INTRODUCTION
Attention-deficit hyperactivity disorder (ADHD) is a neurodevelopmental disorder that becomes evident in preschool and school age and often persists into adulthood. It is reported that around 5% of school-age children all over the world have ADHD [1,2]. Three main symptoms are characteristic, such as inattention, impulsivity, and/or hyperactivity. It has been thought that genetic factors may be at the forefront besides environmental factors in the disease, which was defined as mini brain damage in the past years [2,3]. However, no single cause has been identified. In these patients, diagnosis and follow-up are based on observations of parents and teachers. In its pathophysiology, ADHD was thought to be caused by dysregulation of catecholaminergic system. In the studies, it was showed that there are defects in dopamine pathways effective in cortical and subcortical brain perfusion [4]. For this reason, drugs that are effective on dopaminergic pathways are frequently used in the treatment [5]. Methylphenidate (MPH)-like pharmacological agents that are effective in the treatment are drugs that have a vasoconstrictor effect on the vessel [6]. Therefore, they probably show their success in treatment by acting on the local or systemic blood circulation. Their effectiveness in ADHD patients may be related to the increased circulatory dynamics in these patients. Therefore, there seems to be an important relationship between the dynamic global circulation of the brain and the pathophysiology of ADHD patients. The well-blooded brain has a developed venous circulation system that collects this blood and returns it to the heart. The large-volume, low-pressure and low-velocity venous circulation of the brain plays a critical role in maintaining homeostasis in the central nervous system [7]. Although local brain perfusion studies have been performed, there is no study in the literature based on direct or indirect measurement of cerebral venous circulation in ADHD, and the effect of treatment on cerebral venous circulation. For this purpose, superior vena cava (SVC) flow seems to be a good biomarker as it is a noninvasive, easily measurable, reproducible method, and provides indirect information about cerebral venous circulation. Because SVC flow is a proxy of cerebral perfusion and cerebral blood flow [8]. Many studies have been conducted on SVC flow in neonates and children [8-10]. Especially in studies conducted in newborns and premature babies, a relationship was found between SVC flow and intraventricular haemorrhage, death, and neurological development [10,11]. Therefore, it was aimed to noninvasively measure SVC flow, which is an indirect indicator of cerebral venous flow, by transthoracic echocardiography in healthy children and patients with ADHD before and after MPH treatment.
METHODS
Study population
Two groups were formed in this single-centre study, 40 children with ADHD and 44 children without ADHD. The patient group consisted of children newly diagnosed with ADHD in the child and adolescent psychiatry outpatient clinic and in need of medical treatment (MPH). The healthy control group consisted of healthy school-age children who did or plan to do sports activity and applied to the pediatric clinic for health check-up for this purpose. Twenty-four children who do sports regularly (at least 4 hours a week) and 20 children who plan to start sports and did not do sports before were included in this group. The groups were matched for age, sex, and weight. Inclusion criteria were term delivery, normal mental status, no medication for any disease in the past 6 weeks, and no previous treatment for ADHD. Exclusion criteria of the patient and healthy group were the absence of any neurological, psychiatric (except for ADHD only in the patient group), cardiac and/or systemic chronic disease in the past or post-screening.
This study was approved by the Ethics Committee of Şişli Hamidiye Etfal Research and Training Hospital (Reference number: 3361/14.12.2021).
Psychiatric evaluation
Psychiatric evaluation of children was conducted with Schedule for Affective Disorders and Schizophrenia for School-Age Children Present and Lifetime Version, Diagnostic and Statistical Manual of Mental Disorders, 5th edition -Turkish Adaptation (K-SADS-PL-DSM-5-T). ADHD was evaluated with Turgay DSM-IV-Based Child and Adolescent Behavioral Disorders Screening and Rating Scale (T-DSM-IV-S). K-SADS-PL-DSM-5-T is a semi-structured interview using the early diagnosis of psychiatric disorders in children and adolescents based on DSM-5 criteria [12]. The reliability and validity of the Turkish version of this interview tool was demonstrated by Ünal et al. [13] Participant interviews were conducted by a child and adolescent psychiatrist certified and experienced in K-SADS-PL-DSM-5-T.
