INTRODUCTION
Posttraumatic stress disorder (PTSD) is a psychiatric disorder, induced when an individual is exposed to a traumatic life event, resulting in impairments in the individual’s overall daily life functioning. Difficulties in emotional control and negative changes in thinking and mood often develop into chronic PTSD (CPTSD), hindering an individual’s ability to engage in social interactions, and leading to extreme mental distress that can impede their relationships or economic life [1].
Experts use interview tools and patient-reported outcome measurements (PROMs) to diagnose PTSD symptoms. PROMs are structured and standardized self-assessment tools that assess symptoms, functional condition, and quality of life based on the patient’s direct experience, with the goal of determining treatment outcomes [2]. In PTSD treatment, PROMs provide researchers with information regarding the patient’s perception of their symptoms, and how these symptoms affect their overall function and relationships with others. Therefore, PROMs are essential communication and feedback tools for PTSD diagnosis that goes beyond reporting health and treatment-related satisfaction or feelings [3].
To allow for the clinical application of mental health PROMs, there is a need to elucidate the nature of the trauma experienced by individuals and the social culture. Since post-traumatic psychological adaptation is more dependent on how an event is perceived and accepted than on the diagnostic criteria for PTSD, it is crucial to consider the cultural characteristics related to the individual’s traumatic experience. Therefore, it is essential to assess PTSD and related symptoms from the onset of the traumatic event and to consider these factors when surveying appropriate interventions to prevent the development of CPTSD [4,5].
As of December 2022, a total of 33,882 North Korean defectors had escaped from North Korea and settled in South Korea [6]. During their escape, defectors experience both physical and mental trauma, including separation from family members, detention in labor/political prison camps, public executions, torture, beatings, punishment, and prostitution [7-10]. The lifetime prevalence of PTSD among North Korean defectors is 15.3 times higher than that among South Koreans [11].
So far various measurements have been used to study PTSD, including partial PTSD, among North Korean defectors; the diagnostic criteria were based on the Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV) [12]. Thus, it has been found that the prevalence rates vary according to the type or characteristics of each tool [13]. Using tools whose suitability has not been reviewed is likely to present distorted research results [14], and the degree of support for interpretation or theory of research results may be insufficient [15,16].
This scoping review aimed to identify the current use of PROMs and determine the properties of each measurement used in studies on PTSD among North Korean defectors. To identify the appropriate tools for research and clinical practice [17], the COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN) classification and checklist for evaluating self-reporting measurement tools were used [18]. The findings of this study could inform the selection of appropriate measurement tools for evaluating PTSD symptoms among North Korean defectors.
METHODS
Literature search strategy
A systematic literature search was conducted according to the COSMIN methodology through four databases: Research Information Sharing Service, ScienceON, PubMed, and Embase from their inception up to September 15, 2022. To identify all PROMs that have been used to detect PTSD in North Korean defectors, we used the following two search elements, the construct of interest (PTSD) and population (North Korean defectors), as follows: (((((Post-Traumatic Stress Disorder) OR (post-traumatic stress disorders)) OR (mental health trauma)) OR (psychiatry*)) OR (psychology*)) AND (((((North Korean defectors) OR (North Korean refugees)) OR (North Korean immigrants)) OR (Saetemin)) OR (North Korean emigrants)). The search term for the type of instrument and measurement properties were not applied because our study aimed to identify all PROMs that have been used for North Korean defectors. Search terms on the construct and study population of interest were reviewed by the librarian to expand the search with the appropriate terms.
Eligibility criteria
The inclusion criteria were: 1) papers published in English or Korean; 2) mental health and social adaptation papers that used PROMs to assess PTSD symptoms or major-related variables; and 3) papers involving North Korean defectors aged ≥19 years.
The exclusion criteria were: 1) papers that did not include PROMs to measure PTSD; 2) papers involving North Korean defectors aged <19 years; 3) papers involving North Korean defectors who do not live in South Korea; and 4) literature reviews, comments, qualitative research, and unpublished academic papers/research reports with unidentified original documents.
Data collection process
The data collection and selection were conducted independently by two researchers. In cases of disagreement between the researchers, the data were reviewed by a third researcher until a common consensus was reached. Retrieved data were managed using EndNote X9 (Clarivate, Philadelphia, PA, USA), a literature management program.
