INTRODUCTION
Patients with major affective and anxiety disorders frequently experience psychosocial impairment and multiple dysfunctions.123 Psychoactive medications together with other treatment options are commonly used to minimize, at least partially, these negative outcomes in major psychiatric conditions.
Given the detrimental consequences of these disabling conditions either at individual and social levels, researchers are encouraged to identify factors that may help to better predict illness trajectories as well as early management and adequate treatment.
Studies highlighted the involvement of sensory perception in emotional processes. It has been suggested that Sensory Processing Disorders (SPD) may be significantly involved in psychopathological processes and directly contribute to impaired daily functioning.45 The term ŌĆ£sensory intoleranceŌĆØ has been recently used in the current literature6 and is also recognized as SPD. SPD encompass difficulties in registering and modulating sensory information and organizing sensory input to perform successful adaptive responses to situational demands.78 Hyposensitivity may be expressed by either a pattern of low registration in which individuals fail to detect sensation and do not actively seek for sensory input, or sensation seeking in which individuals enjoy rich and intensive sensory environments and activities. Conversely, hypersensitivity, expressed in either a pattern of sensory sensitivity in which individuals feel discomfort with regular sensations but do not actively limit their exposure to them, or sensation avoidance in which people actively limit exposure to unpleasant sensations.9
Evidence also suggested the importance to identify the main predictors associated with a poor outcome in patients with anxiety and affective disorders. Longer duration of illness episodes have been associated with higher recurrences of the illness and chronicity1011 which are related, in turn, with higher social/functional impairments1213 as well as poorer response to treatment141516 when compared with less persistent illness episodes. Furthermore, a delay in initiating treatments has been suggested as one of the most relevant predictor of non-response to treatments and poor functional outcome.1718
Similarly, the severity of side effects has been reported as a predictor of poor treatment adherence negatively influencing the long-term outcome of patients with major affective disorders1920 and potentially enhancing treatment resistance as well as the neurobiological sequelae associated with the illness.21
However, although their influence on the outcome of patients with anxiety and affective disorders has been widely demonstrated, the relationship between SPD, duration of untreated illness and current illness episode together with severity of side effects related to psychoactive medications has not been systematically investigated.
Here, we aimed to investigate the association between SPD, duration of untreated illness and current illness episode as well as severity of medications side effects in a sample of psychiatric outpatients. Based on previous studies examining the impact of SPD and sensory over-responsivity in healthy young individuals,92223 adults22232425 and different populations of patients (e.g., children with disabilities or healthy individuals),26272829 we hypothesized that the longer duration of current illness episode and untreated illness together with the higher severity of medications side effects may correlate with specific SPD patterns.
