Efficacy of the Life Goal-Focused Brief Intervention among Patients with Alcohol Use Disorder: A Preliminary Study
Article information
Abstract
Objective
The aim of this study was to examine the efficacy of the life goal-focused brief intervention, or the so-called the goal-focused self-regulation program (GFSRP), for patients with alcohol use disorder (AUD).
Methods
The GFSRP was developed as an 8-week group-program, which is based on a wide range of self-regulation theories, such as goal setting and implementation intentions. Patients with AUD (n=50) took part in the GFSRP and were compared to the control group (n=48). This study examined the changes in outcome measures from baseline to follow-up (12-week) in a mixed design.
Results
The GFSRP group had higher scores for the abstinence self-efficacy in negative affect situations than the control group at the post-test. In addition, it showed greater scores of optimisms compared to the control group. Furthermore, in the GFSRP group, there was no difference in intrinsic life goals from baseline to the 12-week follow-up, whereas the control group showed a significant decrease.
Conclusion
The GFSRP could increase the abstinence self-efficacy and optimism among patients with AUD. Moreover, it might prevent loss of life-goals as core factors in self-regulation among patients with AUD.
INTRODUCTION
The Epidemiological Survey of Mental Disorder of Korea reports that the lifetime prevalence of alcohol use disorder (AUD) is 13.4% (20.7% in males, 6.1% in females), which is the highest percentage of lifetime prevalence among mental disorders reported in Korean adults [1,2]. In addition, the estimated number of patients with AUD is almost 1.6 million individuals, and the one-year prevalence is 4.4% (6.6% in males, 2.1% in females), which is considerably higher than that for other mental disorders.
In Australia, the percentage of AUD patients receiving treatment is 22.4% [3], whereas it is no more than 6.6% in Korea. This emphasizes the need not only to intervene in AUD at a policy level and provide pharmacotherapy, but also to develop an effective way to intervene more systematically at the psychological level. The psychosocial intervention that is commonly applied to patients with AUD and proven to be effective includes the Twelve Steps of Alcoholics Anonymous, motivation-enhancement training, cognitive behavioral therapies, stress management, relapse prevention, and emotion regulation program [4,5]. However, these therapeutic methods may have different effects depending on the patient’s symptoms and level of motivation to change, therapeutic environment, and therapeutic aim (e.g., abstinence or moderation) [6].
AUD is known to be one of the mental diseases in which more than 50% of the patients who are discharged from the hospital relapse within one year, and suffer severe physical, psychological, social, and economic damage [7,8]. Therefore, rehabilitation and maximized functioning in everyday life are important for patients with AUD. Nevertheless, they rely mainly on specialized treatment for AUD, which can control the cues for drinking, instead of adaptation training in everyday life, due to realistic limits. Moreover, most of the programs mentioned above are generally sobriety-centered interventions. Putting an emphasis on the short-term goal of sobriety, in absence of long-term life goals, can be a limitation to enhancement of the motivation to change.
There is increasing theoretical and empirical evidence that indicates intervention in goal setting and implementation is a key element in not only successful rehabilitation of the patients with chronic diseases (e.g., stroke, diabetes) but also in prevention of recurrence [9,10]. However, life goal intervention is utilized for those who have a high functional level, largely in non-clinical aspects such as occupation, education, and sports [11].
Therefore, this study assumed that the interventions that can maintain or enhance the intrinsic life-goals will be helpful for preventing failure in alcohol control and maximizing adaptation to everyday life. Specifically, this study aimed to 1) develop the goal-focused self-regulation program (GFSRP) centered on goal setting and implementation intention [12,13], one of the self-regulation theories and 2) identify its effects on alcohol self-control failure, life goals, abstinence self-efficacy, and optimism in patients with AUD.
METHODS
A total of 98 male inpatients with AUD were recruited from alcohol centers of psychiatric hospitals. Patients who met the AUD diagnostic criteria in the Diagnostic Statistical Manual of Mental Disorders, 5th edition (DSM-5) [14] and received specialized treatment for AUD were included. Those who revealed their interest in participation after publication of the advertisement, but 1) showed serious aggression and hostility because they were psychologically very unstable, 2) were illiterate, 3) could not fill in a self-report questionnaire due to issues such as visual impairment or head injury, or 4) were difficult to enroll in this program because their judgment was deteriorated or their decision-making was impaired, were excluded.