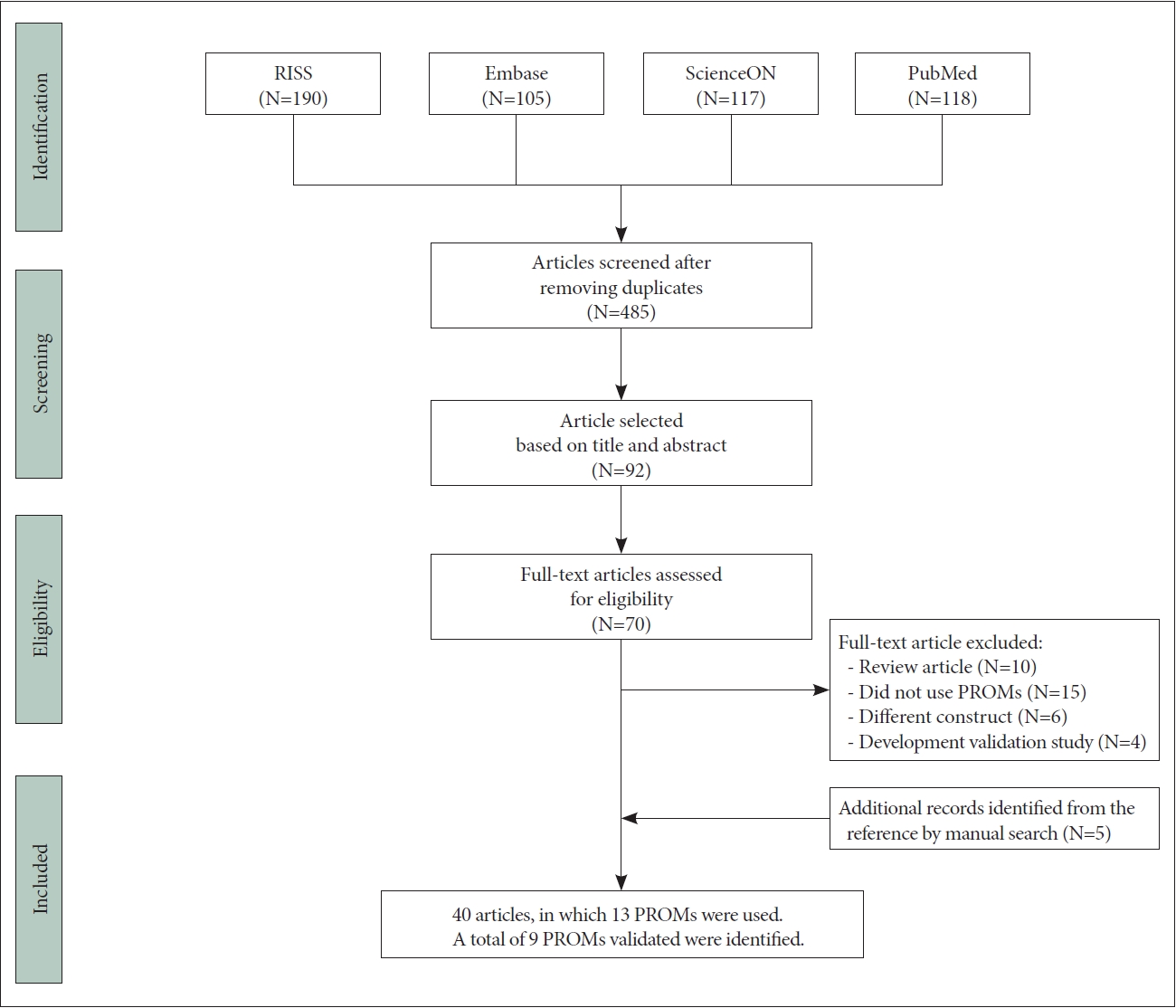
The process of selecting articles is presented as a flow chart of PRISMA (preferred reporting items for systematic review and meta-analysis) in Figure 1 [19]. After excluding duplicates, the electronic literature search yielded 485 articles. Initially, irrelevant studies were excluded by reviewing titles and abstracts and then 70 full-text articles were reviewed. The manual search based on the bibliographic references of the included studies yielded five additional studies. A total of 40 studies that used PROMs were reviewed in this study. Finally, we identified 9 validated PROMs, which were evaluated based on the COSMIN methodology in this study.
