Suicidal Ideation Predicts Functioning and Quality of Life Over One Year after Acute Coronary Syndrome
Article information
Abstract
Objective
This study investigated the associations of suicidal ideation (SI) evaluated within 2 weeks after an acute coronary syndrome (ACS) episode with functioning, disability, and quality of life (QOL) at a 1-year follow-up assessment.
Methods
This study recruited 1152 consecutive patients within 2 weeks of a confirmed ACS episode; 828 of these patients who were followed up 1 year later comprised the study sample. SI was determined at baseline using the “suicidal thoughts” item of the MontgomeryÅsberg Depression Rating Scale. At both examinations, social and occupational functioning were measured by the Social and Occupational Functioning Assessment Scale (SOFAS), disability was estimated by World Health Organization Disability Assessment Schedule-12 (WHODAS-12), and QOL was assessed using the World Health Organization Quality of Life-Abbreviated form (WHOQOL-BREF). Baseline covariates included sociodemographic data, depression characteristics, cardiovascular risk factors, and current cardiac status.
Results
SI at baseline was independently associated with less improved or decreased scores on the SOFAS, WHODAS-12, and WHOQOL-BREF over 1 year after adjusting for relevant covariates.
Conclusion
SI within 2 weeks of an ACS episode predicted poorer functioning and QOL at a 1-year follow-up assessment. Thus, the simple evaluation of SI in patients with recently developed ACS could be helpful in screening for functioning and QOL during the chronic phase of this disease.
INTRODUCTION
Suicide is a major public health problem worldwide [1], and suicidal behavior has been associated with poor mental health [2]. In particular, suicidal behavior is strongly associated with depression, in that such behavior strongly predicted depression relapse and persistence in depressive patients [3,4]. Suicidal behavior may also be associated with functional aspects of mental health such as social functioning, disability, and quality of life (QOL). However, this issue has rarely been investigated, and most studies have been cross-sectional in design [5,6].
Suicidal behavior occurs more frequently in patients with severe physical disorders than in the general population [7]. In particular, epidemiological and clinical studies have demonstrated that patients with acute coronary syndrome (ACS) are at increased risk for suicidal behavior [8,9]. Therefore, the association between suicidal behavior and worse mental health may be more prominent in patients with ACS. In this regard, we previously reported that suicidal ideation (SI) within 2 weeks after an ACS episode predicted poorer outcomes on measures of depression at a 1-year follow-up assessment, similar to findings for patients with depression [10]. However, no studies have investigated the effects of suicidal behavior on the functional aspects of mental health in patients with ACS, although treatment becomes focused on improving general health and functional status after the acute stage of ACS [11].
The spectrum of suicidal behavior ranges from SI and attempts to completion [12]. In clinical studies of ACS, SI was typically used as a phenotype [9,13]. Thus, the present study investigated the effects of SI, identified within 2 weeks of an ACS episode, on social functioning, disability, and QOL at a 1-year follow-up assessment.
METHODS
Study outline and participants
The present analysis was carried out using data from the Korean DEPression in ACS (K-DEPACS) study, which investigated the epidemiology of depressive disorders in ACS patients using a naturalistic prospective design. The study design and rationale have been published [14,15]. Of 4809 patients in the Department of Cardiology of Chonnam National University Hospital (CNUH) in Gwangju, South Korea, from 2006 to 2013 with recently developed ACS, 1152 met the eligibility criteria and agreed to participate in the study. Baseline evaluations made within 2 weeks after hospitalization for ACS included SI, sociodemographic and clinical characteristics, and functional status in terms of social functioning, disability, and QOL. At 1 year after the baseline evaluation, 828 patients were successfully followed up; this group comprised the present study sample. Follow-up evaluations were conducted in an outpatient setting, and the same functional status variables were assessed. Written informed consent was collected from each participant, and the study was approved by the CNUH Institutional Review Board (IRB No. 06-050).
