INTRODUCTION
Obesity is a serious health problem at present [1,2], and antipsychotic use-related weight gain and obesity are major concerns. Although the exact cause of antipsychotic-induced weight gain (AIWG) remains unclear, antagonism of histamine H1-receptors and serotonin 5HT2A/2C-receptors are known neurotransmitter causes of AIWG [3-5]; antipsychotic-induced disruption of leptin signaling and neuropeptide (orexigenic or anorexigenic) expression of hypothalamic nuclei are considered neuroendocrine causes of AIWG [6-9]. Regardless of the underlying mechanism of AIWG, weight gain occurs when energy intake exceeds the expenditure.
Olanzapine, one of the antipsychotic medications, has been found to increase calorie intake, causing weight gain, although there have been conflicting results regarding its effects on resting energy expenditure [10-12]. Other studies have shown that olanzapine induces a mean excessive energy intake of 28%, causing significant anthropometric changes in olanzapine-naive patients with schizophrenia and olanzapine-induced weight gain can be moderated by controlling food intake [13,14]. Therefore, the primary cause of AIWG may be related to increased food intake rather than reduced resting energy expenditure.
Phentermine is an effective and affordable anti-obesity drug with potent appetite suppression effects through the release of neurotransmitters, including norepinephrine, dopamine, and serotonin [15-18]. Like its prototype drug amphetamine [19], which can cause serious cardiovascular and psychotic complications [20], the concerns that phentermine could worsen the clinical symptoms of patients with psychiatric conditions restricts the application of phentermine in patients with obesity taking antipsychotic medications. Sletten et al. [21] conducted a double-blind crossover study in 1967 to compare the effects of chlorphentermine and phenmetrazine in patients with obesity taking antipsychotic medications; both drugs failed to prove their weight-loss effects in patients with obesity taking antipsychotic medications, and the reason was not well described. Since then, there have been no studies on phentermine monotherapy in patients with obesity taking antipsychotic medications. Thus, we performed a study to observe the phentermine use in patients with obesity taking antipsychotic medications and to explore clinical factors related to the weight-loss effect of phentermine.
METHODS
Data
This retrospective study used clinical data from the Nutrition and Weight Management Center at Boston Medical Center between July 2014 and August 2022. Patient’s chart was retrospectively reviewed multiple times to reduce errors in the clinical data extraction. This analysis was approved by the Institutional Review Board at Boston University Medical Center (H-26417).
Participants
Figure 1 shows the participants selection process. The inclusion criteria of original data were: 1) age 18-75 years; 2) body mass index (BMI) ≥30 kg/m2 or BMI ≥27 kg/m2 with weight-related comorbidities such as hypertension, diabetes/prediabetes, hyperlipidemia, or metabolic syndrome; 3) history of phentermine treatment; 4) and history of any antipsychotic exposure regardless of psychiatric diagnoses. Any antipsychotic medications classified into code N05A of the Anatomical Therapeutic Chemical classification were included in this study [22]. Through chart review, we acquired the diagnostic information made by internal medicine and psychiatric department specialists, respectively. For the psychiatric diagnosis, the Diagnostic and Statistical Manual of Mental Disorders, 5th edition criteria was applied [23]. The exclusion criteria for original data were: 1) patients with unclear antipsychotic exposure history; 2) patients with unclear phentermine exposure history; 3) patients whose phentermine intervention preceded antipsychotic exposure; 4) patients who did not use antipsychotic during phentermine treatment; and 5) other causes such as prescription error, combined use with other anti-obesity drugs, and refusal to use phentermine. The final cohort (n=57) was obtained using secondary exclusion criteria, which were: 1) patients who missed the initial or follow-up measurements and 2) patients with short-term (<3 months) phentermine use. Based on the percentage of body weight (BW) reduction (BWR%), the final cohort was classified into responder (n=25; BWR% ≥5%) and non-responder (n=32; BWR% <5%) groups.
