INTRODUCTION
Given that the majority of suicide victims and survivors have a history of mental illness and that suicide-related behaviors are more likely to be shown by those with mental illnesses than those without, suicide is considered to be a serious mental health problem [1]. In South Korea, 13.3% of patients who visited the emergency department due to psychological problems showed suicide-related problems, and 38.5% of suicide victims were found to have a history of emergency department visits due to a previous suicide attempt [2]. Suicide attempts (SA) are generally a risk factor for suicide, and greater frequency of SA increase the likelihood of death from suicide [3]. Another suicide risk factor is suicidal ideation (SI), which manifests in various ways, from general thoughts of suicide to detailed suicide plans. This is a process of cognitive thought that precedes suicidal behavior and is regarded as an important indicator of SA [4].
While it appears similar to suicidal behavior, self-injury, an act of directly and deliberately harming oneŌĆÖs body, is considered a clinical syndrome independent of suicide [5,6]. Suicidal behavior is motivated by the clear desire to die and to ease oneself and others through death. But self-injury is performed to control aversive internal conditions such as anxiety, depression, and anger, to endure difficult situations, or as self-punishment. Based on the differences in motivation and purpose of such behaviors, the two behaviors were classified as suicidal behavior and non-suicidal self-injury (NSSI) in the Conditions for the Further Study chapter of the recent 5th edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) [7]. Nevertheless, repeated NSSI is still considered a risk factor for suicide in that it increases the likelihood of suicidal behavior while reducing the fear of pain [1,3].
Temperaments and characters are among the factors affecting behaviors related to suicide and self-injury [8,9]. Temperaments refers to the tendencies for an automatic emotional response to environmental stimuli, and they are relatively stable traits throughout life in relation to the genetic aspects [10]. Temperaments include novelty seeking, a tendency to respond actively to novel stimulations and reward cues; harm avoidance, a tendency toward an inhibitory response to punishment or harm signals; reward dependence, a tendency for a positive response to signals of social rewards; and persistence, a tendency to steadily continue a once rewarded action without constant reinforcement. On the contrary, characters are relatively conscious self-concepts, such as the differences between goals and values of an individual, formed through interactions with the environment and continuously changed throughout life while being influenced by socio-cultural learning. Characters involve self-directedness related to self-efficacy and the ability to regulate behavior; cooperativeness related to being agreeable in oneŌĆÖs relations with other people; and selftranscendence related to the acceptance and appreciation of spiritual and religious beliefs. Many previous studies have consistently shown that high harm avoidance is associated with SA and SI [11-15]. On the other hand, some studies have found that suicide-related behaviors are associated with high levels of novelty seeking [16,17], while a study has found that its effect disappears when controlling for the depression level [18]. As such, the effect of novelty seeking on suicidal behaviors is inconsistent between studies, and the influences of other personality and temperament traits are also unclear [9].
However, many previous studies regard SA and SI as a single category without distinction, and did not consider NSSI by grouping self-harm patients into those with suicidal tendencies. Additionally, although there is an increasing interest in NSSI, attempts to identify their temperaments and characters are still limited [13,14]. Moreover, as studies that control for depressive symptoms are quite uncommon despite research showing their significant effects on suicide-related behaviors [3], putting limitation on accurately identifying the unique effects of each factor. Therefore, this study classified high suicide risk (HSR) subjects into the SA, SI, NSSI groups to identify the temperaments, characters, and discriminants of each group. Furthermore, the study examined the differences in temperaments and characters between the HSR patients and psychiatric patients without suicidal tendencies (PP). In this process, the study controlled for the level of depression was to explore whether the temperament variable directly explained suicidal tendencies and self-harm. The study hypothesized that each group would vary in temperaments and characters, and that the NSSI group would be particularly distinguished from other two groups.
