Measuring the Quality of Life for Individuals With Prolonged Social Withdrawal (Hikikomori)
Article information

Abstract
Objective
This study aimed to develop a quality of life scale for hikikomori (QOL-H), measuring the subjective quality of life (QOL) of individuals with hikikomori, and confirming its reliability and validity.
Methods
The characteristics of the scale were examined using item response theory. Data were collected from 99 people with hikikomori, 100 people who had experienced hikikomori in the past, and 198 people who had not experienced hikikomori, to develop the scale, examine its reliability, validity, and characteristics. For convergent validity, the correlation coefficients between QOL-H and social interaction behaviors, hikikomori characteristics, depressive symptoms, subjective happiness, and difficulty in social participation were calculated.
Results
Good internal consistency, test-retest reliability, and convergent validity were confirmed for the QOL-H. Furthermore, significant differences in scores among all groups confirmed adequate criterion-related validity. Total information function indicated a high measurement accuracy when QOL was average or slightly high.
Conclusion
This study suggests that QOL-H can be an appropriate measure of QOL for individuals with hikikomori.
INTRODUCTION
Hikikomori, or prolonged social withdrawal, became known in Japan in the 1990s and is gradually becoming an international phenomenon, with cases being reported in countries/ regions such as India, Korea, USA [1], Brazil [2], China [3], Croatia [4], Hong Kong [5], Spain [6], and Ukraine [7]. Hikikomori is defined by the Japanese Ministry of Health, Labour and Welfare’s research group as a phenomenon with characteristics including avoidance of social interactions (e.g., attendance at school and work, socializing outside one’s home, staying at home on most days except solitary outings) for more than six months [8].
Most hikikomori phenomena relate to the difficulties of life of those who experience it. People with hikikomori have difficulties in interpersonal relationships [9-11], and 80.3% of those who utilized mental health welfare services were diagnosed with other psychiatric disorder(s), such as mood, anxiety, personality, or developmental disorders [12]. Furthermore, severe physical problems, including nutritional disorders [13] and increased body weight and obesity may be found in hikikomori cases [14]. Some studies developed tools to assess the clinical picture of hikikomori, including psychological and behavioral characteristics [15], affinity for hikikomori [16], and social interaction [10].
Traditionally, psychosocial support for hikikomori has focused on social participation and reintegration. However, people with hikikomori do not always seek social participation, and may focus on improving their quality of life (QOL) without working [8]. Furthermore, even if their hikikomori improves and they begin to participate in society, their subjective QOL may not increase sufficiently. For these reasons, people who have experienced hikikomori and mental health professionals in Japan have repeatedly expressed that support should focus on the individual’s living difficulties rather than social participation such as employment. This opinion has been shared in media broadcasts and is gaining popularity in Japan. Thus, there is a growing social awareness that support for hikikomori should focus on reducing the person’s difficulty with living, that is, improving their QOL [17]. This requires a scale that appropriately assesses the QOL of people with hikikomori. Moreover, as the QOL of each individual with hikikomori varies largely, the variation must also be addressed. However, currently, no assessment tool focuses on the subjective QOL specific to hikikomori.
QOL is defined as an individual’s perception of their position in life based on their culture and value systems, goals, expectations, standards, and concerns [18]. Previous studies have used existing scales, which are not specific to hikikomori to assess the QOL of these individuals [7,19,20]. However, individuals with hikikomori have a different living environment than those without. For example, they do not attend school or work, do not interact with others, live with their parents, and often avoid treatment. They face difficulties in social interactions and spend a majority of their time at home. However, existing QOL scales do not measure these factors, making it difficult to adequately assess changes in QOL during hikikomori. Therefore, a tool to assess QOL specific to hikikomori is needed.
In this study, we developed a scale to assess the QOL specific to hikikomori and confirmed the psychometric properties.