Evaluation of each measurement properties of the included PROMs
Each measurement’s properties of the included 9 PROMs were evaluated using the initial 2 steps of 3 substeps for performing a systematic review of COSMIN methodology [18,20].
First, the methodological quality of each study on measurement properties was evaluated using the COSMIN Risk of Bias checklist [17,20]. This checklist was developed to systematically evaluate tools that determine the PROM’s content validity, structural validity, internal consistency, cross-cultural validity/measurement invariance, reliability, measurement error, criterion validity, hypothesis testing for construct validity, and responsiveness. Content validity is a crucial measurement attribute that determines how well the PROM’s content reflects the measurement concept including relevance, comprehensiveness, and comprehensibility [17]. The internal structure refers to how the different items in the PROM are related, this step concerns an evaluation of structural validity, internal consistency, cross-cultural validity, and other forms of measurement invariance [20]. Structural validity is defined as the degree to which the scores of a measurement instrument adequately reflect the dimensionality of the construct being measured, and it can be assessed using factor analysis and item response theory (IRT)/Rasch analysis [21]. Subsequently, the remaining measurement properties (reliability, measurement error, criterion validity, hypotheses testing for construct validity, and responsiveness) were evaluated. Unlike content validity and internal structure, the evaluation of these measurement properties provides information on the quality of the scale or subscale as a whole, rather than on the item level [22]. The methodological quality of each measurement was rated as very good, adequate, doubtful, or inadequate using items in the checklist with the worst score counts principle, in which the lowest rating of any standard was taken as the methodological quality [20].
Second, the result of every single study on a measurement property was rated against the updated criteria for good measurement properties: sufficient (+), insufficient (-), or indeterminate (?) [22]. For the assessment of structural validity, the updated criteria required results related to confirmatory factor analysis (CFA) or IRT. In this study, the results from exploratory factor analysis (EFA) were evaluated by the following criteria: sufficient (+) if the identified factors explained at least 50% of the variance, indeterminate (?) if the explained variance was not reported, and insufficient (-) if the factors explained less than 50% of the variance [21]. Cronbach α was used to evaluate the property of internal consistency: sufficient (+) if the Cronbach α≥0.70 for each unidimensional scale or subscale, indeterminate (?) if the evidence was not reported, and insufficient (-) if the Cronbach α<0.70 [22]. For the assessment of reliability, the updated criteria required intraclass correlation coefficient or weighted kappa. However, in this study, reliability was assessed based on results of Pearson’s coefficient: sufficient (+) if Pearson’s r≥0.80, indeterminant (?) if Pearson’s r was not reported, and insufficient (-) if Pearson’s r<0.80 [21]. Criterion validity was also assessed using correlation with a gold standard; sufficient (+) ≥0.70, indeterminant (?) if no information was reported, and insufficient (-) <0.70 [22]. To interpret the findings of the hypothesis test, a formulation of a set of hypotheses for the expected relationship is suggested to evaluate validity and responsiveness. For the convergent validity, at least 0.50 between the PROM and the comparator instrument that intends to measure the same construct was interpreted as sufficient in this study [20]. Unlike convergence validity, the discriminant validity hypothesizes that a weak correlation between the PROM and the comparative measurement tool that measures different properties was interpreted as sufficient [23]. The known group validity test hypothesizes that there will be differences in the concept of interest scores according to the group, and empirically judged by the research team [24].
RESULTS
General characteristics of the included PROMs and studies
Table 1 presents the characteristics of 40 studies in which 13 PROMs were used to detect PTSD. The number of participants included in the studies ranged from 14 to 702 (mean age range: 25.9 [standard deviation, SD=±3.0] to 52.8 [SD= ±15.9] years) and 17 studies reported the PTSD prevalence ranged from 14.0% [25] to 71.0% [26]. The range of CPTSD prevalence was 11.3% [27] to 40.7% [9], while another study reported a lifetime prevalence of 15.3% [11]. Twenty-four studies were conducted with participants living in the community [9,11,28-44,46-48,61,62], 8 studies at Hanawon (The Settlement Support Center for North Korean defectors) [26,27,50-55], 6 studies at medical centers [25,45,48,56-59], and 2 studies were conducted using an online survey [49,60]. Out of 40 studies reviewed, only one study reported the longitudinal trajectories of the mental health of North Korean defectors [48].