METHODS
Research subjects and procedures
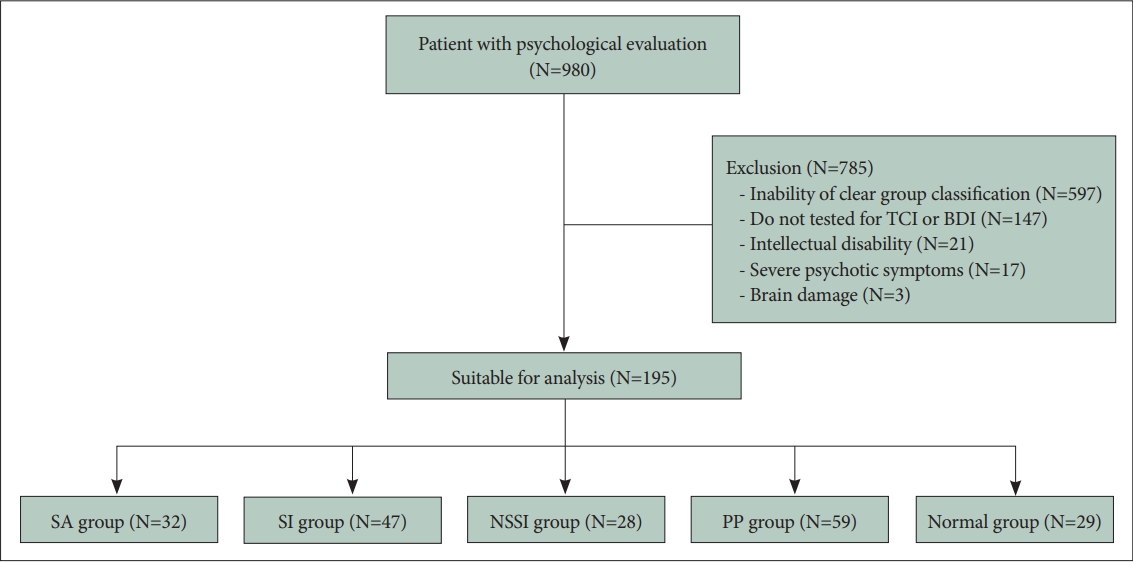
This study examined the electronic medical records of 980 patients who received a diagnostic psychological evaluation at the department of psychiatry at Hanyang University Guri Hospital in Gyeonggi-do, Republic of Korea, from September 2009 to March 2020. Among them, 147 patients who were not tested for Temperament and Character Inventory (TCI) or Beck Depression Inventory (BDI) were excluded, and 41 patients who had difficulties in self-report due to brain damage, intellectual disability, or severe psychotic symptoms were excluded from the analysis because of the impaired reliability of their reports. Lastly, in the process of confirming suicidal tendencies during the clinical interview, 597 patients who did not provide clear information on any of SA, SI, or self-injury were excluded from the analysis due to the inability of clear group classification. Finally, 195 patients were classified into the SI, SA, NSSI, PP, and Normal groups and used for analysis (Figure 1). Sex, age, educational level, current psychiatric disorder, and current level of depression were recorded for all study subjects (Table 1). The patientsŌĆÖ diagnosis of mental illness was provided from their electronic medical records, based on the Structured Clinical Interview for DSM-IV Axis I Disorders, clinician version, conducted by three psychiatric doctors during the first to third medical examination [18]. All research protocols were approved by the Institutional Review Board of Hanyang University Guri Hospital (IRB No. 2019-03-018), and prior consent was waived because the data was obtained through retrospective medical chart review that was performed by two clinical psychologists using psychological evaluation reports and electronic medical records.
Group classification
The patients were classified into the following five categories based on the retrospective medical chart review that included self-reported or guardian-reported cases of HSR, that is, SA, SI, and NSSI: 1) the SA group consisting of those having SI and a history of SAwithin the past year as of the time when the evaluation was conducted; 2) the SI group consisting of those having SI without any history of self-injury orSA; 3) the NSSI group consisting of those with no history of suicide attempt within the past year and whose behaviors corresponded to NSSI in DSM-5 that was defined as deliberate damage to oneŌĆÖs body without intent to die; 4) the PP group consisting of those who did not experience SI within the past year and did not have a history of suicide-related behavior; and 5) the Normal group consisting of those with no history of suicidal or self-harming behaviors. They were donors of kidney transplants or job seekers who had been psychologically evaluated at the hospital and did not score high on any of the Minnesota Multiphasic Personality Inventory-2 scales.
Measurement tools
Temperament and Character Inventory-Revised Short version
TCI is a self-report questionnaire developed by Cloninger et al. [10] to measure temperaments and characters. The validated Korean version was used for this study, which consisted of 140 items on a five-point Likert scale [19]. TCI is composed of seven scales and 29 subscales spanning four temperament dimensions (novelty seeking, harm avoidance, reward dependence, persistence) and three character dimensions (selfdirectedness, cooperativeness, self-transcendence).
Korean-Beck Depression Inventory-II
BDI is an evaluation tool developed by Beck et al. [20] (1961) to measure the severity of depressive symptoms. It measures depression, guilt, SI, and sleep problems. The validated Korean version was used for this study, which consisted of 21 items measured on a four-point Likert scale [21]. The total score was used for analysis, with a greater average score indicating more severe depressive symptoms.
Data analysis
First, descriptive statistics were performed on the demographic characteristics of each group, and a chi-square test and an analysis of variance were performed to identify differences between the groups. A multivariate analysis of variance was then conducted to determine if there were differences in temperaments and characters for each group. In this process, level of depression, psychiatric diagnosis, and academic background were set as covariates to control their influence. Finally, a multinomial logistic regression analysis was performed to confirm whether temperaments and characters (the independent variables) could discriminate the HSR group (the dependent variables). The Statistical Package for Social Sciences (SPSS) for windows 22.0 (IBM Co., Armonk, NY, USA) was used for all analyses, and statistical significance of the analysis was defined as a two-tailed p-value of less than 0.05.
