Systematic Review of the Neural Effect of Electroconvulsive Therapy in Patients with Schizophrenia: Hippocampus and Insula as the Key Regions of Modulation
Article information

Abstract
Objective
Electroconvulsive therapy (ECT) has been the most potent treatment option for treatment-resistant schizophrenia (TRS). However, the underlying neural mechanisms of ECT in schizophrenia remain largely unclear. This paper examines studies that investigated structural and functional changes after ECT in patients with schizophrenia.
Methods
We carried out a systematic review with following terms: ‘ECT’, ‘schizophrenia’, and the terms of various neuroimaging modalities.
Results
Among the 325 records available from the initial search in May 2020, 17 studies were included. Cerebral blood flow in the frontal, temporal, and striatal structures was shown to be modulated (n=3), although the results were divergent. Magnetic resonance spectroscopy (MRS) studies suggested that the ratio of N-acetyl-aspartate/creatinine was increased in the left prefrontal cortex (PFC; n=2) and left thalamus (n=1). The hippocampus and insula (n=6, respectively) were the most common regions of structural/functional modulation, which also showed symptom associations. Functional connectivity of the default mode network (DMN; n=5), PFC (n=4), and thalamostriatal system (n=2) were also commonly modulated.
Conclusion
Despite proven effectiveness, there has been a dearth of studies investigating the neurobiological mechanisms underlying ECT. There is preliminary evidence of structural and functional modulation of the hippocampus and insula, functional changes in the DMN, PFC, and thalamostriatal system after ECT in patients with schizophrenia. We discuss the rationale and implications of these findings and the potential mechanism of action of ECT. More studies evaluating the mechanisms of ECT are needed, which could provide a unique window into what leads to treatment response in the otherwise refractory TRS population.
INTRODUCTION
Schizophrenia affects approximately 1% of global population, with more than 21 million patients worldwide [1]. Treatment- resistant schizophrenia (TRS) is defined as the absence of a response after two different antipsychotics at an adequate dosage and duration. Twenty to 50% of patients with schizophrenia are considered treatment-resistant [2-4], and, not surprisingly, treatment-resistance results in an additional socioeconomic burden that is approximately 3 to 11 times greater than the burden experienced by patients with schizophrenia who remain in remission [5]. The treatment of choice for these patients is to introduce the medication clozapine [2,4,6], but 40% to 70% of treatment-resistant patients will not respond to clozapine [7], leaving 14% to 20% of all patients with schizophrenia to be treatment refractory without better treatment options [5].
Electroconvulsive therapy (ECT) was first introduced to treat schizophrenia before antipsychotic medication was available [8]. After the late 1950s, with the advent of antipsychotic agents, the use of ECT in schizophrenia declined worldwide [9], with its primary indication being catatonia, psychotic depression, suicidality, and drug intolerability [10]. Although its main pattern of use somewhat differs among countries (according to a systematic review in 2011, in United States, Europe and Australia, 8–29% of patients receiving ECT were patients with schizophrenia, while in Asia and Africa it was 60–83%),9,11,12 ECT is currently most commonly used for patients with treatment- resistant depression [11], where its efficacy is robust and superior compared to the standard combination of antidepressants [13,14]. TRS is another clinical group in which ECT is commonly used to augment standard antipsychotic treatment [10,15]. A large volume of clinical research literature and systematic reviews along with an increasing number of treatment guidelines support the addition of ECT to antipsychotic agent regimens [15-23], including a recent review from the Cochrane systematic reviews [24]. Considering the prevalence and rather striking socioeconomic consequences of TRS, clinicians have argued that ECT should not be used as the ‘last resort’ and that it should be increasingly applied to patients with schizophrenia [9,25].
