e.g., unemployment, no spouse or cohabitant) to influence suicide attempts, leading to suicide [56]. Similar to previous studies, our research showed that marital and occupational status may aggravate or attenuate the suicidality of vulnerable individuals, rather than induce suicidality. Neuroticism and conscientiousness were found to interact with marital status and occupational status, respectively, which supports the findings of prior studies as discussed above. If this result is applied to the existing diathesis-stressor model [41], unemployment and the inability to maintain marriage act as stressors, and high neuroticism and conscientiousness interact as diatheses to increase suicidality. Subsequent subgroup analyses indicated that participants in currently non-married categories were more prominently affected by neuroticism. For neurotic people susceptible to stress and sensitivity, the stress caused by divorce, bereavement, and living alone may act as an exacerbating factor [57]. Prior research examining the relationship between social proxies (including marital and occupational status) and suicide found that the results were related to the characteristics of the study group. Unmarried status was a risk factor in the group, which mainly comprised married people, and unemployment was a risk factor in the group with mostly employed participants [58]. Marriage is a standardized cultural criterion for middle-aged Korean adults, and failure to maintain marital status may cause feelings of thwarted belongingness, because such individuals might feel that they have deviated from the conventional norms of the mainstream group [59]. These stressors may increase the risk of suicide in temperamentally vulnerable, or neurotic individuals.
Full-time employment showed a protective effect on suicidality among more conscientious participants. Conscientiousness is a personality trait related to diligence and thoroughness. Thus, it plays a pivotal role in an individual’s ability to maintain a stable job and has a positive role in maintaining self-esteem [60], and may have a protective effect on suicidality. Part-time employment has been reported to increase suicide risk due to job insecurity [61]. In this study, in the model without personality variables, the OR of part-time employment was higher than that of unemployment (Table 2), although it was not statistically significant. However, part-time employment× conscientiousness was not significant, and the OR was lower compared to that of the unemployment group in the subgroup analysis. This may be because participants with high conscientiousness hold a high regard for maintaining employment. Therefore, it can be assumed that working consistently, even at an unstable job, is more helpful in maintaining positive emotions than being unemployed. Meanwhile, according to a previous study, high conscientiousness was suggested to increase suicide risk in older adults, which was considered to be related to higher responsibilities and striving for achievement [62]. In view of this, one can also estimate that high conscientiousness might increase suicide risk in those with parttime jobs or who are unemployed. In fact, for unemployment status in this analysis, the OR of conscientiousness was higher than 1, despite it being statistically insignificant.
The clinical implication of this study is that both personal and social factors should be considered when planning interventions to prevent suicide. It is important to select the target population whose risk factors have a stronger impact on suicidality, especially when creating active intervention policies for population groups who are living alone and are unemployed. Given that marriage and occupation can be indexed, they are also major targets of social welfare policies. Therefore, it can be of practical help to consider personality and sex when formulating marriage- and occupation-related policies
This study has several strengths. First, the sample was extracted as a representative group of Korean adults by a rigorous statistical method. Owing to these methodological advantages, the results of this study can be generalized to the entire population of Korean middle-aged adults. Furthermore, the results of this survey were not self-reported, but were obtained face-to-face by well-trained interviewers. The results can also be considered reliable as structured tools that have been validated and tested in large-scale epidemiological studies. Finally, this study included more than 2,400 large-scale community participants and measured various demographic and clinical variables, which increases the generalizability of the findings.
However, this study also has several limitations. First, suicidal ideation, suicidal plan, and suicide attempt were pooled as one variable named “suicidality.” According to previous studies, risk factors for suicidal ideation and suicide attempt were different [63]. Therefore, if the variables were analyzed separately, the results of this study might have been different. However, in this study, only nine participants (0.3%) reported a 1-year suicidal attempt, so it was difficult to derive statistically significant results. We believe that the number of participants should be supplemented in future large-scale observation studies.
Second, as the design of this study is cross-sectional, we were unable to reveal any temporal and causal relationships. However, since 1-year suicidality was only evaluated for the past year, the possibility of changes in personality or socioeconomic status due to suicidality is relatively low. Nevertheless, the possibility of reverse causality cannot be eliminated. Therefore, large-scale, community-based studies with a longitudinal design should be conducted.
Finally, indicators of socioeconomic status and interpersonal relationships were not included except for marital and occupational status. For example, previous studies have suggested that friendship has a protective effect on suicide risk.64 Therefore, this study should be interpreted in terms of marital and occupational status rather than overall “social support.”
In conclusion, personality may be useful as a predictor of suicidality among middle-aged adults. Furthermore, marital status, occupational status, and sex may influence suicidality by interacting with personality. Hence, individualized social and psychological interventions according to individual personality traits are required for suicide prevention.