Symptom Persistence after Iron Normalization in Women with Restless Legs Syndrome
Article information
Abstract
Objective
The aim of this study was to determine the clinical course of restless legs syndrome (RLS) and potential risk factors for the persistence of RLS symptoms after iron normalization in women with RLS and low serum ferritin (<50 μg/L).
Methods
We reviewed 39 women with RLS and iron deficiency, who achieved iron normalization after oral iron replacement for three months. Risk factors contributing to symptom persistence were estimated by logistic regression analyses. Remission was defined as no RLS symptoms for at least 6 months after the iron normalization.
Results
Over the observation period of 2.5±1.4 years, 15 patients reported no RLS symptom whereas 24 patients still complained of RLS symptoms. The remission rate of RLS with iron replacement was 38.5%. The relative risk of symptom persistence was increased by the duration of RLS symptoms (OR: 1.88, 95% CI: 1.01–3.49) or by the age at RLS diagnosis (OR: 1.25, 95% CI: 1.01–1.56).
Conclusion
Almost two-third of RLS patients with iron deficiency showed persistence of the symptom even after iron normalization. Considering that longer duration of RLS symptoms and older age at RLS diagnosis were risk factors for symptom persistence, early intervention of iron deficiency in RLS is warranted.
INTRODUCTION
Restless legs syndrome (RLS) is an urge to move the legs, usually accompanied by uncomfortable and unpleasant sensation in the legs. It is associated with disrupted sleep and lower quality of life [1]. The clinical course of RLS is known to fluctuate throughout a patient’s life. However, it has been recently reported that patients with greater RLS severity are more likely to have a chronic course [2]. RLS can be divided into primary or idiopathic and secondary forms. Well-documented secondary cause of RLS is an iron deficiency condition including end-stage renal disease, pregnancy, iron deficiency anemia and gastric surgery [3]. Although the pathogenesis of RLS is unknown, the abnormality of dopamine system is suggested as a mechanism for developing RLS and therapeutic effects of dopamine agonists have been clinically demonstrated. On the other hand, iron supplementation has been first recommended for RLS patients with low serum ferritin level (50 ng/mL or less) according to management guidelines [4,5].
Two randomized, placebo-controlled studies have documented that iron replacement treatment was beneficial for RLS patients with low serum ferritin level [6,7]. Wang et al. have compared the efficacy of oral iron therapy in eighteen participants, and found that symptom severity measured by the International RLS study group rating scale for severity (IRLS) [8] scores was decreased in the treatment group compared to that in the placebo group after 12 weeks of therapy [6]. The mean IRLS score change in the treatment group, was greater than that in the placebo group. The response rate defined as improvement of quality of life was reported to be 63.6%. Relatively small sample size and short follow-up period to estimate the efficacy of iron treatment remained as limitations of the study. Grote et al. [7] have performed a study with sixty RLS patients from multi-centers and prospectively followed-up the efficacy of intravenous (IV) iron sucrose compared to placebo until 12 months. The response rate which was defined as ≥50% reduction of IRLS scores at 11 weeks after iron treatment was 65%. Since oral iron is widely used in the treatment of iron deficiency, outcomes including efficacy and side effects of IV iron sucrose may be limited when generalized in real clinical settings. In our recent randomized controlled trial comparing oral iron therapy and pramipexole, we observed a modest response rate of 47% to iron replacement for fifteen RLS patients with low serum ferritin levels [9]. Since it was not a naturalistic study, little was known about the clinical course of RLS after correcting iron deficiency by oral iron treatment.
Although the response of iron treatment has been confirmed in RLS patients with low serum ferritin levels compared to placebo, not all RLS patients with low serum ferritin have shown sufficient response to iron treatment. The factors contributing to the persistence of RLS symptoms after the iron treatment are currently unknown. Up to date, the course and prognosis after iron treatment in patients of RLS with low serum ferritin levels have not been reported yet. Therefore, the objective of this current study was to extend the knowledge of the clinical course of RLS and potential risk factors associated with symptom persistence after iron replacement in RLS patients with low serum ferritin levels.