METHODS
Sample
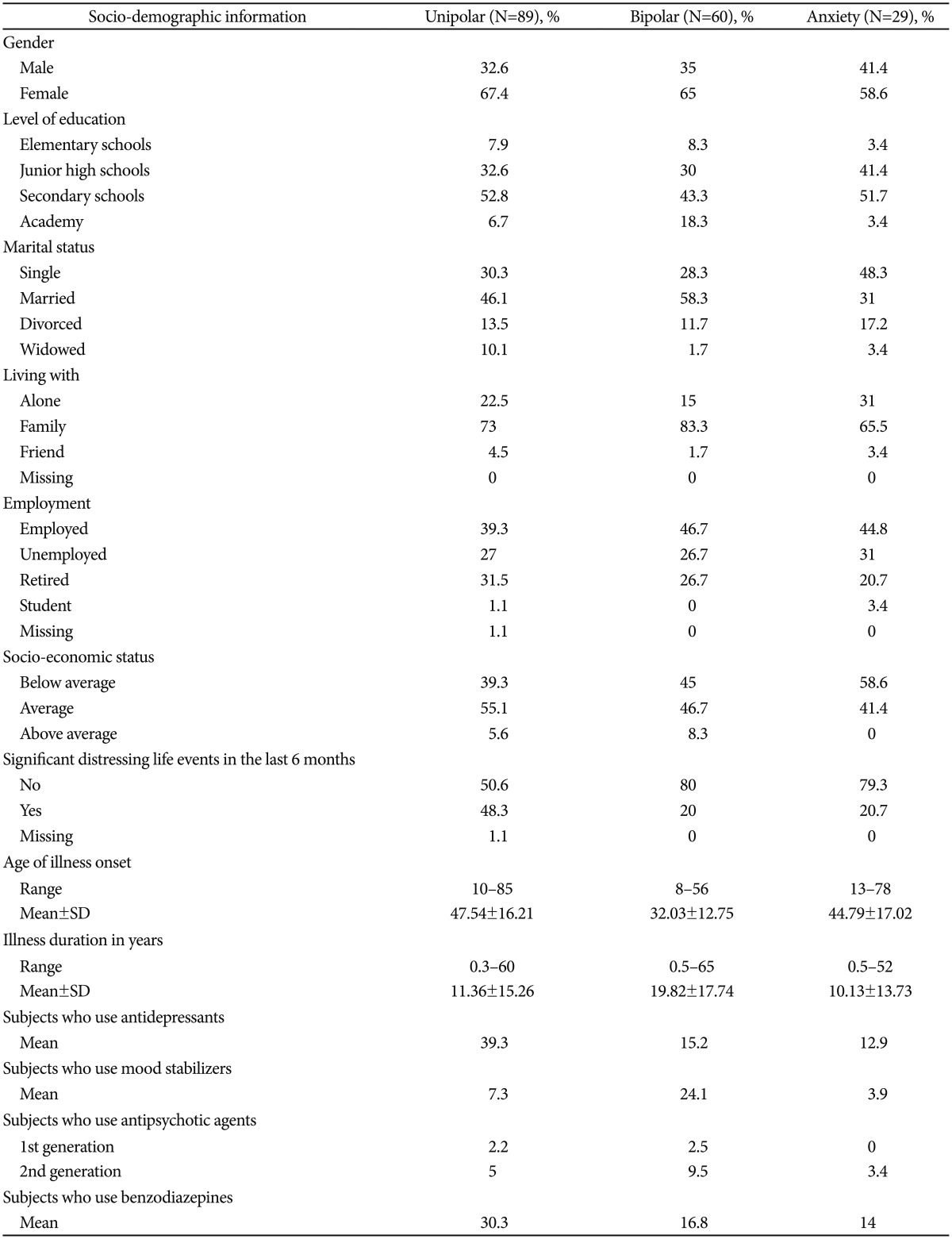
The sample included 178 participants with an age ranging from 17 to 85 years (mean=53.84┬▒15.55). Participants were distributed as follows: 50% of them were diagnosed with unipolar Major Depressive Disorder (MDD), 33.7% with Bipolar Disorder (BD) type I and type II, and 16.3% with Anxiety disorders (AD). All participants were consecutively admitted to the Department of Neuroscience (DINOGMI), University of Genoa, between July and December 2014. Psychiatric histories were carefully collected using all the available cross-sectional and retrospective information: medical records, information from the treatment team, and additional information from family or friends. All subjects were diagnosed using the Diagnostic and Statistical Manual of Mental Disorders criteria (DSM-IV, TR)30 and the Mini International Neuropsychiatric Interview (MINI).31 Exclusion criteria were any conditions affecting the ability to fill out the assessment, including delirium, dementia or any severe neurological diseases, and denial of the informed consent. Significant discrepancies between these sources served as further criteria for exclusion from the study. All the patients accepted voluntarily to participate in the study and gave regularly their informed consent. The study design was approved by the local ethical review board. Table 1 summarizes the most relevant participants' socio-demographic and health related information in each diagnostic group.
Measures
Demographic questionnaire. In this self-report questionnaire respondents answered questions about: health status, socio-demographic status, psychoactive and non-psychoactive medications.
The Adolescent/Adult Sensory Profile (AASP)32 is a self-measure psychometric tool with 60 items, sorted into four patterns reflecting Dunn's model.9 Participants indicate the frequency of their behavioural responses to sensory experiences in daily life on a five-point Likert scale. In the present study, the five ranges for each sensory processing pattern, as presented in the AASP manual were merged into: 1) ŌĆ£Less than most peopleŌĆØ [representing approximately 16% of the population, or more than one standard deviation (SD) below the mean]; 2) ŌĆ£Similar to most peopleŌĆØ (representing approximately 68% of the population between ŌłÆ1 SD and +1 SD); 3) ŌĆ£More than most peopleŌĆØ (representing approximately 16% of the population, or more than 1 SD above the mean). The AASP is currently under validation in Italian language.
The Udvalg for Kliniske Unders├Ėgelser (UKU) measured pharmacological treatment side effects and their severity.33 The severity and the perception or assessment that a symptom is a side effect was assessed as follows: 0=no, 1=mild, 2=moderate, 3=severe side effect. The UKU Scale is divided into four sections evaluating psychiatric symptoms (10 items), neurological symptoms (8 items), autonomic symptoms (11 items), and other effects (19 items), respectively.