Despite this context of robust effectiveness, the underlying mechanism of action of ECT has largely remained elusive. Historically, the generalized seizure hypothesis, changes in neurotransmitters and neuroendocrine function hypothesis, and the neurotrophic hypothesis has been postulated as working models of ECT [26]. Recent studies examining depressive patients have consistently found increased bilateral hippocampal volumes by ECT [27-31], providing support for the neurotrophic hypothesis, but correlations between volumetric changes and clinical improvements were found to be repeatedly inconclusive, leaving out the main ‘key’ factor regarding the long unanswered question of ECT’s clinical effectiveness. Furthermore, the factors leading to clinical improvement after ECT in schizophrenia patients are cryptic, with only a small number of studies and divergent findings. This is indicative of a largely underrepresented current state of research for a disease with such great burden and the tantalizing problems of obstinacy. Identification and delineation of the common and disease-specific effects of ECT can serve to provide insights into the currently ‘untreatable’ TRS population, which constitutes a major problem in the modern practice of psychiatry. Thus, we aimed to systematically review the current status of research investigating the effects of ECT in schizophrenia patients using, utilizing etc. various neuroimaging modalities.
METHODS
PubMed, EMBASE, and the Cochrane Reviews were searched for publications with the following keywords: ‘ECT’, ‘schizophrenia’, and the terms of various neuroimaging modalities. Studies available based on the search by May 1, 2020, were included. We intended to include articles that examined patients with schizophrenia undergoing ECT sessions and implemented at least one neuroimaging modality according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Statement. Articles published before the 1990s were excluded owing to two reasons: 1) to minimize the heterogeneity among study methods, and because 2) earlier studies tended to focus on deleterious side effects of ECT [32-34]. While ECT can bring about selective cognitive side effects such as acute delirium or impairments in autobiographic memory, it is nowadays widely agreed that ECT does not cause other severe long-lasting side effects such as brain damage or dementia [35]. Detailed descriptions of the methods are provided in the supplementary methods in the supplementary material.
RESULTS
Study selection and characteristics
During the initial search, 325 articles were found, and after removing 3 duplicates, 322 articles were screened. A total of 305 records that unmet the inclusion criteria were excluded after abstract screening (PRISMA flowchart, Figure 1).

Flowchart of the literature review process. *Three studies studied both structural and functional MRI changes after ECT, and thus was included in both structural and functional MRI categories. ECT: electroconvulsive therapy, MRI: magnetic resonance imaging, MRS: magnetic resonance spectroscopy, PET: positron emission tomography, SPECT: single positron emission computer tomography, NIRS: near-infrared spectroscopy.
A total of 17 studies were selected and considered eligible for inclusion in the current review. Three of the studies explored the role of ECT in changes in cerebral blood flow (CBF), 3 studies used magnetic resonance spectroscopy (MRS) to measure changes in brain metabolites, and 11 studies used magnetic resonance imaging (MRI) as the study modality (6 structural and 8 functional studies, with 3 using both modalities). Detailed information about each study eligible for inclusion in the review is provided in Supplementary Results and Supplementary Table 1 in the Supplementary Materials (in the online-only Data Supplement).
Effect of ECT on cerebral blood flow
Three studies measured changes in CBF using differing study modalities, namely, of positron emission tomography (PET), single-photon emission computed tomography (SPECT), and near-infrared spectroscopy (NIRS) (Table 1).

Cerebral blood flow in patients with schizophrenia receiving electroconvulsive therapy (ECT)
A PET study reported decreased CBF in the bilateral frontal lobes, right temporal lobe, and right putamen after ECT (n=5) compared to controls (n=6) [36]. In another study, CBF in the right parietal and bilateral temporal lobes measured using SPECT was increased in patients with schizophrenia (n=5) compared with MDD patients (n=5) [37]. A NIRS study revealed an increased blood flow ratio of the left prefrontal cortex (PFC) to right PFC in patients with schizophrenia (n=11) after ECT, an asymmetry that was not observed in the MDD (n=10) group [38].