This study was conducted in South Korea between March and December 2015 and received ethical approval from the Ajou University Institute Review Board (201412-HR-SB-002-02). All subjects voluntarily participated in the study and signed a consent form.
Development of the GFSRP
In this study, the GFSRP is based on the integrated definition that includes emotion regulation as well as goal orientation and goal implementation. Therefore, this study focused primarily on understanding that there are various life goals and assisting with the selection of preferred life goals. Additionally, the GFSRP applied balancing between “best possible self” and “worst possible self” [15,16] to facilitate future-oriented thinking. Furthermore, it aimed to apply implementation intention [17], which is known to be an effective strategy for enhancing goal implementation, to emotional and behavioral regulation.
Accordingly, the GFSRP consisted of 8 sessions (50 min each), which was administered once a week by a licensed psychologist. Components of the GFSRP were as follows: self-regulation and mental health (session 1); searching for purpose in life (session 2); goal orientation (session 3 and 4); goal-focused emotion regulation (session 5 and 6); goal implementation (session 7 and 8). On the basis of the previous research outcomes, the treatment duration was selected as 8 weeks to maximize the effects of the brief intervention. The treatment group took part in the GFSRP as well as a usual addiction specialized program, including addiction education, 12-steps therapy, and cognitive behavioral therapies (CBTs), whereas the control group received only the specialized addiction program.
Measures
To achieve homogeneity between the groups, severity of alcohol dependence, smoking preference, frequency of hospitalization, initial drinking age, recent period of abstinence, longest period of abstinence, blackout experience, and family history were investigated, in addition to the demographic variables.
The Korean version of Alcohol Dependence Scale (ADS-K) [18] was used to assess the severity of alcohol problems. ADS-K is a scale consisting of a total of 25 items, which is developed to assess compulsive drinking, behavior when drinking, and alcohol withdrawal symptoms [19]. In this study, the reliability of this scale was acceptable (α=0.96 at the pretest).
The Aspiration Index (AI) [20] was used to assess life goals. It consists of 6 factors, including intrinsic goals (personal growth, relationships, and community) and extrinsic goals (wealth, fame, and image). Korean version of AI is the Future Oriented Goals Scale (FOGS) [21]. In this study, the reliability of this scale was appreciable (pre-test α=0.96 for full scale, α=0.83 -0.95 for the subscale).
Alcohol abstinence self-efficacy was assessed with the Alcohol Abstinence Self-Efficacy Scale (AASE) (DiClemente et al., 1994). The AASE evaluates an individual’s efficacy in abstaining from drinking in 20 situations (four categories) that represent typical drinking cues. The Korean version of the AASE [22] was used, for which a solid subscale structure and strong indices of reliability and validity were demonstrated. In the present study, five items that examine cues related to negative affect were used, and the reliability of the instrument was appreciable (at the pretest, α=0.84).
To measure the optimism, the Korean version [23] of Life Orientation Test-Revised (LOT-R) [24] was used to measure the general positive expectations for the future. In this study, the internal consistency reliability of LOT-R was appreciable (at the pretest, α=0.64).
Statistical analysis
To identify pre-test homogeneity between GFSRP group and control group, χ2 test was conducted for categorical variables and independent sample t-test for continuous variables. In order to test the effects of treatment, different analyses were used for each dependent measurement based on the results from the normality test (Kolmogorov-Smirnov & Shapiro-Wilk’s test) of each scale. In other words, if normality could be assumed and pre-test homogeneity was achieved, repeated ANOVA or ANCOVA with pre-test score as covariate was conducted. In contrast, if the normality of measured values could not be assumed, “within-effects” were identified by conducting a Wilcoxon-Singed Rank Test W test (W test) and “between-effects” by conducting a Wilcoxon-Mann-Whitney U test (U test) [25,26].