Intervention and safety monitoring
The phentermine drugs explored in this study included generic phentermine 8, 15, 30, and 37.5 mg tablets, Lomaira 8 mg tablets, Adipex-P 37.5 mg capsule, and Qsymia (phentermine and topiramate combination). All phentermine drugs were administered orally every morning. To monitor adverse events (AEs) and tolerability, half the daily dose was prescribed for the first two weeks which was gradually increased under close monitoring. Most phentermine drugs are indicated for temporary use (<3 months), except for Qsymia, which was approved as a long-term prescription. For this study, we selected 3-6 months as the exposure duration because phentermine is frequently used off-label for >3 months with topiramate in the clinical setting [24]. Considering the participants’ vulnerability to psychiatric AEs, they were provided detailed information about the possible AEs of phentermine use and were strictly monitored.
Measures
The study initiation point was determined as the first ever exposure to phentermine mentioned in the medical chart. Age, sex, medical and psychiatric diagnoses, psychiatric medication information, and initial anthropometric variables, such as BW, BMI, systolic blood pressure, diastolic blood pressure, and pulse rate, were extracted. To compare the dosages of different antipsychotic medications used by each patient, they were converted into chlorpromazine-equivalent doses [25]. The follow-up point was 6 months after the study initiation date, and the final anthropometric variables were collected. If there were no follow-up visits after 6 months, the available data from the closest follow-up visits within 2 months were substituted. AEs were reviewed and recorded at every visit during the 6-month study period.
Statistical analysis
Continuous variables are described by their means (standard deviations), and categorical variables are described by their frequency and percentages. To compare the differences between responders and non-responders, the chi-square or Fisher’s exact test was used for qualitative variables, whereas the independent t-test was used for quantitative variables with normal distribution patterns. A paired t-test was used to determine the effectiveness of phentermine before and after intervention. A logistic regression analysis was performed to adjust the effects of confounding variables which might influence the weight-reduction effect of phentermine. Statistical significance was determined by a p-value of <0.05. All statistical analyses were performed using Predictive Analytics Software (PASW version 27.0; SPSS Inc., Chicago, IL, USA).
RESULTS
Baseline demographic and clinical features
The demographic and basic clinical variables of the final cohort, responders, and non-responders are listed in Table 1. In the final cohort, the mean age of the participants was 45.1 (13.1) years, and 78.9% were female. Hypertension (42.1%) and bipolar disorder (38.6%) were the most common medical and psychiatric diagnoses encountered, respectively. The mean phentermine dose used was 29.4 (10.5) mg, and the mean duration of phentermine exposure was 5.3 (1.0) months. There were no significant differences in age, sex, and medical and psychiatric diagnoses between the responders and non-responders.
Comparison of anthropometric variables before and after phentermine use
Figure 2 shows the results of the paired t-test performed on the variables of the final cohort, responders, and non-responders. The final cohort had a mean BWR and BMI reduction (BMIR) of 4.45 (7.04) kg (p<0.001) and 1.64 (2.61) kg/m2 (p<0.001), respectively. The responders showed a mean BWR and BMIR of 10.13 (4.43) kg (p<0.001) and 3.67 (1.92) kg/m2 (p<0.001), respectively. The non-responders showed no significant BW or BMI changes between the initial and 6-month follow-up parameters.