Effect of ECT on brain metabolites
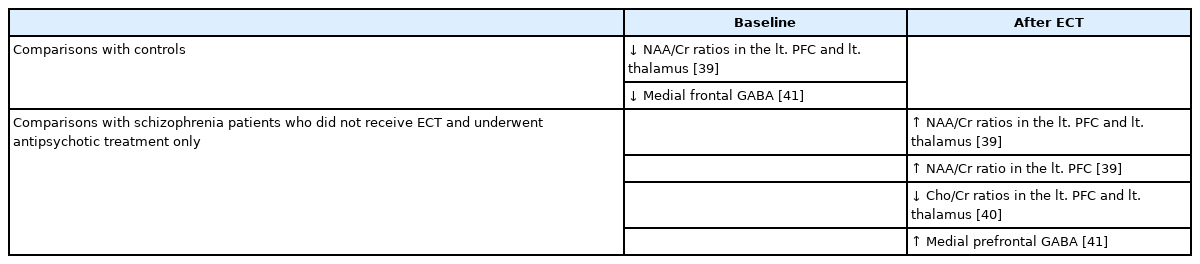
Three studies examined the changes in brain metabolites using MRS (Table 2). Two independent studies (n=34 and n= 10) revealed changes of N-acetyl-aspartate/creatinine (NAA/ Cr) ratio in the left PFC and the left thalamus [39,40]. Another study showed an increase in medial prefrontal γ-aminobutyric acid (GABA) levels (n=14) [41].
Brain metabolites measured by magnetic resonance spectroscopy in patients with schizophrenia receiving electroconvulsive therapy (ECT)
Effect of ECT on brain structures
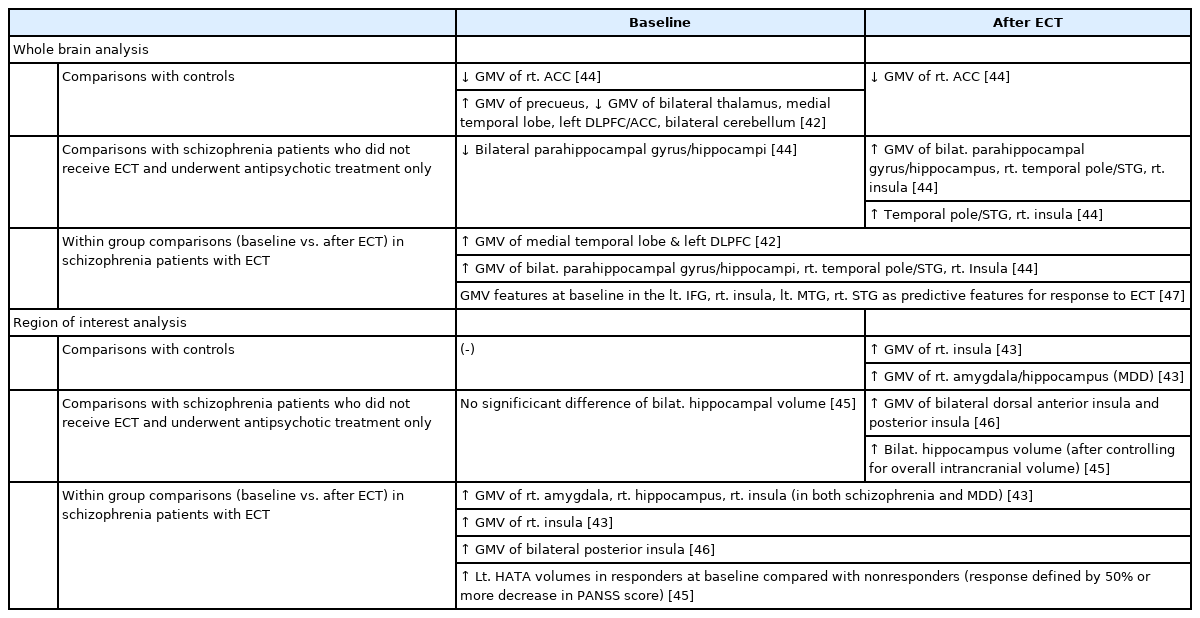
Six studies investigated structural changes after ECT in patients with schizophrenia. Table 3 demonstrates the findings of each study according to the method of analysis [wholebrain analysis or region-of-interest (ROI) analysis]. Notably, three datasets from three different study groups were analyzed, and using different and complementary analysis methods, a total of six publications were included. This relatively small number of studies may be partially attributed to the relatively restricted use of ECT in some parts of the world [11], with varying treatment guidelines across nations, and a series of index ECT treatments require approximately one month to perform, which raises the issue of accessibility.