At the same time, to compensate for limited significance testing that is affected by sample size, we aimed to closely investigate the effect of the program by considering the effect size. In relation to the effect size in ANCOVA, partial η2 [SSeffect/(SSeffect+SSerror)] provided by SPSS is likely to overestimate the effect size [27]. For this reason, to analyze the effect size of treatment in analysis of covariance, η2 (SSeffect/SStotal) was calculated, and η2=0.01, 0.06, and 0.14 can be construed as small, medium, and big effect size, respectively [28]. In addition, to analyze the effect size of W test, r=4x|W-[(R++R-)/2|/N(N+1) [29] was used, and to analyze the effect size of U test, r=1-(2U)/n1*n2] [30] was used. To compare the intensity of the two effect sizes, the correlation coefficients 0.10, 0.30, and 0.50 can be construed as small, medium, and large effect size, respectively. For statistical analysis, IBM SPSS 20.0 (IBM Corp., Armonk, NY, USA) was used.
RESULTS
Homogeneity of participants
The mean age of the entire group was 50.68 years (SD=8.82); the GFSRP group, 51.56 years (SD=7.94), and the control group; 49.77 years (SD=9.66). The mean education period of the entire group was 12.08 years (SD=2.82); GFSRP group, 12.20 years (SD=2.79), and the control group, 11.93 years (SD=2.88). The differences in age and education period for the all groups were statistically insignificant (Table 1).
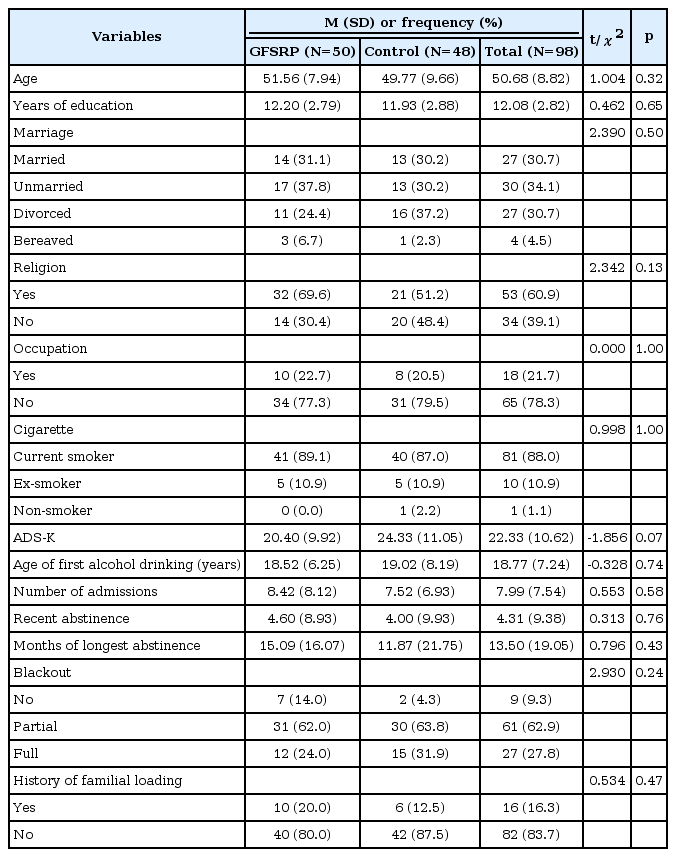
Demographic and clinical characteristics of subjects
In addition, in relation to alcohol use, there was no statistically significant difference in initial drinking age, recent abstinence period, longest abstinence period, blackout experience, and family history. At the same time, there was no significant difference between groups in terms of severity of AUD-K.
The difference between groups in life goals and optimism was not statistically significant and abstinence self-efficacy to negative affect was also not significantly different.
Outcome measures
Alcohol self-regulation
To know the effect of GFSRP, return-to-hospital-after-drinking cases when they went out or slept outside hospital were investigated from post-test to follow-up as behavioral measure and regarded as alcohol self-control failure. However, contrary to expectations, the difference in alcohol self-control failure between GFSRP group and control group was not statistically significant (χ2=4.511, p=0.105).