Suicidal ideation
The presence of SI was identified using the “suicidal thoughts” item of the Montgomery-Åsberg Depression Rating Scale (MADRS-ST) [16]. This item assesses the feeling that life is not worth living and the existence of plans for suicide, with scores ranging from 0 (life satisfaction) to 6 (explicit plans for suicide). As in previous studies [17,18], we considered suicidal thoughts as being present if the patient scored ≥2 on this item, where a score of 2 refers to fleeting suicidal thoughts.
Sociodemographic and clinical characteristics
Sociodemographic data on age, gender, duration of education, living status (living alone or not), housing (owned or rented), and current occupation (employed or not) were obtained. With regard to depression characteristics, previous and family histories of depression and scores for depressive disorder based on the Diagnostic and Statistical Manual (DSM)-IV were collected [19]. The following cardiovascular risk factors were evaluated: diagnosed hypertension and diabetes mellitus, hypercholesterolemia by fasting serum total cholesterol level (>200 mg/dL), obesity by measured body mass index (BMI) (>25 kg/m2), reported current smoking status, and previous and family histories of ACS. As a measure of current cardiac status, the severity of ACS was estimated by the Killip classification [20], left ventricular ejection fraction (LVEF) was estimated using echocardiography, and serum cardiac biomarkers troponin I and creatine kinase-MB (CK-MB) were measured.
Functional status
Social and occupational functioning was measured by the Social and Occupational Functioning Assessment Scale (SOFAS) [21], which takes into account functional impairment caused by both physical limitations and mental problems. The SOFAS considers social and occupational functioning across a continuum that ranges from 100 (optimal functioning) to 1 (serious functional impairment). Disability was estimated using the World Health Organization Disability Assessment Schedule-12 (WHODAS-12) [22]. The WHODAS-12 covers six domains: cognition, mobility, self-care, getting along, life activities, and participation. For each of the 12 items of WHODAS-12, respondents must rate their ability to undertake the addressed activities during the previous 30 days using a 5-point scale (no difficulty-extreme difficulty). A summary index is available, with scores ranging from 0 to 100; higher scores indicate higher disability. QOL was assessed by the World Health Organization Quality of Life-Abbreviated form (WHOQOLBREF), a 26-item self-administered questionnaire with items rated on a 5-point scale [23]. WHOQOL-BREF evaluates four domains: physical factors, psychological factors, social relationships, and environmental context. The physical domain includes seven items including pain and discomfort; the psychological domain includes six items including positive affect; the social domain includes three items including personal relationships; and the environmental domain includes eight items including financial resources and transportation. Because the psychological domain includes depressive symptoms, this subscale was excluded, and the remaining three subscales were analyzed. Raw subscale scores were converted to a scale ranging from 0 to 100 to facilitate comparison with other instruments; final scores represented the percentage of the total possible score achieved, with higher scores indicating better QOL.
Statistical analyses
Baseline sociodemographic data, depression characteristics, cardiovascular risk factors, and current cardiac status were compared between patients with and without SI using either t-tests or chi-squared (χ2) tests. The associations of SI at baseline with changes in the scores on SOFAS, WHODAS-12, and WHOQOL-BREF (values at 1 year minus values within 2 weeks after ACS onset) were evaluated using repeated-measures analysis of covariance to calculate group × time interactions after adjusting for corresponding baseline scores and covariates associated with SI at baseline (p<0.05). The Bonferroni correction was used to maintain an overall type I error rate of 0.05 against multiple comparisons for four Leeds Sleep Evaluation Questionnaire (LSEQ) outcomes; a two-sided p-value of 0.01 (0.05/5) was used to define statistical significance. Statistical analyses were carried out using SPSS 21.0 software (IBM Corp., Armonk, NY, USA).
RESULTS
Socio-economic and clinical characteristics by suicidal ideation
SI at baseline was present in 164 (19.8%) of the 828 study participants. Table 1 presents baseline characteristics of those with and without SI. SI was significantly associated with female gender, lower education, rented housing, current unemployment, previous history of depression, DSM-IV depressive disorder, and higher troponin-I levels. Table 2 summarizes adjusted associations between simultaneously entered baseline characteristics and suicidal ideation. In the acute phase of ACS, suicidal ideation was independently associated with past history of depression, depressive and anxiety disorders, and higher troponin-I levels.