RESULTS
Demographic characteristics
There was a total of 195 participants with a mean age of 27.18 (SD=12.34), ranging from 18 to 68 years of age. Among them, 32 participants were assigned to the SA group, 47 to the SI group, 59 to the PP group, and 29 to the Normal group. Significant differences were observed among the groups for level of depression [F(4, 195)=2.499, p<0.05], type of mental illness (Žć2=259.98, p<0.001), and level of education (Žć2=24.796, p<0.05). Level of depression was highest for the SA group and was significantly higher than all groups except the NSSI group. For diagnosis, anxiety disorders in the PP group and personality disorders in the NSSI group appeared in greater proportions than in other groups. In the case of education, the HSR group had a higher percentage of high school graduates, whereas other groups had a higher percentage of university graduates (Table 1).
Temperament and character differences among groups
Significant differences were observed in novelty seeking [F(4, 195)=4.154, p<0.01], harm avoidance [F(4, 195)=7.833, p<0.001], and persistence [F(4, 195)=3.762, p<0.05] for temperaments, and in self-directedness [F(4, 195)=9.727, p<0.001] for characters. To be specific, the Normal group showed lower novelty seeking compared to other groups (p<0.05), and among the HSR groups, the NSSI group showed higher novelty seeking compared to the SI group (p<0.05). Moreover, the Normal group had the highest harm avoidance score followed by PP and HSR (p<0.05), and between HSR groups, the NSSI group showed higher harm avoidance compared to the SA group (p<0.05). The NSSI group reported lower persistence compared to the SA, PP, and Normal groups. The HSR groups had the highest self-directedness followed by the PP and Normal groups (p<0.05), and between the HSR groups, SA groups showed higher self-directedness than the NSSI group (p<0.05) (Table 2).
Logistic regression analysis
A logistic regression analysis was conducted to identify the discriminants for the SA, SI, and NSSI groups within the HSR groups. SA was more likely than NSSI to have greater persistence (odds ratio [OR]=1.085, p<0.05). On the other hand, higher novelty seeking led to a greater likelihood of classification into NSSI as opposed to SI (OR=0.916, p<0.05). While not included in the table, no variables were found to discriminate between SI and SA when SA was set as a reference group (Table 3).
DISCUSSION
This study classified the SI, SA, and NSSI groups to identify the differences in temperaments and characters of each group. It also examined whether these differences could play a role in discriminating each group. Not only all clinical groups including the HSR groups showed higher levels of novelty seeking than the normal group as shown in previous studies [16,17], but the NSSI group showed higher novelty seeking than the SI and PP groups. According to NockŌĆÖs (2009) pragmatic hypothesis [5], individuals with high novelty seeking take measures to quickly and easily alleviate negative emotions, rather than benefiting from long-term goals or objectives. Self-harm can be an attractive tool for those with high novelty seeking as it does not require special tools or pre-calculations [22]. Also, studies on the biological effects of NSSI have shown that self-injurers experience a phenomenon similar to an addiction, as endorphins are produced to alleviate and calm pain following an injury [23]. Therefore, it appears that when an individual with high novelty seeking experiences such pleasure, they are more likely to repeat NSSI in uncomfortable situations.
The clinical group showed higher harm avoidance compared to the normal group, and the HSR patients were found to have higher harm avoidance than the PP group. Since harm avoidance is related to worrying and pessimistic thoughts as it focuses on predicting and avoiding harm in daily life, those with harm avoidance feel more fear and less psychological security in uncertain situations [24]. In other words, anticipatory anxiety makes one expect negative rather than positive events in neutral situations. Therefore, individuals with high harm avoidance can be seen to contemplate suicide or self-injury as a means of avoiding uncontrollable anxiety when they expect a catastrophic result [11-15].
An interesting finding in this study was that the NSSI group showed significantly greater harm avoidance compared to the SA group. Both NSSI and SA may choose to escape the pain that they believe they have no control over. However, NSSI is generally a strategy for emotional control, known to be more frequent and less intense than SA [6,25]. Conversely, those who engage in NSSI can frequently feel psychologically uncomfortable in daily life. Thus, individuals with high harm avoidance could be more closely related to NSSI in that they tended to be more cautious in their surroundings and were more likely to feel negative emotions even from minor stimuli.
