INTRODUCTION
The aetiology of eating disorders is complex, with genetic, biological, psychological and sociocultural factors appearing to contribute significantly to their susceptibility.1,2 Although it is thought that eating disorders result from the interplay of these different factors, a comprehensive model of eating disorders remains to be established.
There have been a number of studies which examined the role of developmental factors in predicting the onset of eating disorders and their results were summarized in systematic reviews.3,4 The putative risk factors for eating disorders include diet vulnerability,5 less social support,6,7 high social anxiety,8 perfectionism,9 emotional eating10 or picky eating.11 It is unclear to what extent childhood risk factors contribute to eating disorders and what is their relative importance between anorexia nervosa (AN) and bulimia nervosa (BN). Pre-existing cognitive abnormalities may also be relevant to both the development12 and maintenance of eating disorders.13 Body image disturbance has been considered to be a key characteristic of patients with both AN and BN,14 the main neuropsychological component of which is a distorted body perception.15 A dysfunctional visuoperceptual ability may underpin distorted body perception in AN.16 Studies of patients with AN have reported impairments of visuospatial ability.17,18 The specific profile of visuospatial impairments of AN was in rapid visual information processing, whereas no impairments on tests of spatial span, pattern recognition memory, and spatial working memory.19 Not only have fewer studies of BN been conducted than of AN, but also their results were more subtle rather than invasive visuospatial cognitive difficulty.20 Furthermore, the detailed profile of visuospatial impairments and different patterns between AN and BN are uncertain. The stress diathesis model, in which additional environmental factors add to the risk of neuropsychological deficits with regard to obsessive-compulsive disorder,21 may explain the visuospatial deficits in the aetiological model of eating disorders.
We aimed at the development of coherent model of eating disorders including comprehensive childhood risk factors and visuospatial dysfunction. Thus the present study was designed to answer the following questions; To what extent do childhood risk factors contribute to eating disorders and what is their relative importance between AN and BN?: What are the detailed profiles of visuospatial impairment in AN and BN?: What is the comprehensive model consisting of both childhood risk factors and visuospatial deficit in AN and BN? The main hypothesis was that patients with AN and BN have certain risk factors in common and that both of them have an impairment of visuospatial ability, but that the pattern of impairment might differ. To test those hypotheses, we chose two neuropsychological tests, the Rey-Osterrieth Complex Figure Test22 and the Group Embedded Figures Test23 which were used for measuring the detailed profiles of visuospatial ability in previous studies.24 We performed a retrospective assessment of various eating disorder-specific-childhood risk factors compiled from an extensive review of the literature made by one of the researchers (J.T.).25
METHODS
Study population
A total of 76 participants, including 22 women with AN and 28 women with BN as well as 26 healthy women, were recruited. The diagnoses of eating-disorder patients were as per the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) criteria using the Korean version of the Structured Clinical Interview for DSM-IV Axis I disorders (SCID).26 Among the AN patients, 15 (68%) had the restrictive subtype and 7 (32%) the purging subtype. Seven (25%) BN patients had a history of AN, whereas none of the AN patients had a history of BN. The controls' exclusion criteria were the past or current clinically significant eating disorder symptoms and any current psychiatric disorders. The exclusion criteria for all participants were histories of neurologic illness, brain injury, substance-abuse disorder, or psychosis. We permitted only the use of selective serotonin reuptake inhibitors (SSRIs) within 2 weeks before the neuropsychological test, as evidence suggests antidepressant medication has a relatively negligible effect on the cognitive profile.27 Eight (36%) with AN and 16 (57%) with BN were taking SSRIs at the time of the study. This study was approved by the Institutional Review Board of Seoul Paik Hospital in Seoul, Korea. We obtained written informed consent from all of the participants.
Procedure
We matched the groups in terms of general intelligence ability and years of education, administering the Korean version of the Wechsler Adult Intelligent Scale28 to them to ascertain the former. We measured participants' depression, anxiety, and obsessionality levels via Korean versions of the Beck Depression Inventory,29 the Spielberger State and Trait Anxiety Inventory,30 and the Maudsley Obsessive Compulsive Inventory,31 respectively. The patients underwent interviews using the Korean version of the 12th edition of the Eating Disorders Examination (EDE)32 to measure their objective eating-disorder symptoms.