METHODS
Subjects
For retrospective analysis, female patients with RLS confirmed as iron deficiency at first visit were selected from the chart of the sleep clinic of Seoul National University Bundang Hospital (SNUBH) from January 2008 to December 2014. All patients were diagnosed as RLS by two sleep experts based on the essential criteria for RLS recommended by the National Institutes of Health (NIH) [10]. To exclude RLS mimics [11] such as myalgia, venous stasis, leg edema, arthritis, leg cramps, and positional discomfort, we used additional clinical examination and mimics-related questions. According to RLS treatment guidelines [4,5], the oral iron therapy was applied to the patients with serum ferritin concentration lower than 50 μg/L or iron saturation lower than 17% at their first visit. Patients were recommended to take oral iron supplement of iron sulfate 256 mg with ascorbic acid 30 mg twice a day for three months as the guidelines. If the patients complained of remaining symptom even after iron normalization, they were given additional medications such as dopamine agonists or α2δ ligand. Only subjects who achieved ferritin concentration ≥50 μg/L or iron saturation >20% and were observed for a period of at least 6 months after correcting serum ferritin were selected. Drop-outs with no follow-up data of serum ferritin or incomplete iron replacement, and individuals who had comorbidities including pregnancy, end-stage renal disease, malignancy, and other medical diseases causing iron deficiency were excluded from this study. The study protocol was approved by the Institutional Review Board of SNUBH (B-1606-350-102).
Baseline assessments
Baseline demographic and laboratory data at the initial diagnosis were extracted from electronic medical records of patients. All subjects were routinely evaluated for RLS severity using IRLS at the first visit. Participants were classified into the following four groups based on total IRLS scores for RLS severity; mild (1–10), moderate (11–20), severe (21–30), and very severe (31–40). In addition, we asked patients about several characteristics of RLS, including symmetry, presence of upper limb symptoms or pain, and family history. The other information of several questionnaires including the Pittsburgh sleep quality index (PSQI) for subjective sleep complaints [12], the Epworth sleepiness scale (ESS) for daytime sleepiness [13], and the Beck depression inventory (BDI) for depressive symptoms were also obtained. In addition, based on medical records or interviews, we determined whether patients had been taking medications such as antidepressants known to generate or exacerbate RLS symptoms.
Follow-up procedures and outcomes
Follow-up evaluation of RLS symptom at 6 months or more after achieving iron normalization had been conducted in June 2015 by face-to-face or telephone interviews as a part of RLS case management in the clinic, and this recording data was retrospectively obtained. The iron level was not measured at the follow-up evaluation, but in case of the recurrence of RLS symptoms during the follow-up period, the iron level test was done again to confirm whether the recurrence was related with iron deficiency. Sixteen patients were evaluated through face-to-face interview in the clinic and telephone interview was used for the rest of patients. We had asked the following question: “How are your RLS symptoms after iron normalization compared to those at the initial diagnosis?.” Responses included 0) absent or negligible without any medication for RLS after stopping iron supplements, 1) similar, fluctuating, or deteriorating, and 2) taking some medications to control RLS symptoms. If the response was “0,” the participant was assigned to the “remission” group. Those whose responses were “1” or “2” were assigned to the “persistence” group. The outcomes of this study were persistence of RLS symptoms and risk factors associated with RLS symptom persistence.
Statistical analysis
Between the remission and the persistence group, demographic characteristics, clinical characteristics, and laboratory data were compared using chi-square test or student t-test. Mann-Whitney test was performed when data were not normally distributed. We used multivariable logistic regression analyses to estimate the relative risk for persisting RLS symptoms as a dependent variable. Odds ratios (OR) and 95% confidence interval (CI) were determined after adjusting for the use of antidepressants, baseline serum ferritin level, family history and scores of BDI, PSQI and ESS as covariates. All tests of significance were two sided. p-value of less than 0.05 was considered as statistically significant. SPSS version 22.0 for Windows (IBM Corp., Armonk, NY, USA) was used in all analyses.