Regional volumes measured by structural magnetic resonance imaging in patients with schizophrenia receiving ECT
One group compared the effects of ECT on patients with schizophrenia (n=9) and MDD (n=12) [42,43]. Based on the results of the whole-brain analysis, the authors found that the gray matter volume (GMV) in the medial temporal lobe (MTL) network and the left dorsolateral prefrontal cortex (DLPFC) increased in patients with schizophrenia after ECT [42]. An additional complementary analysis of the temporal regions revealed that increases in volumes of the hippocampus and insula were shared by patients with schizophrenia and MDD, but were restricted to the right side [43]. The post hoc withingroup analyses only revealed increased GMV in the right insula in the schizophrenia group.
Another group examined the effects of ECT on patients with schizophrenia (i.e., ECT+antipsychotic medication; n=21) compared with schizophrenia patients who did not receive ECT and underwent antipsychotic treatment only (n=21) [44-46]. Whole-brain analyses showed increased GMVs in the bilateral parahippocampal gyri/hippocampi, right temporal pole/right superior temporal gyrus (STG), and right insula after ECT compared to baseline and the antipsychotics only group [44]. Additional ROI analyses of the insula and hippocampus indicated increased GMVs in the bilateral dorsal anterior insula and posterior insula [46] and bilaterally increased hippocampal volumes [45]. An analysis stratified according to response status to ECT further showed that higher baseline volumes in the left hippocampus-amygdala transition area (HATA) were observed in responders [45].
A separate study group reported that baseline GMVs in the temporal region, including the right insula, left middle temporal gyrus (MTG), and the right STG, along with the left inferior frontal gyrus (IFG), predicted ECT response [47].
While the specific findings differed among studies, reviewed results overlap in findings of increased GMVs in the hippocampus (whole-brain analysis, n=2; ROI analysis, n=2) and the right insula (whole-brain analyses, n=2; ROI analysis, n=2).
Effect of ECT on functional connectivity
Eight studies from four different groups examined restingstate functional connectivity (rsFC) after ECT. Table 4 demonstrates the findings of each study according to the method of analysis (whole-brain analysis or ROI analysis). Findings common to these studies were changes in the rsFC of the default mode network (DMN), PFC, thalamus, hippocampus, and insula.

Functional connectivity measured by functional magnetic resonance imaging in patients with schizophrenia receiving ECT
The first study group, which included schizophrenia (n=9) and MDD (n=12) patients, performed a whole-brain analysis and observed increased rsFC of the medial prefrontal cortex (mPFC) within the DMN, between the executive network and the DMN, and between the executive network and salience network, along with decreased low-frequency oscillations in the striatal networks in patients with schizophrenia after ECT [48]. ROI analyses of the amygdala to other brain regions showed decreased rsFC between the right amygdala and various regions, including the mPFC, insula, and DLPFC [43].
The second study group compared patients with schizophrenia treated with either ECT (n=21) or antipsychotics alone (n=21). Whole-brain analyses showed increased connectivity of the ventral medial prefrontal cortex (vmPFC) and dorsal medial prefrontal cortex (dmPFC) after ECT compared with the antipsychotics only group and controls [49]. This group performed ROI analyses of the insular subfields [46], hippocampus [45], and thalamic subfields [50]. While significant changes in various regions were found, responders to ECT exhibited increased rsFC of the hippocampus to the PFC and the hippocampus to the DMN [45], and between the thalamus and regions of the temporal lobe and the cerebellum [50].
The third group simulated electrical fields of ECT stimulation to select regions with large electrical fields, and compared the changes in those regions before and after ECT (n=47) [51]. After ECT, rsFC between the right amygdala and left hippocampus was increased compared to baseline.
The fourth group observed altered rsFC within various networks, including the DMN and temporal lobe networks, in the ECT group compared with antipsychotics only group [52].
The results from the aforementioned studies suggest rsFC of the DMN and associated regions (n=5), PFC (n=4), thalamus (n=2), hippocampus (n=2) and insula (n=2) were commonly altered after ECT.
Associations with clinical improvement and ECT response status
Findings of significant associations with clinical improvement and the status of the ECT response are listed in Supplementary Tables 2 and 3 (in the online-only Data Supplement), respectively. Four studies reported associations of clinical improvement with changes in the hippocampus [44,45,51,52], two studies with changes in the insula [46,47], and one study with changes in the amygdalar region, respectively [51].