Baseline characteristics by suicidal ideation (SI) in 828 patients with acute coronary syndrome (ACS)
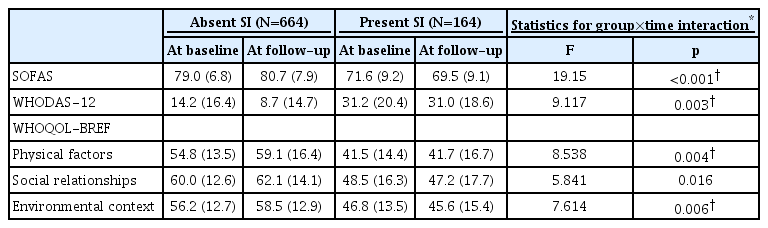
Scale scores by baseline suicidal ideation (SI) at baseline and at follow-up (N=828)
Associations of SI at baseline with changes in functional status over 1 year
The associations between SI within 2 weeks of the ACS episode and changes in functional status over 1 year are summarized in Table 2 and illustrated in Figure 1. SI at baseline was independently associated with less improvement or a decrease in the scores on SOFAS, WHODAS-12, and all three domains of WHOQOL-BREF at 1 year post-ACS after adjusting for gender, education, housing, current employment, previous history of depression, DSM-IV depressive disorder, and troponin I levels. After applying the Bonferroni correction, the associations remained significant for SOFAS, WHODAS-12, and the physical and environmental domains of WHOQOLBREF in the same adjusted model.
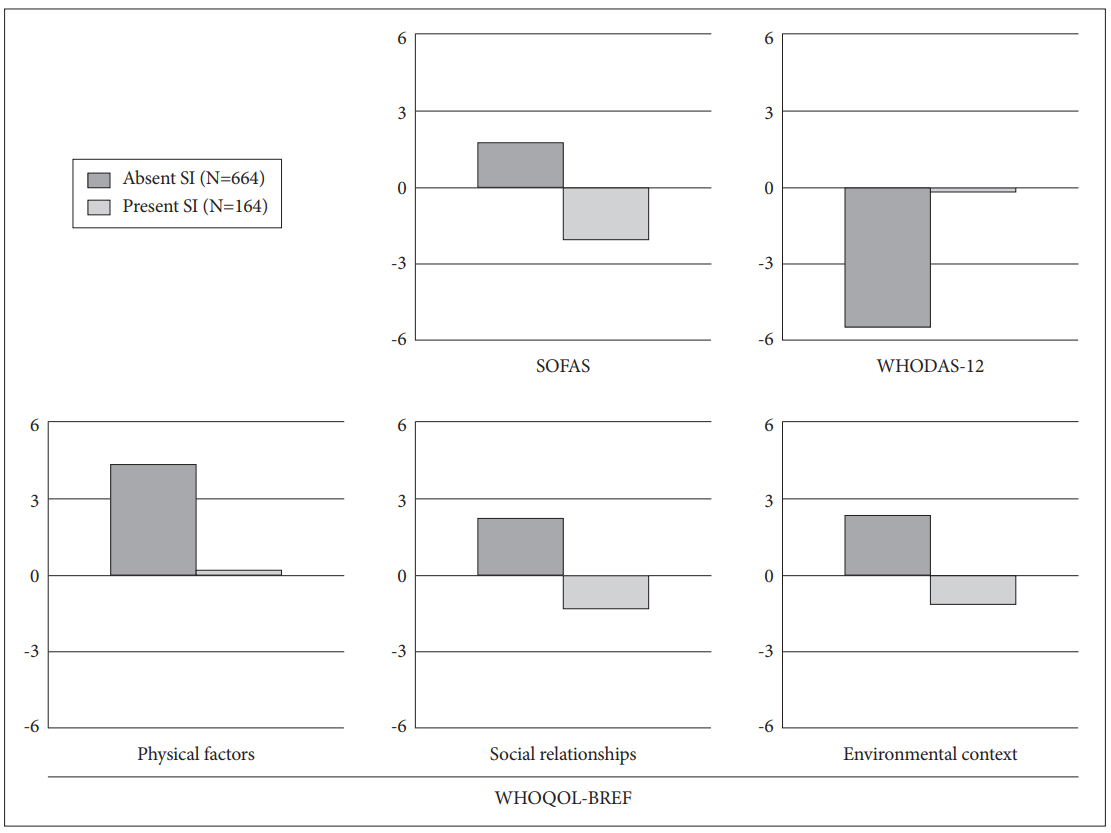
Changes in scale scores by baseline suicidal ideation (SI) over one year follow-up (N=828). SOFAS: Social and Occupational Functioning Assessment Scale, WHODAS-12: World Health Organization Disability Assessment Schedule-12, WHOQOL-BREF: World Health Organization Quality of Life-Abbreviated form.