T-DSM-IV-S is a scale that evaluates ADHD and disruptive behavior disorders and is based on DSM-IV criteria [14,15]. In this study, the first 18 items of this 42-item scale related to ADHD symptoms (nine attention deficit and nine hyperactivity/impulsivity) were used. According to the questions asked, the parents rated the frequency of each symptom according to the 4-point Likert scale (0=none, 1=very little, 2=a lot, and 3=very much). According to this scaling, the family’s rating of “a lot” or “very much” for each item was considered positive. Children who were scored as “a lot” or “very much” on least 6 of the 9 items related to only inattentive on the scale were considered as “ADHD inattentive appearance.” Children who were scored as “a lot” or “very much” on least 6 of the 9 items related to only hyperactivity/impulsivity on the scale were considered as “ADHD hyperactivity/impulsivity appearance.” Children who were scored as “a lot” or “very much” on at least 6 of each of nine attention deficit and nine hyperactivity/impulsivity items on the scale were considered as “ADHD combined appearance.”
After psychiatric evaluation, children with diseases other than ADHD in the patient group, and children with ADHD and other psychiatric disorders in the healthy group were excluded from the study.
Cardiac evaluation
All children underwent transthoracic echocardiography and 12-channel electrocardiography (ECG). Transthoracic echocardiographic examinations were performed with Vivid S70N (General Electric Healthcare, Horten, Norway) echocardiography device using a 1.5-4.6 MHz transducer in the supine position, while the children were calm, and their eyes were open. All children’s SVC diameters and SVC flow velocity time integrals (VTI) were measured from a modified parasternal long-axis view and the subcostal view respectively, over an average of 8-10 cycles. Mean values of 8-10 measurements were taken to reduce respiratory variability. Simultaneously, ECG monitoring of all children was performed. To time flow events, ECG was recorded simultaneously with doppler flow rate. Heart rate was measured from the beats used to evaluate the VTI. SVC diameter was measured from the proximal segment of the SVC at the right atrium junction through the parasternal long axis window. The average of the maximum and minimum diameters was taken for the measurement. SVC flow was calculated separately for each ADHD patient (before and after treatment) and healthy child using the formula (VTI×heart rate×[SVC diameter]2×π/4×weight) [16]. In addition, SVC volume/beat was calculated formula (VTI×[SVC diameter]2×π/4×weight). In the formula, units (VTI in cm, SVC diameter in cm, π=3.14, and weight in kg) were applied. Those who were detected to have heart disease after the cardiac evaluation of all participants were excluded from the study.
Study design
At the first admission, all participants were evaluated with K-SADS-PL-DSM-5-T and T-DSM-IV-S. According to the results of all psychiatric evaluation, participants diagnosed with ADHD together with subgroups constituted the patient group. The healthy control group consisted of the participants who applied to the pediatric cardiology clinic for sport approval and who were not determined to have ADHD or other psychiatric disease findings in the psychiatric evaluation. Echocardiography and ECG examination were performed in all patients at the first admission. SVC flow of all participants were calculated. Children who were detected heart disease in the cardiological evaluation were excluded from the study. Patients in the ADHD group were started on osmotic-release oral system (OROS)-MPH as a single morning dose of 18 mg as recommended by the Food and Drug Administration [17]. The drug dose, which corresponds to an average of 0.6 mg/kg according to the weight of the patients, was not changed throughout the study period. Children who were started on treatment were called for control on the 15th day for treatment compliance and evaluation of SVC flow. Control transthoracic echocardiography and ECG were performed in about 6 hours after MPH treatment (in the 6-8 hours period when OROS-MPH concentration is highest [18]) to patient group, who used MPH treatment regularly, and who could come to the 15th day follow-up. In addition, corrected QT interval (QTc) of ADHD patients before and after treatment was calculated with Bazett’s formula.
If enough patients could be reached, it was planned to retrospectively compare the clinical responses of ADHD patients to treatment and the SVC flow values of the 1st and 15th days at the end of the 1st month. The clinical evaluation at the end of the 1st month was performed by psychiatrist blind to the SVC flow of the patients. Patients who did not use regular MPH therapy and could not attend their clinical follow-up were excluded from the 2nd and 3rd phases of the study.
Statistical analyses
Statistical analyses were performed using the IBM SPSS software (IBM SPSS Statistics for Windows, Version 21.0.; IBM Corp., Armonk, NY, USA). Visual (histograms) and analytical (Kolmogorov-Smirnov/Shapiro-Wilk’s test) methods were used to determine whether the variables were normally distributed. The chi-square test or Fisher’s exact test was used for categorical comparisons of nominal values in different groups. Student’s t-test or Mann-Whitney U test was used to compare the continuous variables between groups. Paired Student’s t-test was used to compare the measurements at two-time points for SVC flow and heart rate. The capacity of SVC flow values in predicting the presence of ADHD was analysed using receiver operating characteristic (ROC) curve analysis. A p<0.05 was considered statistically significant.