Current episode duration/duration of untreated illness. Current episode duration has been measured by clinicians in days whereas duration of untreated illness has been retrospectively retraced in years based on the clinical history.
RESULTS
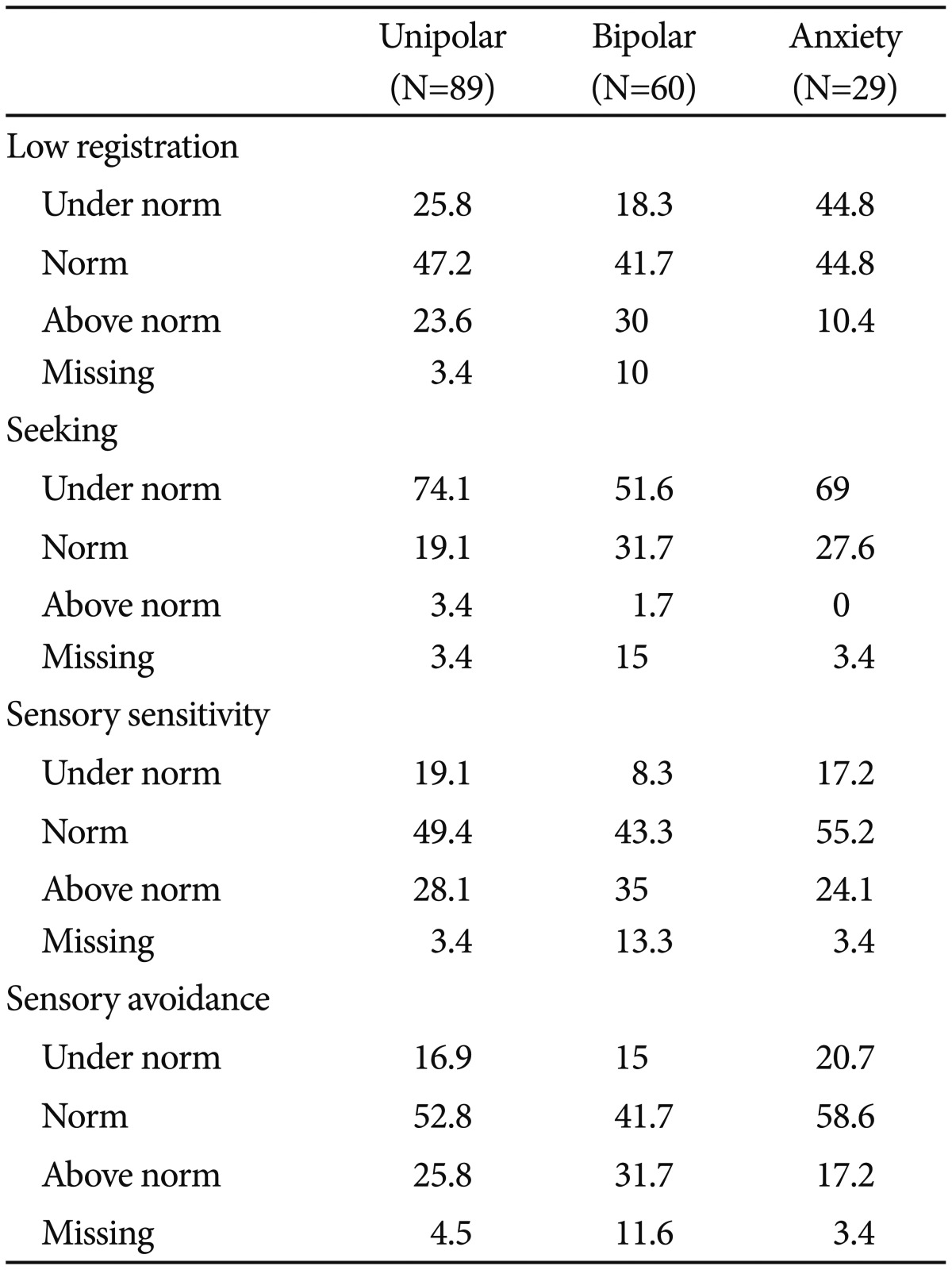
Frequency of SPD as presented by the percentage of participants in each sensory processing performance range for every diagnostic group
As presented in Table 2, low registration was found under norm (16% according to the AASP manual) almost 2-3 times more frequently among individuals with unipolar and anxiety disorders (25.8%, 44.8%, respectively).