Comparison of anthropometric changes before and after phentermine use between responders and non-responders
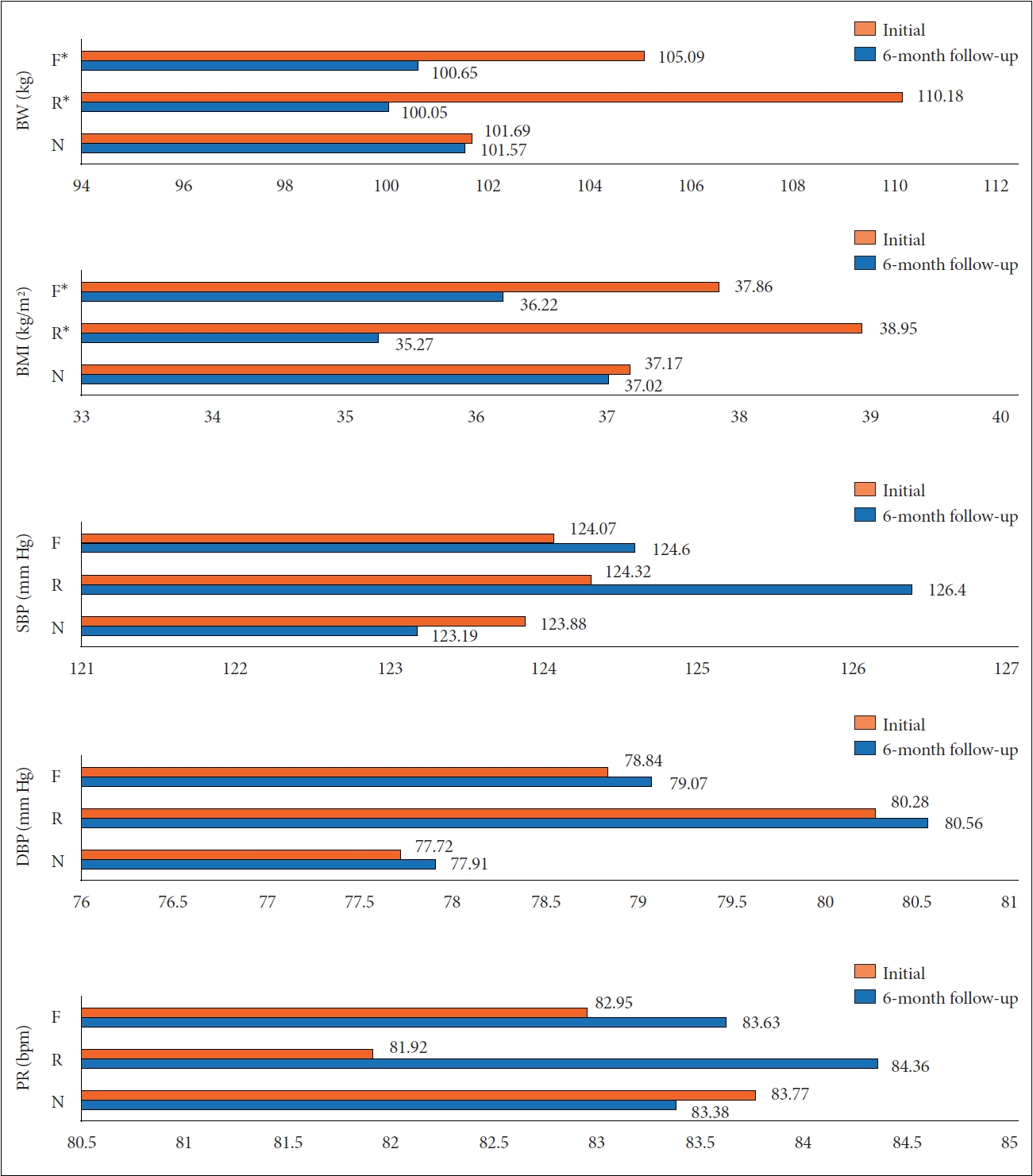
Figure 3 presents the anthropometric variables of the final cohort before and after phentermine use, and the statistical comparisons between the responder and non-responder values. In the final cohort, the mean BWR% and the mean BMIR percent (BMIR%) were 3.92% (6.69%) and 4.04% (7.02%), respectively. In the responders, the mean BWR% and BMIR% were 9.35% (4.09%) and 9.41% (4.92%), respectively, which was significantly different from that of the non-responders with a mean BWR% and BMIR% of -0.31% (5.68%) and -0.15% (5.39%), respectively. There were no significant differences in the other anthropometric variables between responders and non-responders.