DISCUSSION
This is the first systematic review to examine neural effects of ECT in patients with schizophrenia. A standardized literature search yielded 17 studies. The majority of recent studies (n=11) used MRI as the study modality, which examined morphometric (n=6) and functional (n=8) changes before and after ECT. An additional six studies investigated the effect of ECT on CBF (n=3) and brain metabolites (n=3). Overall, the reviewed publications considerably differed in both study designs and modalities, which precluded performing a metaanalysis.
Cerebral blood flow changes after ECT
Two studies compared changes in blood flow after ECT in patients with schizophrenia and patients with MDD and observed increased blood flow in patients with schizophrenia using SPECT and NIRS, respectively [37,38]. Notably, studies of patients with MDD quite frequently report decreased blood flow in various regions following ECT sessions [53]. Two other studies compared the data obtained from patients with schizophrenia before and after ECT, and one study did not report significant alterations (SPECT) [37], while the other reported decreased blood flow after ECT (PET) [36]. Due to the small numbers and discrepancies in study modalities and findings, a solid conclusion concerning changes in blood flow after ECT is difficult to obtain.
Changes in brain metabolites after ECT
Other studies examined changes in brain metabolites using MRS; interestingly, two studies reported increased NAA/Cr ratios in the left PFC and the left thalamus. The NAA/Cr ratio is considered an indicator of neuronal integrity [54,55], which is known to decrease in conditions such as aging, brain tumors, and acute pathological processes [56], and these decreases are known to be reversible with treatment [55]. Previous meta-analyses provided consistent evidence of decreased NAA/Cr ratios in the hippocampus, thalamus, frontal and temporal lobes of patients with schizophrenia [57], which, interestingly, were increased after antipsychotic treatment [58,59]. Although these findings must be replicated in the future due to the small number of studies that utilized MRS, the increase in NAA/Cr ratios in the left PFC and the left thalamus, regions that are strongly implicated in the pathophysiological hypothesis of schizophrenia [60-63], may imply therapeutic neuronal ‘reorganization’ by ECT. These results from MRS, since they contain properproperties of both structure and function, might serve integrative functions in explaining the effects of ECT when results from MRI studies are combined along with the proposed pathophysiological models of schizophrenia. Future studies examining NAA, GABA, and glutamate or glutamine in the regions highly implicated in schizophrenia and ECT (such as the frontal and temporal lobes, the hippocampus, and thalamostriatal regions), may help to further our understanding of the mechanism of action of ECT.
Structural and functional changes after ECT
Only four study groups independently examined the neural effects of ECT on patients with schizophrenia. Although fewer studies of patients with schizophrenia have been reported than studies of patients with depression, the results quite consistently indicate increases in the volumes of the hippocampus (structural, n=4) and insula (structural, n=4). Additionally, a comparison of patients with schizophrenia and MDD revealed common increases in the GMVs of the hippocampus, while the increases in right insular GMV were restricted to patients with schizophrenia [43]. FC studies presented more divergent results for different ROIs, while commonly identified alterations were located within the regions of the DMN (functional, n=5), PFC (n=4), thalamostriatal system (n=2), hippocampus (n=2), and insula (n=2). Moreover, among the features that were associated with symptom reductions were the hippocampus (n=4), insula (n=2), and amygdala (n=1).
From the integrated findings of both structural and functional measures, we infer, albeit preliminarily, that the hippocampus (total, n=6; symptom associations, n=4) and insula (total, n=6; symptom associations, n=2) are the common regions of modulation in patients with schizophrenia after ECT.
Insula
The insula is located deep within the lateral sulcus of the human brain. The upper cortices that cover the insula are called the operculum, which are composed of parts of the adjacent frontal, temporal, and parietal cortices. The insula is involved in various functions, such as interoception, multimodal sensory processing [64], self-related processes [65-68], taste [69], social emotions [70-73], homeostasis [74,75] and auditory perception [76-78]. This whole spectrum of functions can be served owing to the extensive viscerosensory inputs into the region and its anatomical position amidst three different cerebral lobes permitting dense reciprocal connections with the limbic, prefrontal, somatosensory, and temporal areas [79,80].