Seeking was found under norm mostly among individuals with unipolar disorders (74.2%) although the percentage of individuals with bipolar and anxiety disorders in this interval was also relatively 3-4 higher than in the general population.
Greater sensitivity was found among individuals with bipolar disorders (35%), however the percentage of individuals with unipolar and anxiety disorders above the norms, was also relatively high (28.1%, 24.1% respectively). A similar trend (bipolar: 25.8%, unipolar: 31.7%, anxiety: 17.2%) was found in regard to sensation avoiding.
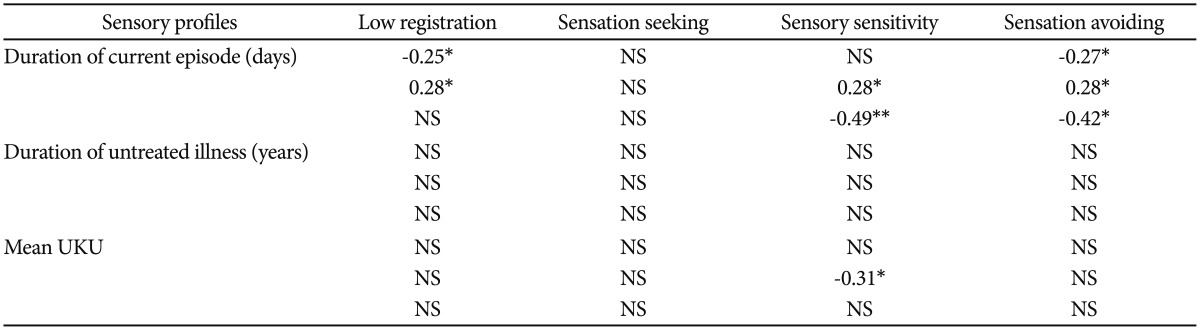
Correlations between SPD, duration of untreated illness, and duration of current episode
As presented in Table 3, among unipolar participants, longer duration of current episode (days) significantly correlated with greater registration of sensory input (r=-0.25; p=0.02) and lower avoidance from sensory input. Among bipolar participants, an opposite direction was found: longer duration of current episode (days) significantly correlated with lower registration of sensory input (r=0.28; p=0.04), greater tendency for sensory sensitivity (r=0.28; p=0.04) and sensation avoidance (r=0.28; p=0.03). Among participants with anxiety disorders, longer duration of current episode (days) significantly correlated with lower sensory sensitivity/avoidance (r=-0.49; p=0.01; r=-0.42; p=0.01, respectively).
DISCUSSION
This is the first study aimed to investigate the association between SPD, duration of untreated illness and current illness episode, as well as severity of medications side effects in a sample of psychiatric outpatients. The prevalence of SPD among patients with major affective and anxiety disorders was mainly expressed in elevated sensory sensitivity/avoidance, low registration, and lower tendency for sensation seeking. While an extremely higher percentage of individuals was reported in all three groups in regard to lower tendency for sensation seeking, these trends were much more prevalent (69%, 44.8%, respectively) among subjects with anxiety. This may be related to the greater sensitivity and avoidance of these patients. Similar results were found in the study of Engel-Yeger and Dunn23 on healthy adults in which sensory sensitivity/avoidance profiles but also lower registering were related to enhanced anxiety trait. The authors suggested that lower registrators tend to miss sensory stimuli but once they do notice, they are overwhelmed.
Unipolar patients showed similar SPD trends as patients with anxiety disorders. Bipolar patients showed the highest prevalence of subjects with sensation avoidance and sensitivity. Overall, this supports previous reports about the elevated vulnerability of patients with major affective and anxiety disorders to impaired modulation of sensory input34 but also suggests that the expression of SPD in specific affective conditions may be slightly different.