Comparison of clinical variables associated with the phentermine response
Table 2 presents a statistical comparison of the clinical variables between the responders and non-responders. There were significant differences in the rates of the anticonvulsant combination therapy (ACT; responder, 72.0% vs. non-responder, 43.8%; p=0.033) and total duration of antipsychotic exposure (responder, 23.9 [16.9] months vs. non-responder, 37.2 [27.6] months; p=0.039). To adjust for confounders such as age, sex, and baseline BW and assess the contribution of ACT and the total duration of antipsychotic exposure to the weight-loss effect of phentermine, a logistic regression analysis was performed (Table 3). The odds ratio of ACT for the phentermine response was 3.840 (95% confidence interval [CI]: 1.082-13.630; p=0.037). The total duration of antipsychotic exposure (odds ratio=0.726; 95% CI: 0.497-1.060; p=0.097) was not independently associated with the phentermine response. This model (χ2=12.80; difference=6; p=0.046) was correctly classified with the 63.2% of participants, and its Nagelkerke R2 was 0.270.
Safety of phentermine
In the final study cohort (n=57), 13 subjects reported 17 tolerable AEs such as sleep disturbance (n=4, 7.02%), dry mouth (n=2, 3.51%), dizziness (n=2, 3.51%), and constipation (n=2, 3.51%). In the short-term phentermine users (n=29) who were excluded from the primary cohort (n=110), 13 subjects reported 15 AEs, which led them to discontinue the phentermine treatment. These intolerable AEs included irritability/mood change (n=3, 10.34%), anxiety (n=3, 10.34%), headache (n=2, 6.90%), and palpitation (n=2, 6.90%) (Table 4). Two subjects required hospital admission or an emergency room visit due to severe mood change or headache accompanied by palpitation.
DISCUSSION
To the best of our knowledge, this is the first study to observe the use of phentermine for patients with obesity with psychotic or non-psychotic psychiatric conditions. Among the 57 participants in the final cohort, 25 participants had ≥5% of mean BWR over 6 months and were classified as the phentermine responder group. The non-responder group had a longer total duration of antipsychotic exposure and lower rates of ACT. After modifying the confounding variables, ACT presented significant association with the phentermine response. The final cohort experienced 17 tolerable AEs.
In the final cohort, the mean BWR in 6 months was 4.45 (7.04) kg, with a response rate of approximately 44%, which is considerably lower than the reported mean BWR in a general population of 7.5-9.2 kg with approximately 70% response rate [15,16], indicating the limited efficacy of phentermine in patients with obesity taking antipsychotic medications. One of the hypotheses for this phenomenon is the counteraction between phentermine and antipsychotic medications, which has been reported by several preclinical studies [26,27]. Although phentermine releases neurotransmitters in the hypothalamus and limbic area [17,18], where the antipsychotic medications exert antagonistic effects on neurotransmitter receptors, especially on the dopamine D2 receptors [28,29], phentermine mainly releases norepinephrine [30,31]. There is little evidence of a counteraction between phentermine and antipsychotic medications.
Another possible explanation for the decreased BWR in patients with obesity taking antipsychotic medications on phentermine compared to the general population could be the orexigenic effects of antipsychotic medications or the nature of the serious psychiatric conditions. Anti-psychotic medications cause increased food intake through diverse mechanisms [3-9,12-14]. Patients with psychiatric conditions also tend to have a less balanced diet and more sedentary lifestyle [32]. Antiobesity drugs other than phentermine might show reduced efficacy in patients with obesity taking antipsychotic medications compared with the general population. However, few studies have directly compared the effects of anti-obesity drugs in the general population and patients with specific illnesses or medications. Further investigation would help us better understand the obesity pathophysiology and the mechanism of anti-obesity drugs.