However, only 9 PROMs were validated for South or North Koreans before they had used for the study: Impact of Event Scale-Revised-Korean (IES-R-K) [63,64], Impact of Event Scale-Revised-North Korean Refugees (IES-R-NKR) [65], Minnesota Multiphasic Personality Inventory-PTSD-Korean (MMPI-PTSD-K) [66], PTSD Checklist Civilian-North Korean Refugees (PCL-C-NKR) [67], PTSD Checklist-5-Korean (PCL-5-K) [68], Trauma Scale for North Korean Refugees [69], Posttraumatic stress Diagnosis Scale-Korean (PDS-K) [70], and Post-Traumatic Stress Symptom Scale for North Korean Refugees [71]. To evaluate the properties of each measurement, we excluded 4 tools that had only been translated into Korean without any validation. For example, PDS was excluded but PDS-K was included because PDS-K was validated in South Koreans. And two versions of IES-R-K and IES-R-NKR, which were translated and tested by different researchers, were included and evaluated separately (Table 2).
Characteristics of PTSD measurement tools
We found nine validated PROMs that had been used in the studies on North Korean defectors (Table 2). IES-R, MMPI-PTSD, PCL-C, PCL-5, and PDS were originally developed in foreign countries, and have been validated as South or North Korean version.
IES-R is the revised version of the IES scale (7 intrusion items and 8 avoidance items) developed by Horowitz et al. [72], comprising 22 items [73]. In IES-R, intrusion symptoms (8), avoidance symptoms (8), and hyper-arousal symptoms (6) were evaluated on a 5-point scale (0-4). MMPI-PTSD is a scale created by extracting items characteristically appearing in PTSD patients among MMPI items [74]. Subscale is divided into seven categories: emotional problems (12), memory problems (10), interpersonal problems (7), unrealistic experiences and thinking (3), impulse control problems and physical discomfort (3), concentration disorders (5), and destructive impulses (4) [66]. The PTSD Checklist (PCL) is based on the PTSD diagnostic criteria of DSM-IV. It consists of 17 items to assess re-experience (5), avoidance symptoms (7), and hyperarousal symptoms (5) on the Likert scale from 1 point (not at all) to 5 points (very much) [67,75]. There exist several versions that can be used for the general public (civilian versions, PCL-C), special occupations (specific versions, PCL-S), and military officials (military versions, PCL-M) [76]. The PCL-5 has been changed in accordance with the revised standards of DSM-V, and “negative interaction recognition and mood” has been added to “intrusion,” “avoidance,” and “alterations in addition and reactivity.” [77] PDS [78] is a tool that can diagnose post-traumatic stress and evaluate the severity of symptoms, including 17 items of re-experience (5), avoidance (7), and hypersensitivity (5), which were evaluated on the Likert scale from 0 to 3.
The Trauma Scale for North Korean Refugees [69] and the Post-Traumatic Stress Symptom Scale for North Korean Refugees [71] are PROMs that have been particularly developed and validated for North Korean defectors. Understanding both the traumatic experiences and their related symptoms will be helpful in selecting a treatment approach because the traumatic events experienced by North Korean defectors during their escape journey are quite different from those experienced by the general population. These two PROMs include a trauma experience checklist specialized to North Korean defectors such as imprisonment, torture, threats to personal security, etc. The Trauma Scale for North Korean Refugees [69] was developed for North Korean defectors in accordance with the DSM-IV diagnostic criteria, and a total of 16 items were answered on a Likert scale of 1 point to 4 points to measure PTSD symptoms. The Post-Traumatic Stress Symptom Scale-North Korean Refugees was developed to incorporate components of complex PTSD based on the DSM-IV criteria [71].
Methodological quality
The methodological quality of each study is presented in Table 3. Internal consistency was evaluated in all the studies. No study assessed responsiveness, which is a criterion for detecting changes in the constituent concept over time. No study demonstrates evidence for cross-cultural validity and measurement error.