Hence, clinicians may use sensory profiles in order to better understand mechanisms involved throughout the course of psychiatric disease. For example, it is known that sensory hypersensitivity might be an unrecognized contributing factor for anxiety and may exaggerate emotional related outcomes such as negative emotionality35 and depression.36 This trend may be more problematic when combined with lower seeking and registration of sensory input. Indeed, these individuals may not actively seek for sensations in order to avoid them, as a coping mechanism. Reduced seeking and registration have been also related to depression, social isolation, impaired physical, cognitive and emotional status,37 impaired general health,38 and reduced participation in daily life activities.39 A better understanding of this fundamental topic could provide insights into whether the reported patient difficulties may reflect a specific emotional deficit or rather a generalized sensory processing problem.40
The above findings stress the need to refer to the SPD and their possible negative impacts on the individuals' daily life but also refer to the possible interaction between SPD and clinical characteristics. The importance to identify the main predictors associated with a poor outcome in patients with anxiety and affective disorders is well known. In this regard, one of the most interesting variable which has been repeatedly investigated was duration of current illness episode. We found that among bipolar patients, longer duration of episode correlated with lower registration and greater sensitivity/avoidance whereas we did not find any significant correlation between longer duration of untreated illness and SPD. An opposite trend was found among unipolar patients (where longer duration of episode correlated with greater registration and greater avoidance) and patients with anxiety with regard to greater sensitivity/avoidance.
Individuals with lower registration fail to detect sensation and do not actively seek for sensory input whereas individuals who actively limit exposure to sensations use strategies to avoid the unpleasant sensory experience and negative outcomes.9 SPD may predispose bipolar subjects to develop a variety of occasionally maladaptive coping strategies in order to balance the disequilibrium resulting from the inability to integrate information.41 Bipolar patients may be defined in our study as a more vulnerable subgroup of subjects who are more likely to exhibit maladaptive coping strategies and a poorer psychosocial adjustment/participation in daily life activities based on their SPD when compared with other groups.
Another interesting finding was that the severity of medication side effects (measured by mean UKU score) correlated with lower sensory sensitivity only among bipolar participants; therefore the higher is the UKU mean total score, the lower is the sensory sensitivity.
To our knowledge, there are no previous studies in the literature about the predictive potential of sensory patterns to distinguish between individuals with higher or lower perceived severity of side effects related to psychoactive treatments. According to our findings, patients with lower sensory sensitivity (bipolar subjects in this study) may be more likely to experience higher severity of side effects related to medications but it's important to note that these individuals may also present an increased likelihood of perceiving these side effects. Bipolar subjects also showed a higher prevalence of hypersensitivity (above 30% for sensitivity and avoidance). Hypersensitivity is known to be related to greater somatization, greater intensification of pain,22 hypervigilance, increased level of attention and arousal,42 all of which may significantly impact on the perceived severity of medications side effects. Side effects that significantly enhance functional limitations should be early recognized by clinicians in order to avoid significant distress. Also, the optimized selection of psychoactive medications which takes adequately into account the perceived subjective severity of medications side effects may directly impact on treatment adherence.4344 However, this is a complex issue that should be further investigated by prospective studies recruiting larger samples.
In summary, the results of the present study suggest that subjects with major affective and anxiety disorders commonly suffer from SPD that may be associated with specific clinical characteristics which are able to influence the perceived disability and long-term course of the illness. A better understanding of the impact of SPD on daily life of patients with major affective and anxiety disorder may contribute to research and practice related to these patients improving possible intervention benefits as well as quality of life.
Our results should be interpreted in the light of the following limitations. First, the number of participants was relatively low and the study may be underpowered. Thus, the results should be replicated in further larger samples. The cross-sectional study design with the observed associations do not represent causal relationships between the investigated parameters as well. Second, all patients have been selected as outpatients. In addition, given the great variability among participants, it would have been helpful to control for possible confounding socio-demographic variables. Unfortunately, we were not able to control for possible confounders such as age, socio-economic status, age of illness onset, and illness duration. Finally, the possible confounding effect of psychoactive medications (e.g., antidepressants, mood-stabilizers, antipsychotics, and benzodiazepines) was not analyzed. In this regard, it's also important to note that medications side effects should be considered as not specific, since all patients were taking multiple psychoactive medications. However, patients were all consecutive outpatients who had visited our hospital for at least 6 months and whose medication regimens had been stable for at least 6 months prior to recruitment. Moreover, psychoactive medications seem to not significantly affect sensory processing patterns who are supposed to be not state-related but rather stable patterns over the lifespan.45
In conclusion, this is, to our knowledge, the first preliminary study examining the association of SPD with clinical variables of patients with major affective and anxiety disorders and its impact on the long term course. Importantly, in addition to the frequent reports of hypersensitivity, we stressed the negative impact of hyposensitivity in subjects with major affective and anxiety disorders, in particular when related to lower registration, or alternatively the resilient role of SPD when referring to sensory seeking. According to our recent published studies,4647 the inclusion of measures of sensory processing patterns may provide relevant insights into the multiple determinants involved in the emergence/maintenance of major affective disorders.