RESULTS
In the study, 40 (28 males, 12 females) newly diagnosed ADHD patients, and 44 (24 males, 20 females) healthy children were included. Forty ADHD patients consisted of 6 inattentive presentation, 2 hyperactive-impulsive presentation, and 32 combined presentation. Twenty-four of the healthy children consisted of those who exercised regularly for at least 4 hours a week in different sports branches. The other 20 children in this healthy group consisted of children who had not yet exercised regularly. The median ages of the children in the patient and healthy groups were 10 years and 11 years, respectively. As summarized in Table 1, there was no significant difference in age, weight, and sex distribution of the patients. There was no significant difference between the systolic and diastolic blood pressures in the patient and healthy groups. In the patient group, the mean QTc values in the ECG before and after the treatment were measured as 402±17 ms and 419±16 ms, respectively. This difference was statistically significant (p<0.001).
The mean T-DSM-IV-S inattention subscale scores of ADHD and healthy groups were 18.68±4.34 and 2.77±2.07 (p<0.001), respectively. The mean hyperactivity/impulsivity subscale scores of ADHD and healthy groups were 18.20±6.32 and 2.80±1.99 (p<0.001), respectively. The differences between the groups were significant (Table 1).
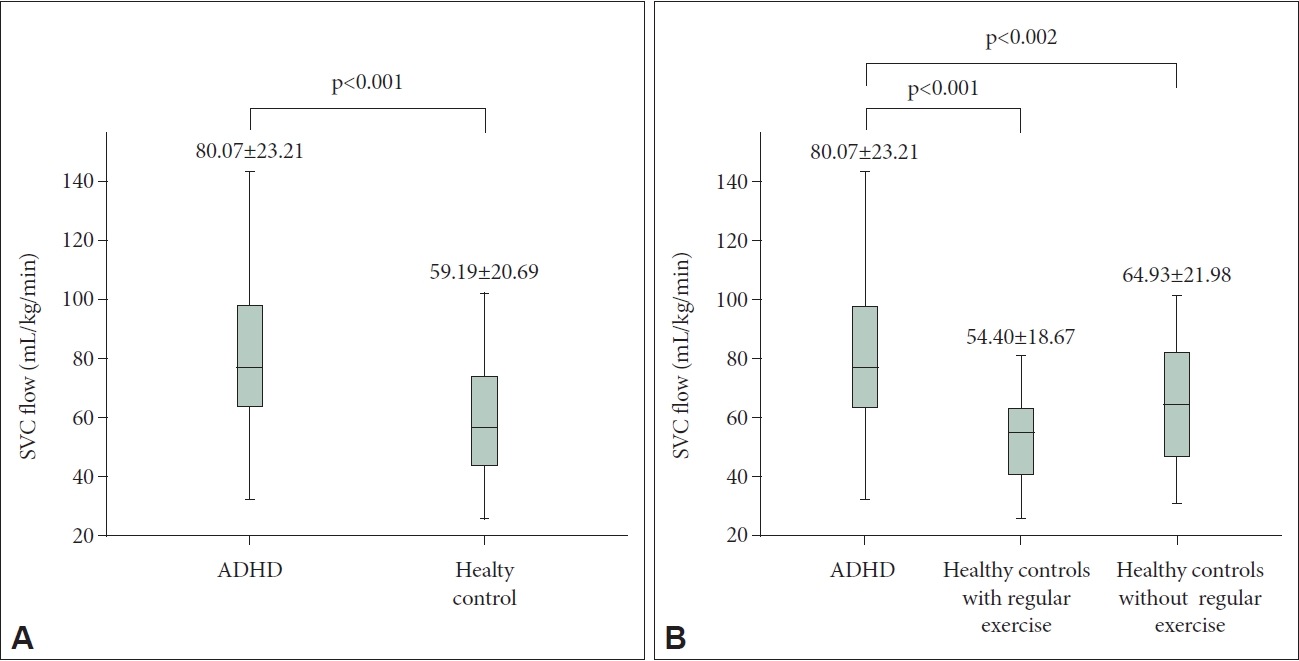
The heart rate of the children with ADHD was significantly higher than the healthy children (Table 1). SVC flow was measured as 80.07±23.21 and 59.19±20.69 mL/kg/min in patient and healthy children, respectively. SVC flow was significantly higher in patient than in all healthy children (p<0.001). The increase in SVC flow was not only related to heart rate. There was also a statistically significant increase in SVC volume/beat and SVC VTI compared to healthy children (Table 1). The SVC flow of healthy children with and without regular exercise were separately compared with the SVC flow of patient children (Figure 1). SVC flows of patient children were detected to be significantly higher than both groups, and this difference was higher in those who exercise regularly. In addition, a significant decrease was detected in SVC flow and heart rate (short-term measured from beat to beat) after 15 days of early treatment with low dose (mean 0.6 mg/kg) OROS-MPH in 26 patients who could come to the 15th day follow-up (Figure 2).