Life goals
In W test, intrinsic life goals were not significantly different for both GFSRP group and control group, compared to pretest, while in U test, the between-group difference of intrinsic life goals was not significant at post-test, and the effect size was also small (Table 2). However, the between-group difference was statistically significant at follow-up (12-week) and the effect size was medium or higher (Wendt’s r >0.30) (Figure 1, Table 3). When repeated ANOVA was conducted with mixed design of group (treatment vs. control; between-subject variables) and time (pre-test, post-test, and follow-up; within-subject variables) for the extrinsic life goals, the main effect of group and measurement point and the interaction of group and measurement point were not statistically significant.
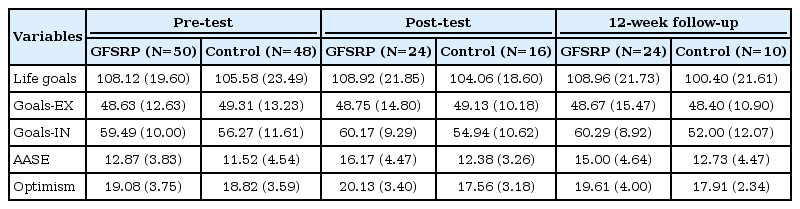
Descriptive of all outcome measures by groups and Times
Changes in intrinsic life goals from baseline to 12-week follow-up among patients with AUD. *p<0.05. GFSRP: Goal-Focused Self-Regulation Program, Goals-IN: Intrinsic life goals, Pre: pre-test, Post: post-test, 12 wk: 12-week follow-up.
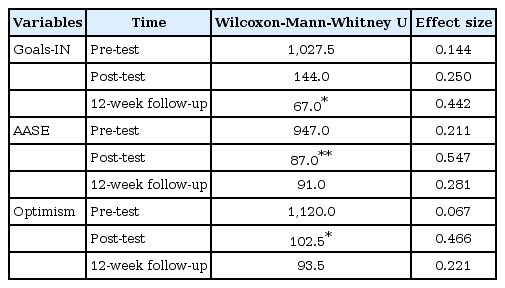
Group differences of outcome measures by times
Abstinence self-efficacy
As the abstinence self-efficacy to negative affect did not meet normality, W test and U test were conducted. In the W test, the abstinence self-efficacy to negative affect showed a significant increase at post-test in both the GFSRP group and the control group, but did not show a significant difference with pretest scores at follow-up (Figure 2). In contrast, in the U test, the abstinence self-efficacy to negative affect did not show a significant difference at pre-test, but the difference between groups was statistically significant at post-test, and the effect size was also medium or higher (U=87.000, p=0.004, Wendt’s r=0.547) (Figure 1).

Changes in alcohol abstinence self-efficacy to negative efficacy scores from baseline to 12-week follow-up among patients with AUD. **p<0.01. GFSRP: goal-focused self-regulation program, AASE: alcohol abstinence self-efficacy to negative affect, Pre: pre-test, Post: post-test, 12 wk: 12-week follow- up.
Optimism
Optimism did not show a significant increase at each point of measures compared to pre-test in W test. However, in U test, optimism was significantly higher in the GFSRP group at post-test than in the control group. Moreover, the effect size was also medium or higher (U=102.500, p=0.013, Wendt’s r=0.466), but there was no significant difference between groups at follow-up (Figure 3).

Changes in optimism from baseline to 12-week follow-up among patients with AUD. *p<0.05. GFSRP: Goal-Focused Self-Regulation Program, Pre: pre-test, Post: post-test, 12 wk: 12-week follow-up.