Content validity
The relevance of the components of the content validity study and trauma was confirmed in all studies. Comprehensiveness was evaluated based on the diagnostic criteria of the DSM to measure PTSD symptoms with all the included studies reporting its values. Tools that examined the validity of the original tools in Korean studies or those involving North Korean defectors did not report comprehensiveness values. Comprehensibility was reported for four tools (IES-R-K [63], IES-R-NKR [65], Trauma Scale for North Korean Refugees [69], and Post-Traumatic Stress Symptom Scale-North Korean Refugees [71]); however, this was difficult to evaluate considering the lack of information regarding the number of individuals surveyed (whether less than 30) and whether interviews were conducted. In addition, it was described that experts participated in the tool translation process; however, there was no mention of content validity index or content validity ratio. The studies that asked participants for comprehensibility and modified the questions were given a sufficient (+) rating (Table 4).
Structural validity
In this study, there were 4 studies confirming the number of factors using principal component analysis (PCA) and the total variance was 46.9% [63], 68.8% [64], 34.9% [66], and 66.9% [68], respectively (Table 3).
One study conducted CFA, but the model fit was not reported. In the IES-R-K, the sample size was considered insufficient because the number of participants (sample size, n=105) was five times lesser than the total number of questions (22 questions×5). Model suitability for factor analysis was not described in all studies.
Internal consistency
Internal consistency indicates to what extent the subscale measures the latent variable, and Cronbach α was generally used. When the measurement tools are multidimensional, it is recommended to present Cronbach α for the subscale rather than Cronbach α for the total scale. There were a total of 4 studies that presented all the values of the subscale [63,67,70,71], and only the total value was presented in 5 studies [64-66,68,69]. All internal consistency met the criteria at Cronbach α>0.70.
Reliability
Reliability was assessed in six of the studies, by administering the same instruments to the same respondents at different times (i.e., the test-retest reliability) [63-66,68,70]. If the period was appropriate from 1 to 4 weeks and the Pearson correlation coefficient was ≥0.70, then the evidence was found to be sufficient. The studies that did not perform test-retest in this study were two studies conducted at Hanawon (an initial settlement education institution, after entering South Korea) or conmmunity [69,71] and one study conducted at a medical clinic [67].
Criterion validity
Criterion validity is defined as the degree to which the scores of a measurement instrument adequately reflect a standard [21], and using the Clinician-Administered PTSD Scale (CAPS) and Structured Clinical Interview for the DSM (SCID) as the “gold standard” measure of PTSD symptomatology [79,80]. In five studies, concurrent validity was measured and three studies showed that the correlation analysis result with the gold standard was r≥0.70. The correlation coefficient between PCL-C-NKR and CAPS was lower (r=0.47) than Beck Depression Inventory (BDI), a convergent validity measurement tool (Table 3). In addition, MMPI-PTSD and IES-R-K were used as standardization tools for the criterion for IES-R-K/PCL-C-MKR and PCL-5-K/PDS-K, respectively.
Hypothesis testing construct validity
Hypothesis tests include convergent validity, discriminant validity, and Known-groups validity [21]. In this study, depression inventory and anxiety inventory were frequently used to test convergent validity. The correlation between PTSD PROMs and depression scales [63-65,67,69,70] and anxiety scales [63,67,69,70] was found to be 0.30 to 0.83. The correlation between Brief Psychological State Inventory (BPSI), Minnesota Multiphasic Personality Inventory (MMPI) and Combat Exposure Scale-Korean (CES-K) was found to be 55, 0.38 and 0.48 [65,68,71].
The discriminant validity was tested using the State-Trait Anxiety Inventory (STAI) [64], Alcohol Use Disorders Identification Test and BPSI-Alcohol [65], and MMPI [71]. There was a low correlation of 0.06 to 0.67 (Table 3).
The Known-groups validity hypothesizes that there will be a difference in the conceptual score of interest in the group of two or more study subjects. In this study, there were four papers including PTSD/non PTSD [67-70], or PTSD/psychometric/normal groups [64,66,70] and the symptom scores of the PTSD groups were significantly higher than the non-PTSD or normal group.
DISCUSSION
In this scoping review, we evaluated the psychological measurement properties of the PROMs used to measure PTSD in North Korean defectors. This scoping review found that 9 PTSD measurements are currently available. The psychometric properties of 9 PROMs validated in Korea were evaluated using the COSMIN checklist.