At the end of the 1st month, enough patients could not be reached. However, clinical response to treatment could be evaluated in 17 of 26 patients whose SVC flows could be measured on the 15th day after OROS-MPH treatment. According to the T-DSM-IV-S criteria, more than 50% improvement was determined in symptom severity in 15 patients who came to the controls and used regular MPH, while the improvement rate in symptom severity in 2 patients was determined around 23%-25%. SVC flow values of 17 patients before MPH and at day 15 after MPH were compared retrospectively. While the SVC flow values of 15 patients who responded above 50% to treatment decreased after MPH treatment (80.5±27.3 to 69.2±27.8 mL/kg/min), one of the 2 patients who had partial response to treatment remained almost unchanged (63.8 to 63.1 mL/kg/min), the other slightly increased (from 46.2 to 49.2 mL/kg/min) (Table 2.)
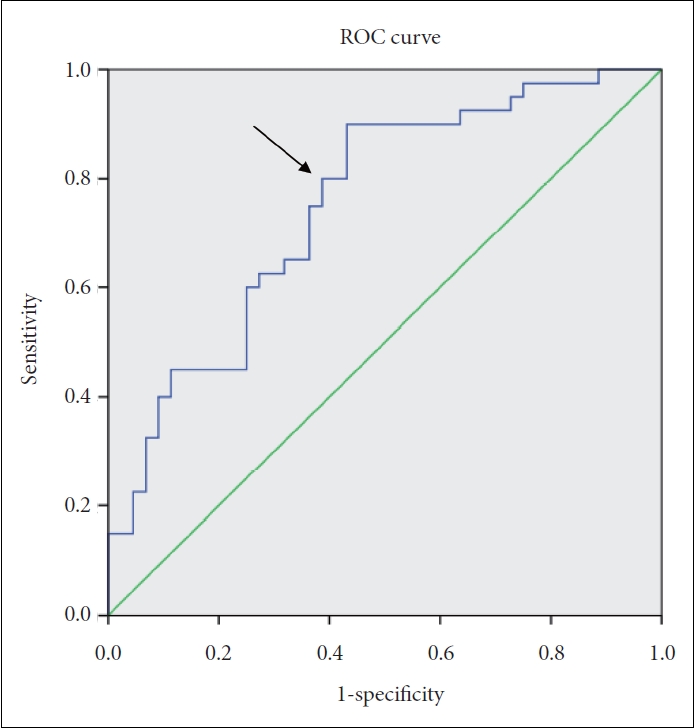
When the cutoff value of the SVC flow was taken as 61.4 mL/kg/min by ROC analysis for ADHD; sensitivity, specificity, and positive and negative predictive values were 80%, 61%, 65%, and 77%, respectively. The area under the ROC curve was 0.75 (95% confidence interval: 0.65-0.86) and was statistically significant (p<0.001) (Figure 3).
DISCUSSION
The mechanism underlying ADHD was not fully elucidated. Therefore, there is no useful biomarker or laboratory parameter for ADHD, whose diagnosis and follow-up is based on clinical observations [19]. In the historical process, many models such as delay in cortical maturation, deviation in maturation, and low cortical stimulation were emphasized [20]. Electroencephalogram (EEG) and magnetic resonance studies were used in supporting studies. However, the results obtained from these laboratory tools are contradictory [20-22].
The venous blood of the central nervous system, collected by the jugular and vertebral venous systems, empties into the right atrium through the SVC [23,24]. SVC flow reaches 35% of cardiac output, that is normal value of adult, at the age of 6 years [9]. Cerebral venous return constitutes approximately 50% of the SVC flow [9,25]. This rate increases as the age decreases, even up to 80% in premature patients [26]. SVC venous circulation is directly related to brain perfusion. For this reason, retrograde brain perfusion from the SVC is one of the techniques that is still being studied and with successful results in aortic arch surgeries [27]. In addition, it has been shown that brain ischemia and EEG changes occur in possible obstructions in the SVC flow [28].
Dopamine pathways are the most emphasized subject in ADHD physiopathology. In particular, the role of dopaminergic systems in working memory and inhibitory processes in ADHD is thought to be responsible for the basic mechanism [29]. Studies in ADHD patients was shown a relationship between dopamine pathways and brain perfusion [4]. In some studies, on brain perfusion, decreased perfusion status of some specific local regions such as frontal, thalamic and cerebellum was detected [4,30,31]. In some of these studies, in addition to this local perfusion increase, it was shown that there is a simultaneous increase in brain perfusion in patient with ADHD, especially in the superior parietal region including primary sensorimotor area, and in occipitoparietal junction [31].