Life goals by duration of the intervention sessions
To identify the practical effect of the program developed by this study, the ANCOVA with pre-test score for each variable as a covariate was conducted to determine whether there is a difference in life goals at post-test between participants who completed all eight sessions (n=14) and those who could not complete one or more sessions (n=36). Prior to analysis, to assess the possibility of systematic elimination, homogeneity test for education drinking severity, alcohol control failure, initial drinking age, and frequency of hospitalization was conducted. As a result, it was found that the between-group difference for all variables was not statistically significant. Additionally, even after controlling the effect of the pre-test score in the total score of life goals, the group that completed all the sessions showed a high tendency compared to the group that did not complete the sessions (F=4.071, p=0.057, η2=0.048). Subfactor analyses revealed that the between-group difference of extrinsic life goals was statistically significant (F=5.138, p=0.034, η2=0.044). In addition, intrinsic life goals showed that the GFSRP group had a tendency to be higher than the control group (F=3.307, p=0.083, η2=0.060).
DISCUSSION
This study aimed to develop the GFSRP as one of the psychosocial interventions for patients with AUD and identify its effects on alcohol control failure, life goals, abstinence self-efficacy, and optimism. The study results indicated that group difference in optimism was significant at post-test. In other words, balancing between “best possible self” and “worst possible self” [16], which is similar to mental contrasting [31,32], known as one of the self-control strategies, is considered to be helpful for enhancing positive thoughts for patients with AUD. Therefore, interventions that can enhance optimism in groups with low motivation for change in behavior, as is the case with AUD patients, will be helpful for avoiding the learned helplessness caused by recurring frustration. Furthermore, as goal setting relies on expectations for the future, it will contribute toward setting a realistic goal by encouraging patients with AUD to recognize, approach, or avoid goals [33]. This is because this approach helps patients with AUD not only imagine the best possible future but also consider the worst possible future. That is, patients with AUD whose average age is in their 50s would find it difficult to escape from the self-definition of “addict”, not only due to frustration in life goals but also relapse. Therefore, the self-balancing training may have potential a clinical significance in the future, in that it can have a positive impact on enhancing the motivation to change in patients with AUD.
In addition, the between-group difference in abstinence self-efficacy to negative affect was significant at post-test. A number of previous researches predicted that abstinence self-efficacy determines future alcohol consumption and is considered an important predictor for recovering from AUD [34,35]. It has been used as a dependent measurement value in verifying the effectiveness of diverse abstinence programs. In particular, given that difficulty in emotion regulation to negative affect (i.e., anger, frustration) tends to select immediate gratification instead of long-term goal-oriented behavior by causing weakened self-control [36], the between-group difference of abstinence self-efficacy to negative affect might have been positively influenced by implementation intention training, which intends to maintain abstinence even in emotional stress situations [37], indicating that contextualized self-efficacy enhancement would be effective for generalized change. Consistent with this, the fact that abstinence-centered implementation intention training for patients with AUD has enhanced the abstinence self-efficacy to negative affect suggests that we can expect the generalization of implementation intention for various goals including future emotional regulation and health management.
Furthermore, the between-group difference of intrinsic life goals appeared consistently until follow-up; this is not because the life goal level of the GFSRP group increases linearly after pre-test, but because the life goal level of the control group after hospitalization tended to decrease gradually. This suggests that goal-focused self-regulation program is likely to have an effect in preventing the loss of goal that might occur after alcohol control failure. Especially, implementation intention training including action plan and alternative plan for achieving goals, rather than just setting an indefinite goal, is likely to maintain the orientation of life goals at follow-up.
Additionally, there was no difference in total score of life goals level between the group that completed the program and the group that could not complete the program at post-test. However, the group that completed the program had a higher interest in extrinsic life goals than did the other group. Further, the level of intrinsic life goals showed that the GFSRP group had a higher tendency compared to the control group. In other words, the group that completed the program showed a tendency for a varying goal range. In several previous researches, although extrinsic life goals had a negative impact on subjective well-being and were related to psychological dysfunction [38], they can be effective for reinforcing motivation in the initial stage of behavioral change [39]. In particular, the fact that extrinsic life goals are maintained or increased in groups with a very low motivation to change, as in the group with AUD, may bring further research. Consistent with this, the Self-Determination Theory [40] also states that autonomic motivation is consistent with the value of an act, and ideally, is a concept that includes internal motive and external motive that can be integrated with the sense of self. Therefore, the fact that extrinsic as well as intrinsic life goals are higher in the group that completed the goal-oriented program than in the group that did not, when the program was carried out in the patients with AUD who have a low motivation level, suggests that we can expect it to be helpful for future behavioral change and subjective well-being enhancement.