According to our results, the theoretical basis was judged to be secure in terms of content validity, as all tools were linked to the DSM and developed to target those who experienced trauma (including survivors from earthquakes, workers in emergencies, veterans from the Vietnam War, and North Korean defectors). The concept of the PTSD measurement tools identified in this study had been determined according to the diagnostic criteria of the DSM-IV or DSM-V in their original versions, and most of the tools were translated later. However, DSM-V was revised in 2013 and included the number of key symptoms of the Disorder of Extreme Stress Not Otherwise Specified (DESNOS) such as persistent erroneous blame of self or others, negative expectations about the future, persistent negative mood, and externalizing behaviors, considering CPTSD that was not available in DSM-IV [77]. This concept of CPTSD was defined by International Classification of Diseases 11th revision (ICD-11) in 2018, and classified into unique symptoms of emotional difficulty, negative self-concept, and relationship difficulties, including re-experience, avoidance, and the threat of PTSD.
North Korean defectors have experienced a combination of various types of trauma for a long time during their stay in North Korea, China, or a third country, and in the process of settling in South Korea [10,11]. North Korean defectors who experienced interpersonal trauma or life-threatening diseases were generally considered to have more severe forms of PTSD and were more likely to be classified into a dual diagnostic group of CPTSD and PTSD [9]. The type, duration, and symptoms of trauma experienced by North Korean defectors were found to be closer to CPTSD than simple PTSD [5,35,36,38,53,65]. Thus, when measuring the trauma experiences and symptoms of North Korean defectors, it is necessary to use a tool that can capture CPTSD attributes.
IES-R, PCL-C, PCL-5, PDS, and MMPI-PTSD were developed in the United States, and IES-R was validated for South Koreans [63,64] and North Korean defectors living in South Korea [65]. IES-R-NKR [65] reflects the linguistic differences between South Korea and North Korea and revises them into terms that are easy for North Korean defectors to understand. PCL-C-NKR [67] was validated for North Korean defectors who visited the medical center; however, there was no mention of verbal modifications in the process. In particular, since the differences between cutoff scores in the previous studies should be checked, and the research was conducted on North Korean defectors suspected of suffering from PTSD, this tool should be cautiously administered to the general public in the community. The differences between cutoff scores in the previous studies should be checked.
Among the selected tools, Trauma Scale for North Korean Refugees and the Post-Traumatic Stress Symptom Scale for North Korean Refugees were developed to measure PTSD of North Korean defectors. For these tools, it is to be noted that cultural and linguistic differences between South and North Korea were considered in the development process. The Trauma Scale for North Korean Refugees was developed based on the SCID, but was used more as a checklist of trauma experience than a symptom scale [30,35,50,53,60]. The trauma Scale for North Korean Refugees is beneficial for various researchers because it was converted from interview tools to PROMs. However, among the symptoms of avoidance/numbing of DSM-IV, “Feelings of detachment or estrangement from others” is not included, creating a difference in direct comparison with the results of other measurement tools.
Post-Traumatic Stress Symptom Scale for North Korean Refugees is a tool developed to measure not only PTSD but also CPTSD [71]. Post-Traumatic Stress Symptom Scale for North Korean Refugees has been adapted from the Davidson Trauma Scale. Symptoms of CPTSD such as anger, personality change, chronic guilt and responsibility, emotional control difficulties, high drug dependence, violence, somatization, and distrust of others, which are the main characteristics of DESNOS were included. The Post-Traumatic Stress Symptom Scale for North Korean Refugees was also used more as a trauma experience checklist than as a symptom scale [10,28,60]. In addition, the trauma checklist included in the measurement tool allows a more detailed understanding of trauma experiences through three categories: North Korean residence, North Korean defector process, and South Korean society.
MMPI-PTSD consists of 49 questions empirically extracted from MMPI [74], however, only 45 of its questions have been validated in South Korea [66]. Although the MMPI-PTSD has been criticized for evaluating only general psychological pain rather than specific PTSD symptoms, it has the advantage of being able to detect faking and response bias. It can also extensively evaluates the general problems of PTSD [74]. However, studies have reported different results in terms of accuracy, indicating caution for its use [81].