RESULTS
The study flow is shown in Figure 1. Among 61 patients who were diagnosed as RLS with iron deficiency, 8 patients droppedout in the process and 4 patients had underlying medical diseases (2 gastric cancer, 1 hypermenorrhea, 1 end stage renal disease). After excluding these 12 subjects, 49 patients of RLS were confirmed to have obtained normalization of serum iron and they stopped taking iron supplements. Among them, 10 patients (4 had no contact or refusal, 3 deceased, 1 rectal cancer, 2 gastric ulcer) were excluded. Finally, a total 39 RLS patients were included in our analyses. The mean age of the patients at the first visit was 53.8±13.5 (range, 14–76) years. Antidepressants were taken in 10 patients (paroxetine=2, venlafaxine=2, escitalopram=2, sertraline=1, mirtazapine=1, trazodone=1, nortriptyline=1) and 13 patients reported moderate to severe depressive symptoms according to BDI. Only two patients in the persistence group reported side effects including constipation and gastric discomfort. The demographics and RLS-related clinical characteristics at baseline were not significantly different between the drop-out subjects and the final participants.
Flow chart of RLS patients with iron deficiency. RLS: restless legs syndrome.
Over the observation period of 2.5±1.4 (range, 0.5–5.7) years after iron normalization, only 15 patients reported no RLS symptom while 24 patients had persistent RLS symptoms or had been taking medication for RLS. Therefore, the remission rate was 38.5%. Two patients in the remission group had reported the recurrence of RLS symptoms accompanied by low serum ferritin level at 3 and 6 months after the initial normalization. However, their symptoms were resolved with additional iron replacements which comprised the same dose and duration as in the initial treatment. Between the remission group and the persistence group, duration of RLS symptom was significantly different (4±3.3 years vs. 11.7±11.2 years, p=0.004). Age at RLS diagnosis also showed an increasing tendency in persistent group compared to remission group (48.7±14.8 years vs. 57±11.8 years, p=0.059). Although the mean score of IRLS rating scale was similar to each other between the two groups, the persistence group showed a trend toward more severe RLS (79.2%) than those in the response group (60%) when RLS severity was classified into mild to moderate and severe to very severe. Other demographic characteristics, serum ferritin level and RLS-related clinical features including antidepressant use were not significantly different between the two groups (Table 1).
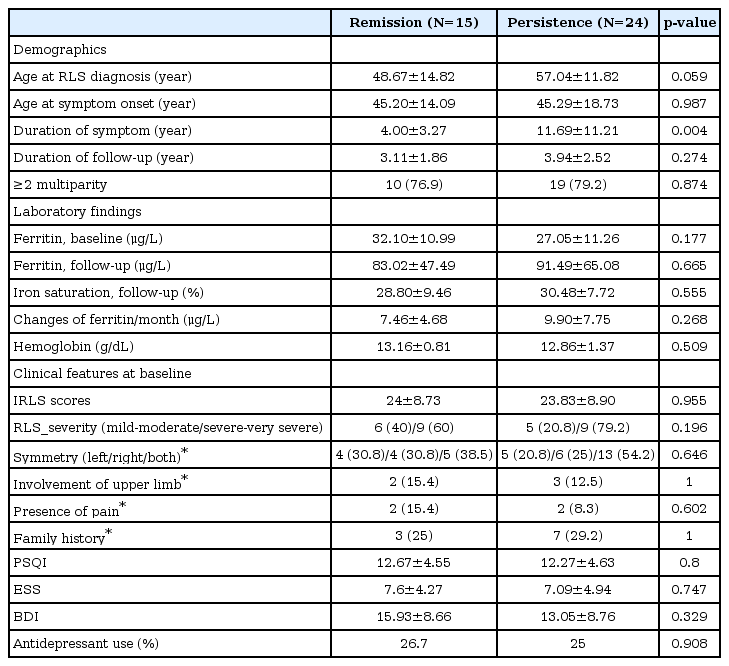
Comparison of baseline demographics and clinical characteristics between the remission group and the persistence group
Multivariable logistic regression analyses showed that RLS symptom duration at baseline and the age at RLS diagnosis were significantly associated with the persistence of RLS symptom after iron normalization (Table 2). There was no multicollinearity between symptom duration and age at diagnosis (Pearson’s coefficient of determinant=-0.075, p=0.639). Long duration of RLS symptom significantly increased the relative risk of symptom persistence (OR: 1.88, 95% CI: 1.01–3.49, p=0.048). In addition, the age at RLS diagnosis was significantly associated with symptom persistence. The relative risk of symptom persistence was higher when the age at diagnosis was older (OR: 1.25, 95% CI: 1.01–1.56, p=0.047). However, RLS severity was not significantly associated with the symptom persistence.