The results from the current systematic review revealed increased GMVs in the right insula in all of the structural MRI studies that performed whole-brain analysis. While conclusion should not be drawn solely based on this result, the underlying implication of insular involvement in patients with schizophrenia suggests that the insula has some unique characteristics worth further discussion.
First, the insula is one of the most consistent regions showing structural alterations in patients with schizophrenia. An anecdotal meta-analysis that included studies performing wholebrain analyses showed that approximately 50% and 40% of studies (which ranks as 7th and 10th, respectively among all regions of interest) reported reduced volumes of left and right insular areas, respectively [81]. Indeed, structural alterations of the insula are considered the most consistent findings in psychosis subjects [82]. In a meta-analysis performed by Crow et al. [82], the insula was the most commonly reported area showing volumetric reduction, followed by the thalamus and anterior cingulate cortex. Additionally, in terms of numbers, right insula was the most commonly reported altered area, while in terms of the size of volumetric reductions, left insular defects were more profound in patients with schizophrenia [82].
Second, recent studies have demonstrated insular involvement in auditory sensory processing. Intracranial electroencephalography recordings found auditory responses of the posterior insula resembling the response in Heschl’s gyrus [77], and a separate study implicated insular involvement in auditory deviance detection and the formation of mismatch negativity [78]. Abnormal sensory gating and altered auditory evoked potentials are one of the key pathophysiological findings explaining the phenomena of hallucinations in schizophrenia patients [83]. Since clinical observations have suggested that ECT is more effective in refractory positive symptoms than in negative domains [15], amelioration of clinical symptoms after ECT might be mediated in part by modulation of the insular cortex.
Third, although its implications in schizophrenia remain unclear, lateralized functions of the insula appear to be related to the control of the autonomic nervous system. Various studies ranging from intraoperative intracranial electrical stimulation to lesion studies have shown that the right insula is involved in the top-down control of sympathetic tone [75,84-86]. While the findings have been somewhat inconsistent, various types of autonomic dysfunction, such as alterations in heart rate variability (HRV) [87,88] and decreased vagal tone [89,90], have been reported in patients with schizophrenia. Autonomic responses and control during stressful situations constitute an important axis in the stress diathesis model of psychiatric illness [91-93], and insular modulation by ECT may exert some effects on the central control of sympathetic nervous system tone.
Finally, the self-related functions of insula share striking commonalities in terms of the main psychopathology of delusions and hallucinations in patients with schizophrenia. Among the wide range of insular dysfunctions demonstrated in patients with schizophrenia [94-100], some studies have reportreported a relationship between decreased right insular volumes and delusion severity [94] or degree of insight [97]. Delusion and hallucination are considered externalizing psychopathologies, which suggest impairment in the insular functions of interoception and self-attribution in patients with schizophrenia.
Hippocampus
The modulation of the hippocampus and its neurotrophic functions by ECT are very strongly supported by findings from animal models of electroconvulsive seizure (ECS) and patients with MDD. The increase in the hippocampal volume observed in patients with depression after ECT are not only a robust finding but also explains many aspects of depression, including its treatment and etiology. Concerning treatment, ECT is considered the most effective treatment modality in depression, including treatment-resistant cases [13,14]. Approximately 50% to 60% of treatment-resistant depression patients will respond to ECT [13], and its efficacy is deemed to be five- to six-fold greater than antidepressant therapy. In addition, the chronic stress model of depression is closely associated with dysfunction of the hypothalamic-pituitary-adrenal (HPA) axis [101], as both early life and chronic stress are known to increase levels of the stress hormone cortisol and alter the functions of the HPA axis [102]. Stress and HPA axis dysfunction are known to exert deleterious effect on hippocampus, including cell loss and volume reductions [103,104].