The non-responders had a significantly longer total duration of antipsychotic exposure, even though the association between phentermine response and the total duration of antipsychotic exposure was mitigated on the logistic regression model. A systemic review reported that AIWG occurs 3-4 fold in patients with limited antipsychotic exposure regardless of type in both short- and long-term trials [33]. Our results suggest that the mechanism of AIWG could differ between individuals who recently started antipsychotic medications and those who took antipsychotic medications chronically, and further study would be necessary in this regard.
Although antipsychotic medications seemed to limit the effect of phentermine, the phentermine responders in this study achieved a mean BWR of 10% between the initial and endpoint measurements. Specifically, responders had higher rates of ACT (predominantly topiramate: a gamma-aminobutyric acid agonistic and glutamate-antagonistic anticonvulsant with weight-loss effects) [34], and the association between ACT and phentermine response was maintained after the modification of confounding factors. Appropriate combination therapy could be an excellent strategy for overcoming the reduced effectiveness of phentermine in patients with obesity taking antipsychotic medications. The combined medication of phentermine and topiramate is already considered effective for weight management in the general population [35]. Although phentermine and topiramate could worsen psychotic or manic symptoms [36-38], combination therapy has improved tolerability compared to monotherapy [39].
There were 13 out of 57 final cohort patients who reported AEs, including dry mouth, sleep disturbance, dizziness, and constipation, which is expected with the known AEs of phentermine include paresthesia, dry mouth, dysgeusia, constipation, anxiety, irritability, sleep disturbance, palpitation, and arrhythmia or ischemic heart disease [40,41]. However, these results might have been caused by a selection bias in the screening process. When the primary cohort (n=110) underwent secondary screening (Figure 1), 51 subjects were excluded because of missing baseline/follow-up evaluation (n=24) or because of short-term phentermine use (n=29). Among these 29 shortterm users, 13 subjects discontinued phentermine due to intolerable AEs, such as irritability/mood change, anxiety, headache, and palpitation; some required hospital admission or an emergency room visit. Although the retrospective nature hindered our study from providing exact numbers, there was a 27% discontinuation rate and a 1.8% serious AE rate based on the primary cohort (n=110). These numbers are similar to the results of previous phentermine and topiramate combination trials that reported an 18% discontinuation rate with high doses and a 2.2%-3.6% serious AE rate [42-44]. Therefore, phentermine could be an effective pharmacological modality for patients with obesity taking antipsychotic medications with a thorough selection process and frequent monitoring for AEs.
This study has several limitations. This study was not adjusted for possible confounders including other medications causing weight change, previous exposure to different types of anti-obesity drugs, and additional weight-loss interventions. Patients in our medical system also may receive medical care from other institutions, which was not accounted for in this study. During the 6-month study period, subtle changes in the participants’ psychiatric symptoms and the interaction between the subjects and their psychologists/psychiatrists may have been omitted due to certain restrictions for reviewing psychiatric notes. This study also reported anthropometric changes only, and laboratory variables such as fasting blood glucose, HbA1c, and lipid profiles, were not included in this study. However, 5%-10% BWR could be sufficient to induce metabolic benefits, which would not be noted in this study [45]. The small sample size limited exploring the difference between the types of antipsychotic medications and the phentermine response. Finally, the retrospective design and the possibility of familywise errors due to multiple comparisons had limitations in generalizing our results. Further prospective studies with a larger sample size would be warranted.
In conclusion, this is the first study to observe the use of phentermine for patients with obesity with psychotic or non-psychotic psychiatric conditions. As in the general population, phentermine treatment is effective for patients with obesity taking antipsychotic medications, and ACT augmented the weight-loss effect of phentermine. The AEs encountered and tolerability were similar to those in the general population. Future directions should include prospective, multicenter studies with a larger sample size to determine efficacy and safety of phentermine in patients with obesity taking antipsychotic medications.