In the study, it was found that SVC flow was higher in ADHD patients than in the healthy group. In addition, the significant decrease was detected in high SVC flow after drug treatment, which supported our findings in the study. There is no study in the literature on SVC flow or diffuse cerebral venous flow that we can compare in ADHD patients. However, in some studies, it was found a decrease in brain perfusion, especially in the prefrontal areas responsible for inhibition [4,30-33]. The inability of the frontal region to fulfil this inhibition task is thought to play a role in ADHD patients [32].
Possibly inadequate inhibitory control causes exaggerated motor activity and unsuppressed hyperactivity in somatosensory areas. As a result, increased brain metabolism and cardiac output increase cerebral venous return. Lee et al. [31] showed the increase in perfusion in somatosensory areas in ADHD patients in their study. There is a close relationship between cardiac output and SVC flow [9,26]. The heart is stimulated by the autonomic nervous system, dominated by the parasympathetic system [34]. There is a close relationship between the prefrontal cortex, conscious functions, and cardiac stimulation [35]. Reduced heart rate variability (HRV) has been shown to be associated with motivation to engage in social situations, social approach behaviors, self-regulation, and psychological flexibility in the face of stressors [34]. HRV studies in ADHD patients have shown an increase in mean heart rates with an increase in sympathetic tone [36,37]. In the study of Buchhorn et al. [37], a decrease in the mean heart rate of patients was observed after MPH treatment, similar to our study. Presumably, increased frontal inhibition control and parasympathetic tone after treatment, resulted in a reduction in heart rate and cardiac output. Although some studies have shown increases in heart rate due to late-term and high-dose MPH effects [38], the decrease in heart rate in our study may be due to early (15th day) and low-dose MPH treatment (on average 0.6 mg/kg/day). Some authors have shifted attention to low-dose MPH due to cognitive error as a result of possible adverse effects of high-dose MPH on D1, α1 and/or β1 receptors [39]. However, although the heart rate in the patient group decreased after 15 days of treatment, the heart rate after drug treatment was similar to the control group. In addition, time of taking the drug, time of day, patient posture, pediatric age group, and ADHD subtype (mostly combined type in this study), may have affected heart rates. In addition, heart rate was measured momentarily from the RR interval of the same beat in which the VTI was measured. Measurements based on long-term monitoring may differ.
At the molecular level, there are 5 subgroups of dopamine receptors in dopamine pathways, namely D1, D2, D3, D4, and D5 [40]. Among them, D1-D5 with stimulating effect and D2, D3, and D4 receptors with inhibitory effect show similarity in terms of structure and drug efficacy [40-42]. In addition, these receptors are also effective in brain perfusion through vasodilator mechanisms [40,41,43]. It is thought that dopamine transporter (DAT) and dopamine receptors play a role in the pathophysiology of ADHD [4,40,44]. MPH increases extracellular dopamine levels by blocking DAT [44]. In a study in healthy young rats, increasing extracellular dopamine levels with MPH resulted in hypoperfusion in large brain areas [43]. In addition, in the study of Schrantee et al. [45] in ADHD patients, the reduction of cerebral blood flow in global gray areas after MPH, supports our study.
In this study, SVC flow of children who exercise regularly were found to be lower than all groups. Similar effects of sports in healthy children and medical treatment in ADHD patients on reducing SVC flow suggest that sports therapy may be effective in ADHD patients. Studies have already shown that sports therapy as well as stimulant medications are effective on the core symptoms of ADHD patients [46].
This study presents some limitations. Participants in the ADHD group consisted mostly of the combination presentation. Therefore, the effect of subgroups on SVC flow could not be evaluated. In this study the effects of OROS-MPH on SVC after 15 days of treatment have been questioned. Studies are needed for the effects of MPH on SVC flow in long-term use. In addition, the relationship between SVC and clinical response to the drug at the end of the 1st month could be studied with a limited number of patients. In addition, multicentre, multi-participant, and double-blind studies are needed to fully demonstrate the relationship between SVC flow and ADHD.
In conclusion, this first study of SVC flow in children with ADHD showed that ADHD was associated with increased SVC flow, and MPH treatment had a reducing effect on this increased SVC flow. We believe that noninvasive, easily measurable, and reproducible SVC flow may be a new focus of interest for future comprehensive studies as a biomarker to support clinical evaluation in the diagnosis and treatment follow-up of ADHD patients.