Meanwhile, most researchers appreciate that schizophrenia is a ‘dysconnection’ syndrome among large distributed brain networks [105,106], rather than problem of a single faulty region. Notwithstanding, hippocampal hyperactivity is among the most consistent functional abnormalities observed in patients with schizophrenia [107-109]. Postmortem studies have replicated reduced hippocampal volumes [110-112], which are also consistent with the current body of neuroimaging studies in patients with schizophrenia [113-116]. In addition, while the number of neurons in the hippocampus is not significantly altered, reduction in inhibitory interneuron population of the hippocampus was demonstrated [107,108,117]. Studies measuring blood flow and metabolism also replicated abnormalities in the hippocampus, and subsequent studies have found that these metabolic shifts are associated with a greater reduction in hippocampal volume with disease progression [109]. Additionally, neuroimaging and animal studies have consistently reported reductions in the volumes of hippocampal subfields, with CA1 subfield showing the most robust changes [118,119].
The dopamine hypothesis of schizophrenia was born based on the clinical effectiveness of antipsychotic agent chlorpromazine [120-122]. The modern mainstream pathophysiological hypothesis of schizophrenia focuses on abnormality of the glutamate system and impairment in interneuron functions [123-125]. Hippocampal hyperactivity can be explained by both the dopamine and glutamate hypotheses. First, while optimal levels of dopamine can enhance memory and functions subserved by the hippocampus, higher levels of dopamine were demonstrated to exert deleterious effects [112,126,127]. Neuronal connections between the ventral hippocampus and striatum are bidirectional and capable of modulating dopamine levels in the other structure [126,128,129]. This means that the dysfunctionally increased dopamine levels in the striatum can induce high dopamine levels in hippocampal areas, and vice versa, which could lead to hippocampal hyperactivity. Second, the hippocampus is among one of the most implicated areas concerning the glutamate hypothesis, which includes NMDA receptor hypofunction and reduced inhibitory interneuron function [107]. These interneuron abnormalities result not only in hyperactivity of the hippocampus but also in dysfunctional connectivity, which includes connections to the striatum and the frontal lobes [126,129,130].
Moreover, with regard to the neurotrophic hypothesis of ECT, there is considerable evidence that neurogenesis functions are altered in schizophrenia [131-133]. Animal models of psychosis have demonstrated decreased adult neurogenesis [134-136]. However, animal models of schizophrenia are mainly induced by administering substances known to induce psychotic illness [129]. While the psychotic state itself is indeed important in understanding the pathology of schizophrenia, it may not be sufficient since schizophrenia follows a more chronic and deteriorating clinical course, including negative symptoms and cognitive impairment. Tracing adult neurogenesis in vivo in patients is methodologically difficult due to technical issues, and thus surrogate markers are frequently used to measure adult neurogenesis, such as Nestin, Ki-67 and Musashi-1, which are expressed in proliferating cells [132,137-139]. Of such markers, downregulation of Ki-67 has been observed in the dentate gyrus of patients with schizophrenia compared to controls [139]. In addition, induced pluripotent stem cell studies have modeled deficient functioning of dentate gyrus granule cells in schizophrenia, marked by alterations in gene expression of adult neurogenesis and decreased functioning [140]. Additionally, numerous genes implicated in schizophrenia, such as DISC1, Neuroregulin-1, Reelin, are associated with neurogenesis [132,141]. Although the direct findings of dysfunctional adult neurogenesis in patients with schizophrenia await verification, these functions are presumed to be altered when the previous literature is considered.
Specificity of the findings and implications
While these results provide evidence of changes in the hippocampus and insula of patients with schizophrenia, several important issues must be considered. First, might these results arise from nonspecific changes induced by ECT, such as edema, inflammation, or reactive gliosis [30]? While this is a possibility that needs to be addressed more thoroughly in future studies, existing evidence from both animal and human studies suggests that the effects of ECT cannot be fully attributed to these nonspecific effects. While ECS in animal models potentiates a wide range of alterations covering various regions of the brain, the results of ECS studies demonstrate rather specific changes in the hippocampal region with marked alterations in neuroplastic functions [142]. Additionally, in human studies, neuroimaging within 15 hours after ECT did not detect marked change in fluid shifts in the hippocampal region [30,143]. Moreover, studies of patients with MDD that controlled for overall cerebral volumes to address these issues have also reported a significant increase in the volume of the hippocampus apart from such nonspecific effects [30,144-147].