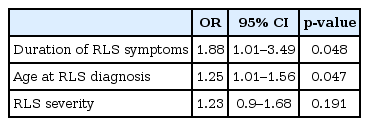
Logistic regression analyses for the persistence of RLS symptom
DISCUSSION
This study for the first time investigated the clinical course and persistence of RLS symptoms after iron replacement treatment in secondary RLS with low serum ferritin levels. The main findings were that almost two-third patients of RLS with iron deficiency showed the persistence of RLS symptoms even after iron normalization. In addition, longer duration of RLS symptom and older age at RLS diagnosis contributed to RLS symptom persistence.
The remission rate of iron treatment was found to be 38.5% in this study, which was slightly lower than 46.7% of our previous study after comparing the efficacy of treatments between oral iron and pramipexole in RLS patients with low serum ferritin [9]. The discrepancy might be due to different definitions used for treatment efficacy. In this study, we examined a relatively strict outcome of the remission state defined as no or negligible symptom. In our previous study, response state was defined as symptom reduction of 50% after oral iron treatment. Thus, the overall remission rate of oral iron treatment could be estimated to be around 40%. The remission rate of 38.5% in this study was unexpected because substantial RLS symptom control was supposed to be achieved after serum ferritin level became 50 μg/L or more. As secondary RLS with iron deficiency was defined as serum ferritin level of less than 50 μg/L or iron saturation of less than 17%, the improvement of RLS symptom would have been reasonably predicted with iron normalization of ≥50 μg/L. The reason for relatively low remission rate after iron normalization might be due to the fact that many cases of secondary RLS with iron deficiency had the pathophysiology of primary RLS at the same time. Among possible pathophysiology of primary RLS, brain iron deficiency and central dopamine dysfunction have been suggested. Serum ferritin level has been accepted as the best single measurement of iron store [14]. However, it is not an indicative marker of brain iron stores. Peripheral iron concentrations have no linear association with brain iron concentrations [7]. For this reason, regional brain iron deficiency still could have contributed to an abnormality of dopaminergic system that produces symptoms of RLS, even though the peripheral iron status has been normalized [15-18]. To control RLS symptoms, IV iron treatment is known to work better by maintaining higher levels of iron availability for short periods and by providing rich and fast iron supply to the brain. RLS symptoms might persist since oral iron supplement could not be effective enough to penetrate brain-blood barriers or replenish iron into brain regions as shown in the present study. The higher response rate (65%) with IV iron injections in previous experimental study with secondary RLS [7] might be due to pathophysiological correction of primary RLS and secondary RLS. To examine the effect of IV iron treatments on RLS, most controlled trials have been carried out for patients with normal iron store of ≥50 μg/L of serum ferritin levels [19-21]. Those trials might have targeted primary RLS rather than secondary RLS.