Contrary to expectations, however, the between-group difference in alcohol control failure as a behavioral measurement value after the completion of the program was not significant. Given that the initial drinking age of study participants was 18.52 years on average (SD=6.25), and most of them were patients who had experienced a relapse, there would be a limit in improving alcohol control failure directly because the program was a self-regulation program targeting AUD Type 2 [41,42].
This study has some limitations as follows. First, alcohol control failure could not be assessed accurately due to the study participants’ sudden discharge from the hospital and outpatient follow-up failure. Second, random assignment for both GFSRP group and the control group could not be performed. Third, the degree of participation in the existing hospital ward program could not be determined. Finally, this study was analyzed without an additional control group such as sham program or non-treatment condition. Considering these factors, the GFSRP may only be considered an empirically supported treatment, needing to replicate using more deliberate design.
Despite these limitations, this study has clinical implications as follows. First, previous researches [43-45] revealed the relation between life goal and alcohol use, but programs that help in setting life goals and facilitate their implementation have not been developed yet in Korea; verification of effectiveness has also not been performed. This suggests preliminarily that the goal setting-based self-regulation program is applicable to severe psychological disorders like AUD. Second, as GFSRP helps to enhance optimism and abstinence self-efficacy and maintain intrinsic goals in patients with AUD, it can compensate for the limitation of interventions in mindfulness enhancement, which do not induce actual behavior change.
Finally, we have some suggestions for future research. First, this study could not keep monitoring strictly over study participants when the GFSRP was conducted as part of the hospital ward program. Furthermore, the number of participants who completed the eight-session program was considerably low. Therefore, it seems necessary to select subjects who have a high motivation to participate in the program, implement the goal-focused self-regulation program in a short-term intensive way, and verify the effectiveness. Second, this study examined the alcohol control failure as a behavioral measurement value; however, it was difficult to evaluate this value accurately due to lack of follow-up. To identify the long-term effect of the program systematically, it seems necessary to examine the abstinence rate and actual behavioral change by applying the outpatient follow-up after discharge from the hospital into the study design process (e.g., using the experience sampling method). Finally, given that maximized functioning is emphasized in AUD rehabilitation and other various clinical settings, it is necessary to check if the short-term intensive program has an effect in improving function. In particular, given that the motivation for goal setting is low due to chronic alcohol control failure, it is necessary to add therapeutic interventions that can enhance the motivation to change before goal setting and implementation intention formation. As an alternative, it is necessary to develop a program that integrates individual sessions and small-scale group sessions for reinforcing motivation.
In contrast, goal setting, or the more relevant goal adherence, requires good executive control. Long term alcohol use impedes executive control (or, as some would argue, poor executive control precedes an AUD) [46,47]. Therefore, it is necessary to consider cognitive rehabilitation training considering the patient’s cognitive profile prior to the target intervention [48,49].
Generally, life goals are formed in early adolescence and adulthood and are known to be as a rather stable variable that determines one’s life. However, the content of life goals depends on an individual’s age [50]. Thus, it seems necessary to develop a small-scale group program by age and an approach to individual cases in order to enhance the effect of the goal-focused program for patients with AUD. Further, given that self-efficacy is most important in goal-focused self-regulation, consistent practice that is based on thorough preparation, i.e. repeated successful experience, will be helpful in enhancing self-efficacy in order to achieve long-term goals.
As the GFSRP is under development, the expectations of appreciable changes in patients with chronic AUD through short-term psychosocial interventions, which might be inadequate for affecting a behavioral change, may not be realistic. Nevertheless, numerous researchers and therapists’ efforts in developing psychosocial interventions, considering the characteristics of patients, and verifying their effectiveness are expected to be instrumental in life goal setting and implementation for patients with AUD.
Acknowledgements
The authors thank Min-Kyu Lee for his supervision of the development of this article.