Second, are these changes common both to MDD and schizophrenia, or are they disease-specific? Previous attempts to explain the mechanisms underlying ECT have largely focused on the overall ECT effect, without differentiating between the two disorders [26]. While conclusions based on the currently insufficient body of evidence may be preliminary, the hippocampus appears to be commonly modulated in both animals and human subjects (including both patients with MDD and schizophrenia), while comparisons of patients with MDD with patients with schizophrenia observed increased volumes in the right insula restricted to the schizophrenia group [43]. However, this evidence is preliminary and needs replication, and current research is even more scarce in terms of what are the requisite conditions for ECT to be effective and the relationship between hippocampal modulation and symptom improvements.
An important difference in the application of ECT between patients with MDD and schizophrenia is that ECT results in a very high proportion of responses and remission among patients with MDD [148]; however, approximately one-third of patients with schizophrenia do not adequately benefit from ECT treatment [19]. Therefore, to clearly delineate schizophrenia-specific ECT treatment effects from the common effects of electrical stimulation, classifying patients into responders and nonresponders and comparing between the two groups might prove useful in future studies.
Furthermore, as the discovery of the effect of chlorpromazine preceded the development of the dopamine hypothesis, efforts to identify the mechanism of ECT may also help to improve our understanding of treatment-resistance in patients with schizophrenia. While treatment-resistance constitutes a serious mental health problem, the neurobiological underpinnings of TRS are at best only poorly understood due to the lack of consistent findings hitherto [149-151]. Because it can now be appreciated, based on large volumes of previous animal and MDD research, that the effects of ECT are specific to some regions, establishing the neurobiological substrates of ECT and combining them with stratification based on treatment response may provide some valuable insights to understanding the neural underpinnings of TRS.
Limitations
There are several limitations of this review. First and most importantly, a small number of studies with divergent modalities precluded a systematic meta-analysis. Second, individually selected ROIs among various studies also made it difficult to infer which region or networks were most consistently modulated after ECT in schizophrenia patients. Third, as discussed above, hippocampal and insular modulation might be a common end result of ECT and may not define schizophrenia-specific alterations.
CONCLUSIONS
This systematic review presents preliminary evidence of hippocampal and insular modulation after ECT in patients with schizophrenia. This holds true for morphometry, FC, and symptom association measures. Other potential candidates include the DMN, PFC, and thalamostriatal system, as demonstrated by MRS and fMRI studies, and the amygdala, along with the hippocampus and insula, which were associated with symptom reductions. However, due to the small number of studies, replication is indispensable to generalize and elaborate our understanding of the neurobiological underpinnings of the ECT effect in schizophrenia patients.
We believe that ECT provides a unique window to the understanding and management of treatment-resistance in patients with schizophrenia. However, the effect and mechanism of action of ECT are most likely to be complex and possibly mediated by various structural, functional, and metabolic alterations. Dysfunctional neurotrophic factors in schizophrenia could partially be remedied by ECT, but other factors, including neurotransmitter changes, synaptic remodeling, and restoration of altered FC in other largely distributed networks, may also play an important role. To disentangle the mystifying mechanisms of ECT, augmentation of functional approaches (functional MRI, MRS, electroencephalography) with morphometric results might prove useful in future study designs.
Supplementary Materials
The online-only Data Supplement is available with this article at https://doi.org/10.30773/pi.2020.0438.
Acknowledgements
This research was supported by the Brain Research Program and the Basic Science Research Program through the National Research Foundation of Korea (NRF), funded by the Ministry of Science, ICT & Future Planning (Grant nos. 2017M3C7A1029610 and 2019R1C1C1002457).
Notes
The authors have no potential conflicts of interest to disclose.
Author Contributions
Conceptualization: Minah Kim, Jun Soo Kwon. Data curation: Sun-Young Moon, Minah Kim. Formal analysis: Sun-Young Moon, Minah Kim. Funding acquisition: Minah Kim, Jun Soo Kwon. Investigation: all authors. Methodology: Sun-Young Moon, Minah Kim. Project administration: Minah Kim. Resources: Minah Kim, Jun Soo Kwon. Supervision: Minah Kim. Validation: Minah Kim, Se Hyun Kim, Jun Soo Kwon. Writing—original draft: Sun-Young Moon. Writing—review & editing: Minah Kim, Se Hyun Kim, Jun Soo Kwon.