Furthermore, the NSSI group was found to have lower persistence than the Normal, PP, and SA groups. This result conflicted with previous studies stating that persistence cannot discriminate between the NSSI and non-NSSI groups [8,14]. Such a result may be attributed to the nature of persistence. Unlike novelty seeking or harm avoidance, persistence is a two-way factor. Low persistence can be considered as a maladaptive trait in situations where continuous effort is needed for problem solving, given its nature of giving up easily in face of frustration, criticism, fatigue, and obstacles. On the contrary, it can also be considered as an adaptive temperament that allows for a change in strategies in situations where rewards quickly change [10]. Considering this, the effect of the level of persistence on NSSI could change depending on an individualŌĆÖs environmental context. Another possibility can be attributed to cultural differences between Eastern and Western cultures, given that previous studies have emerged mainly in Western countries such as the United States. In the case of other countries, self-punishment was the most common personal motivation for self-harm [15]. On the other hand, in South Korea, a large proportion of self-harm was motivated by emotional relaxation, such as the reduction of negative emotions [26]. Therefore, although the relationship between the level of persistence and NSSI is ambiguous when the purpose of NSSI is self-punishment, NSSI appears to be more closely related to a low level of persistence when the purpose is a reduction of negative emotions, as it is used to solve the pain caused by a particular situation.
Among characters, only self-directedness showed a significant difference between the groups. More specifically, the Normal group had the lowest self-directedness, followed by PP and HSR respectively, and this result was similar to that of previous studies [11,14,27]. A low level of self-directedness is associated with difficulty in controlling emotions especially in situations where negative emotions are experienced [28]. Also, those with low self-directedness may experience difficulty in pursuing long-term goals and are characterized by a lack of confidence in their ability to resolve difficult situations [29]. Thus, they not only experience difficulty in controlling their emotions when facing negative emotions or difficult situations, but also may despair in their ability to overcome them. Eventually, they may attempt to resolve them using extreme measures such as suicide or self-injury [14].
In particular, the NSSI group was found to have lower selfdirectedness than the SA group among the HSR groups. While there are no prior studies on this, the consideration of the motivations and purposes of SA and NSSI could be a possible explanation. While individuals who attempt to commit suicide think they can personally end their problems through their own death, motivations for NSSI include temporary psychological stability and the aim to receive help by showing the injury to others [15]. Thus, individuals who engage in NSSI may have lower self-assurance in their ability to solve problems on their own.
Finally, no temperament or character that can discriminate between all three HSR groups was found from the logistic regression. However, between the SA and NSSI groups, those with higher persistence were found to be more likely to engage in SA, and between the SI and NSSI groups, those with higher novelty seeking were found to be more likely to engage in NSSI. Considering the study hypotheses, pain tolerance between SA and NSSI, and acting out tendencies between SI and NSSI can be seen as core discriminants between the groups. However, this cross-sectional study cannot make causal inference between temperaments and characters and suicidal behavior; we cannot say that they increase the risk of suicidal behavior. Nevertheless, the result is significant as it can serve as an empirical basis for longitudinally analyzing suicidal transition by classifying mentally ill patients according to their temperaments and characters.
On the other hand, no significant differences were observed between the SA and SI groups in this study. This could be attributed to the fact that SA and NSSI were separately analyzed in this study unlike the existing studies. Previous studies may have shown significant differences due to the characteristics of serious NSSI patients who were classified together in the SA group. Another possibility could be because we controlled for the level of depression. That is, this result may support the previous studies that found the level of depression to be the sole factor that affected the progression from SI to SA [3].
There are several limitations in this study. First, while this study classified the HSR group into SA, SI, and NSSI groups, it was difficult to closely examine their suicide and self-injury characteristics using objective evaluation tools as this was a retrospective study using chart review. In particular, there was a loss of data from excluding self-injury patients who could not be clearly identified as NSSI from the data collected from clinical interviews. It led to a small sample size for statistical analysis, which might cause bias in age or diagnosis in the classification process. Therefore, future studies need objective evaluation tools for classification and increased statistical power with a larger sample size. In particular, future study can use objective evaluation tools to measure variables such as frequency and type of SA, severity of suicide ideation, and self-harm motivations, methods, and frequency, in order to understand their relationship with temperaments and characters in detail in future studies.
Second, the Normal group used in this study was composed of people who were evaluated to have no psychological problems related to kidney transplants or task performance. Thus, it is possible that they responded in a socially positive manner in the self-report test for their purpose. In follow-up studies, the Normal group should consist of various ages and backgrounds to be compared with the HSR groups.
Finally, the subjects of this study were patients who visited the psychiatric department of a university hospital for a psychological evaluation. Since the hospital is located in a specific geographic area and not all psychiatric visits involve psychological evaluation, the sample may not be representative of psychiatric visits for suicidal issues. Therefore, it is necessary to further research on diverse patients at medical institutions in various areas. Moreover, this study was conducted on the patients who visited the psychiatric department at the hospital and were diagnosed with a mental illness. While the diagnosis was statistically controlled as a covariate, the effect of temperaments and characters on suicide and self-injury might vary depending on the characteristics of their illness. Future studies should repeatedly examine the relationship between the temperaments and characters of patients with a specific disorder to suicide and self-injury.