In this study, patients who had longer duration of RLS showed a higher risk of symptom persistence. Although we could not argue that the duration of RLS symptom and that of iron deficiency were the same, we might cautiously assume an association between both durations. Indeed, a close relationship between the decrease of serum ferritin level and the occurrence of RLS symptom has been reported in some RLS patients who had a tendency to rapidly deplete iron stores [15]. It has been reported that repeated experiences of RLS caused by multi-parity are strongly associated with increasing incidence of RLS not related to pregnancy [22], suggesting that repeated and chronic exposure of peripheral iron deficiency due to pregnancies might cause cumulative pathophysiologic changes on overall iron metabolism including brain, regardless of peripheral iron deficiency. Thus, longer duration of RLS in line with longer state of iron deficiency might have contributed to the development of primary RLS which was not improved with peripheral iron normalization in the present study. Another mechanism of disease duration-related RLS persistence could be associated with neuronal damages such as chronic hypoxia and myelin loss. These neuronal damages can be caused by brain iron deficiency because oxygen transport and myelin synthesis demand proteins, lipids, and cholesterol, all of which are iron dependent [23]. Therefore, it is important to notice that longer duration of RLS symptoms is a potential risk factor for RLS symptom persistence. Early intervention for RLS can provide a better chance for symptom improvement.
Older age at RLS diagnosis was another risk factor for RLS symptom persistence after iron normalization. In women, it has been found that serum ferritin levels remain low from adolescent until the menopause because of menstrual cycles and pregnancy. They gradually rise to levels comparable to those in males after menopause [24]. Meanwhile, the occurrence of RLS in elderly individuals is well known [25]. RLS prevalence increases with age. It reaches its peak around fifties in both genders with a clear tendency in women, then it remains as a plateau [26]. Thus, peripheral iron deficiency in middle aged to old RLS patients of this study might be an incidental finding rather than main causes of RLS. These patients might have persistent symptoms even after correction of peripheral iron deficiency.
When we observed the clinical course of RLS patients for at least 6 months or longer, the incidence of recurrence associated with iron deficiency was reported in two cases. The pattern of recurrence caused by recurrent iron deficiency has been reported in a previous study of Grote et al. [7] We found that RLS symptoms reappeared at 3 and 6 months after the initial oral iron treatment. Early et al. [27] have reported that five cases need to repeat IV iron injection due to recurred symptoms at an average of 6 months (range, 3 to 13 months) after the initial injection. It is currently unclear how long iron treatment needs to be provided to RLS patients with low serum ferritin levels or when iron deficiency will recur. RLS patients with iron deficiency may stop taking oral or IV iron after iron normalization and symptom improvement. They need to be regularly followed up to determine the recurrence of RLS symptom and iron deficiency.
This study has several limitations. First, a recall bias regarding symptom duration might have occurred because the data of onset age were collected depending on participants’ memory. The recall bias is, to some extent, unavoidable in retrospective observational studies for a long duration. Second, no information about IRLS scores was available at the follow-up interview. It was difficult to obtain IRLS scores from telephone interview, and many patients in the persistent group already took RLS medications, making it difficult to interpret the meaning of IRLS scores. Third, the range of follow-up period was too large (from 1 to 6 years). Participants with relatively short duration in the remission group could develop RLS symptoms in the near future. Nevertheless, this study provided valuable information about the clinical course of RLS patients with low serum ferritin levels after iron normalization. In secondary RLS with iron deficiency, the efficacy of oral iron replacement treatment was rather limited. Developing better methods for iron treatment and considering alternative treatment will be needed to control persistent RLS symptoms even after iron normalization. We found that longer duration of symptoms and older age at RLS diagnosis decreased the treatment effect of oral iron but increased the risk of symptom persistence. Therefore, this study provides clinical implication that early intervention of iron deficiency in RLS is needed.