DISCUSSION
The principal findings of this study were that documented SI within 2 weeks after ACS independently predicted less improvement or a decrease in social functioning, increased disability, and reduced QOL during the 1-year follow-up period. These findings were robust after adjustment for a range of demographic and clinical covariates related to SI, including depression characteristics.
In the acute phase of ACS, there is pressing need for intensive medical treatment to save the patient’s life and minimize sequelae [24]. However in the chronic phase of ACS, priority is given to treatment aimed at improving functional status [11]. Previous studies have found only minimal or no association between cardiac disease severity and functional status [25,26]. Rather, depression has been identified as the most significant factor predicting functional status in ACS [27,28]. Other psychosocial factors including life stress or social support also predicted functional status in ACS [29-31]. The present study is the first to report the predictive value of SI for functional status in ACS. This finding might be expected due to the fact that SI is one of the diagnostic criteria for depressive disorders [19], so SI may be fully explained by depression. However, previous research has suggested that pathophysiological characteristics of SI are independent of underlying psychiatric disorders, including depression [32,33]. Moreover, the associations of SI with elements of functional status remained significant even after adjustment for depression characteristics. Screening for depression is conventionally recommended for all patients with ACS because this disorder is significantly associated with increased psychiatric morbidity and mortality [34]. The present findings suggest that screening for SI may also be important for ACS patients due to the predictive value of SI at baseline for functional status 1 year later.
Before drawing conclusions from the findings of the present study, several methodological issues should be considered. First, the main exposure variable was SI, and although SI is closely related to more severe suicidal behaviors [35], no data concerning suicide attempts were obtained. However, previous clinical studies of patients with ACS or other severe physical disorders have also used SI as a phenotype, as more severe forms of suicidal behavior are rare in this type of study [9,36]. Second, SI was identified using the “suicidal thoughts” item of the MADRS rather than being defined using a separate or formal instrument. However, this method has been used in previous studies investigating patients with severe physical disorders as well as patients with depressive disorders [14,17,37]. Furthermore, a recent study reported that an item pertaining to suicidal thoughts taken from a depression rating scale had good validity [38]. Third, it is important to bear in mind that the follow-up assessment was performed at only a single time point and not throughout the 1-year period; thus, it was impossible to determine the nature or course of functional status between examinations.
This study has several strengths. First, participants were recruited consecutively from among all eligible patients with recent ACS, and all measurements were assessed at similar time points (i.e., at 2 weeks and 1 year after ACS), which reduced the risk of error arising from heterogeneous examination times. Second, all measurements of psychiatric and cardiovascular status were well validated. Third, functional outcome was assessed across three comprehensive concepts: social function, disability, and QOL. Fourth, a range of covariates was considered in the analyses.
ACS is the leading cause of disease burden worldwide [39]. The present findings suggest that the simple evaluation of SI in patients with recently developed ACS in a hospital setting could be helpful in screening for functional status over 1 year of this disease. The long-term effects of SI on the treatment, course, and prognosis of ACS should be determined in future research.
Acknowledgements
This study was supported by grants of the Korea Health 21 R&D, Ministry of Health and Welfare, Republic of Korea (HI12C0035), and was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Science, ICT and future Planning (NRF-2016R1A2A2A05919518).