Measures
Childhood risk factors questionnaire
The questionnaire focused on the period before onset of eating disorders to ensure that the exposure preceded the development of the eating disorder. The questionnaire comprised 36 questions, divided into 8 domains which covered (i) Parents or adults concern about thinness (ii) Parents or adults teasing about weight or shape (iii) Social support (iv) Anxiety (v) Perfectionism (vi) Emotional overeating (vii) Emotional undereating (viii) Picky eating. The psychometric properties of the Korean version was assessed with 2 week test-retest reliability for the 8 factors ranging between 0.64 and 0.87, and Cronbach's alpha coefficient ranging between 0.70 and 0.91.
Group Embedded Figures Test
We applied the group version of the EFT33 to subjects individually. As no working memory is required in the Group Embedded Figures Test (GEFT),23 the test is a good perceptual measure for exploring analytical ability in a low-level visuospatial processing modality. The GEFT procedure called for participants to mark the hidden target shapes that were embedded within more complex stimulus patterns, as many times as appropriate. Each participant could check the simple figure against the complex design throughout the whole task. The score was the number of shapes participants correctly located during the given time. The Korean version contains 5 simple geometric forms and allows a maximum of 10 minutes for completing each of the two sections, with 18 complex designs per section. Scores ranged from 0-18 correctly-located shapes per section. According to Korean normative data, the test/retest reliability coefficient of the Korean version of the GEFT was 0.67, and Cronbach's alpha was 0.82.34
Rey-Osterrieth Complex Figure Test
The Rey-Osterrieth Complex Figure Test22 is an open-ended measure of visuospatial constructional ability and visual memory.35 In the first stage of this testing procedure, the participants saw a figure and copied it, without knowing that they would be asked to remember it. The second stage, free-recall test took place after 30 minutes (the delayed condition). We used the system Meyer and Meyer36 developed to calculate the score for each condition, evaluating 18 segments of the figures using criteria such as location and accuracy. There were two criteria for each segment, each worth 1 point, resulting in a score range of 0-36.
Statistical analyses
The three groups (AN, BN, controls) were compared in terms of their clinical variables using analysis of variance and t-tests, as appropriate for the measurements. Multinomial logistic regression with the independent variables consisting of the childhood risk factors, RCFT and GEFT was used to identify those factors which have an impact on the group membership, with the controls used as a reference group. We used multivariate logistic regression analyses using the forward variable selection strategy on the putative factors, in order to find those factors independently contributing to the case status. Two-tailed tests with a 5% level of significance were used throughout the analyses.
RESULTS
Demographic and clinical characteristics
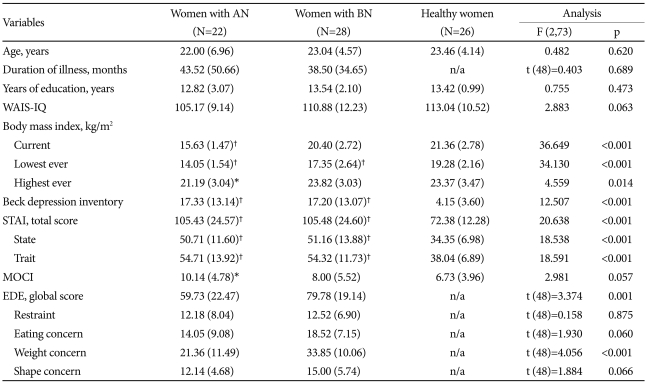
Table 1 shows the participants' clinical and demographic characteristics. The AN group had a lower lifetime weight history, whereas the BN group had a more fluctuating lifetime weight history. Both the AN and BN groups had higher scores for depressed mood and for state and trait anxiety than did the nonclinical group. They showed a tendency toward higher obsessive-compulsiveness, but the difference was statistically minimal (the post-hoc Tukey test; p=0.046 for AN vs. controls: p=0.061 for BN vs. controls). The BN group had higher EDE scores than the AN group did, particularly in the subscale of weight concern.
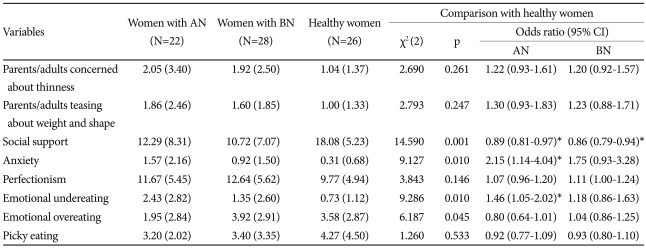
Childhood risk factors
As shown in Table 2, both the AN and BN patients were less likely to report social support (p=0.008 for AN vs. controls: p=0.001 for BN vs. controls). The AN patients were more likely to report childhood emotional undereating (p=0.023) and premorbid anxiety (p=0.018).