In the case of a tool with a predetermined structure, it is not necessary to perform an EFA that determines the number of factors [82]. Especially for foreign-origin tools, it is recommended to perform a CFA because the constituent concepts and theories have already been secured during the validation stage in other languages [20,23,83]. Therefore, it would be more appropriate to implement CFA than PCA. In most studies, only the number of factors was confirmed through PCA, and CFA was rarely conducted on the hypothesized measurement model. In a study developing Post-Traumatic Stress Symptom Scale for North Korean Refugees, CFA was conducted, and each factor correlation was reported as 0.63-0.89. The sample size was 302, which can be considered sufficient, as the minimum sample size required in the measurement model proposed by COSMIN is 200 [20]. In addition to factor analysis, it is necessary to present an index of the suitability of the measurement model. However, indices indicating the fitness of the measurement model were not mentioned.
Reliability reflects the degree of relevance and consistency of the measurement scores and can be evaluated as interrater reliability, test-retest reliability, and intra-rater reliability. The test-retest reliability is to check the stability of the measurement tool and to evaluate whether the results obtained after repeated measurements on the same subject more than once under the same conditions are consistent [84]. Many studies report test-retest reliability, and in this study, it was overall evaluated well.
As for the criterion validity, CAPS and SCID were used and the correlation was found to be good. For convergent validity for hypothesis testing, depression and anxiety measurement tools such as BDI, CES-D, and STAI were used. PTSD is known to have a high correlation with depression and anxiety. Yet, Eun et al. [63], used an anxiety measurement tool as discriminative validity. In most studies, the convergent validity was confirmed, but the discriminative validity was not accurately specified.
No studies mentioned the measurement error and responsiveness, which refers to the systematic and random error of a patient’s score that is not attributed to true changes in the construct to be measured [21]. To assess the measurement error of an outcome measurement tool, repeated measurements in stable patients are required [85]. The measurement property of responsiveness refers to the ability of PROMs to detect change over time in the construct to be measured [22]. Particularly in intervention studies, it is important to select a responsive measurement tool to indicate reactivity to treatment [84]. It has been reported that the lack of evaluation of measurement error and responsiveness was common in several literature reviews, evaluating the measurement tool in accordance with the COSMIN standard [86,87].
In addition, we found that few studies used the tools based on DESNOS [31,50], which are translated and modified without validation in South Korean [9,27], to measure CPTSD among North Korean defectors. To explain more clearly the impact of CPTSD/PTSD on the physical, psychological, and social health of North Korean defectors, it is suggested to assess CPTSD as well as PTSD using a valid measurement tool. Recently, the International Trauma Questionnaire (ITQ) [88] was newly introduced to asses core features of both PTSD and CPTSD based on the revised ICD-11 [89]. The validity of ITQ has been reported for adults who suffered from adverse childhood experiences in South Korea [89]. Since the PTSD studies for North Korean defectors so far mainly have been dealing with PTSD, it seems necessary to validate ITQ for North Korean defectors.
The followings were the limitations of this study. First, we did not review the trauma event checklist, which is the first condition for PTSD diagnosis. The trauma experience of North Korean defectors is somewhat different from that of general South Koreans, veterans, or workers in emergent settings. To measure the trauma experience unique to North Korean defectors, it is needed to evaluate the trauma event checklist and select the appropriate one for further study. Second, since this study included studies that only focused on adults, measurement tools used for children were excluded. Exposure to violence, emotional/verbal abuse, sexual abuse, and bystander behavior in childhood is known to be related to CPTSD. And there are also North Korean defectors in their childhood at risk of CPTSD. Thus, valid measurement tools to detect and manage PTSD/CPTSD early are needed for this population.
Conclusions
This scoping review found that 9 PTSD measurements are currently available for North Korean defectors, and most of the PROMs have not been evaluated on their psychometric properties thoroughly. Because all tools were linked to the DSM and developed targeting those who experienced trauma, the theoretical basis was secure in terms of content validity. However, few studies involved North Korean defectors in the process of development or validation. And the most frequently tested characteristics in measurement properties for the internal structure were internal consistency, criterion validity, and convergent validity. No study reported sufficient structural validity as CFA results with a model fit. Thus, there is insufficient evidence to support the recommendation of a specific PROM for use among North Korean defectors with PTSD. Furthermore, it is suggested that the PROM which could capture core features of both PTSD and CPTSD based on the newly revised ICD-11 should be validated for North Korean defectors.
To effectively assess the PTSD of North Korean defectors, it is imperative to employ valid and reliable measurement tools that take into account their distinct trauma experiences, cultural backgrounds, and language proficiency. This will enhance our understanding of their mental health needs and facilitate more efficient intervention and support.