Visuospatial ability
Table 3 shows the results of the neuropsychological tests. On GEFT, the AN group showed poor ability to identify correct shapes during the given time as compared to the healthy controls (p=0.015). On RCFT, both patient groups showed poorer copy accuracy than the healthy controls did; this finding was less prominent in the AN group (p=0.049 for AN vs. controls; p=0.036 for BN vs. controls). The difference in recall accuracy between the patients and the controls did not reach statistical significance. In a subsidiary analysis to investigate the influence of medication state on performance, comparisons between the eating disorder patients who were and were not currently receiving antidepressants revealed no significant group differences across the neuropsychological tasks (t=1.145, df=48, p=0.258 for GEFT: t=0.010, df=48, p=0.992 for copy accuracy on RCFT).
Independent contribution of identified factors to case status in final model
The identified neuropsychological variables and childhood risk factors obtained from the univariate analyses were entered into the regression model analyses (Table 4). The childhood risk factors were entered first, followed by the neuropsychological variables. Childhood emotional undereating (p=0.011), less social support (p=0.009) and poor performance in the GEFT (p=0.029) contributed independently to the case status of AN. The factor independently contributing to BN case status was less social support in childhood (p=0.002).
DISCUSSION
This study furthers our understanding of the aetiological model of eating disorders. In our study, the AN patients were more likely to report childhood emotional undereating and performed poorly on GEFT. Both the AN and BN patients were more likely to report lower social support, which factors appear to contribute to an increase in vulnerability to eating disorders case status.
Emotional eating involves integrated emotional regulation, reward processing, and interoception. In our retrospective study, childhood emotional undereating strongly contributed to AN case status, which supports the idea of a trait-related dysfunction in the brain appetite circuit in AN, as proposed by Kaye et al.37 Whereas carbohydrate intake reduces anxiety by increasing extracellular serotonin concentration in the brain in a healthy human,38,39 it can stimulate dysphoric mood in AN people.40 Whereas childhood social support was an independent risk factor of eating disorder case status, it is interesting that our model did not include the factors related to diet vulnerability. Their role may be that of a trigger in the onset of eating disorders.41
In the neuropsychological data, our findings are consistent with previous studies of poorer performance on GEFT in AN,42 which contradict the results of Lopez et al.24 This discrepancy may be attributable to the differences in sample chronicity between theirs and ours (duration of illness: 13.08±11.2 years vs. 3.63±4.2 years, respectively) and methodology details (EFT vs. the group version of EFT, respectively). Those severely impaired AN patients may have a different cognitive impairment pattern from other AN patients.45 Thus, the results of Lopez et al.24 may more properly explain treatment-resistant, chronic AN cases. In addition, the AN group might have felt the pressure of the time limitation of the group version than the non-clinical group did, which could lead to their poor performance in the test. Our results on RCFT in BN is generally consistent with previous studies in respect to poorer accuracy on the copy phase46 and no visuospatial memory impairments.45,47 It appears that the visuospatial dysfunction in eating disorder were subtle, but overall our findings suggest dysfunctions in low-level visuospatial processing in AN case status. Our results could be explained based on the stress diathesis model, in which the lower social support may add to the risk of the dysfunction of low-level of visuoperceptual processing.
However, the present study contained a few limitations, which need to be considered. The first is the retrospective assessment of the risk factors. Although we carefully assessed the risk factors with a focus on the period of childhood before the onset of the patients' disorders, to ensure that the period of risk factor exposure preceded the eating disorder's development, such soft judgments as over-concern and expectations may be biased by retrospective recall or affected by the patient's current state. Second, we might not have included all of the risk factors relevant to a more comprehensive neurodevelopmental hypothesis, i.e., perinatal events. Third, we could not use more comprehensive tasks as measures of visuospatial ability. Fourth, the sample size was relatively small.
In conclusion, these findings add to the growing body of evidence for a complex etiological model of eating disorders. Our results suggest that the disturbance in the food-emotion relationship and the deficit in low-level visuospatial processing in people with AN. Lower social support appears to contribute to an increase in vulnerability to both AN and BN.