METHODS
Participants
Among the participants recruited using the online platform, those between the ages of 20 and 64 were included in the analysis. Data were collected from individuals managed by a major, nationwide Internet research corporation, Rakuten Insight, Inc. (Tokyo, Japan), which maintains a pool of 2.2 million members in Japan. The participants resided in the following regions: Hokkaido (4.5%), Tohoku (6.5%), Kanto (38.0%), Chubu (13.4%), Kinki (23.4%), Chugoku (3.5%), Shikoku (3.5%), and Kyushu (7.1%) regions. They were asked if they currently or in the past met the definition of hikikomori [8]. If they answered “Yes” and the duration was six months or more, we defined them as having experienced hikikomori.
Procedure
We classified the participants into three groups: individuals with no experience of hikikomori (control group), those currently experiencing hikikomori (hikikomori group), and those who had previously experienced hikikomori (previous group). To be eligible for the study, participants had to respond to all items regarding their age, sex, and duration of hikikomori. We matched the previous group or control group on sex and age with the hikikomori group. All participants agreed to participate voluntarily and were free to withdraw at any time.
Instruments
Demographics
Participants reported their age, sex, number of days they spend out of their house in a month, difficulty in social participation (1, not difficult at all to 10, very difficult), experience of hikikomori [8] in the present or the past, and the duration of their experience.
Quality of life scale for hikikomori
We selected 50 items, based on the findings of the preliminary research and previous studies, on the description of difficulties in life for those who experienced hikikomori [21]. The preliminary research was conducted with three participants (males; average age, 44 years) who had experienced hikikomori and were currently providing peer support related to hikikomori. We asked them, “Please write down the words that describe the aspects of QOL associated with hikikomori,” and to answer freely in terms of physical, psychological, social relationships, and environment, according to the domains indicated in the previous study [22]. The authors, who are licensed psychologists and specialize in hikikomori, revised the items to check the content validity. Higher scores on the quality of life scale for hikikomori (QOL-H) indicate higher QOL for individuals with hikikomori. Participants rated each item using a 4-point scale ranging from 0 (does not apply) to 3 (does apply).
Adaptive behaviors scale for hikikomori self-report version
The adaptive behaviors scale for hikikomori self-report version (ABS-H-SR) comprises 26 items that measure (low) social interaction behavior–a core characteristic of hikikomori [10,23]. It includes four subscales: interaction, family, values (behaviors that match the values of individuals with hikikomori), and social participation inside and outside the home. Participants rated the frequency of their behaviors using a 4-point scale ranging from 0 (rarely) to 3 (often); higher scores reflect more frequent social interaction behavior. The ABS-H or self-report version has adequate reliability, criterion-related validity, discriminant validity, and construct validity [10,23].
25-item hikikomori questionnaire
The 25-item hikikomori questionnaire (HQ-25) comprises 25 items that assess hikikomori [15]. It includes three subscales: socialization, isolation, and emotional support. Participants rated each item using a five-point scale ranging from 0 (strongly disagree) to 4 (strongly agree); higher scores reflect higher hikikomori characteristics. The HQ-25 has satisfactory reliability and convergent validity [15].
Japanese version of the patient health questionnaire 9
The Japanese version of the patient health questionnaire 9 (J-PHQ-9) comprises nine items assessing the severity of depression [24]. Participants rated each item using a 4-point scale ranging from 0 (not at all) to 3 (nearly every day); higher scores reflect more depressive symptoms. The J-PHQ-9 has adequate criterion validity and construct validity [24].
Japanese version of the Subjective Happiness Scale
The Japanese version of the Subjective Happiness Scale (SHS) comprises four items assessing subjective happiness [25]. Participants rated each item using a 7-point scale ranging from 1 to 7; higher average scores reflect higher subjective happiness. The SHS has adequate reliability, convergent validity, and discriminant validity [25].
Data analysis
Data were analyzed using IBM SPSS Statistics 27 (IBM Co., Armonk, NY, USA) and Mplus 8.4 [26].
Item response theory
We performed an exploratory factor analysis (EFA) with categorical variables to confirm whether the items about QOL met assumptions of unidimensionality with respect to item response theory (IRT). We performed an IRT analysis on the hikikomori group and previous group to assess the QOL characteristics of hikikomori.
We used Samejima’s [27] graded response model for ordinal polytomous data to conduct IRT analyses, establishing parameters for discrimination and difficulty. The discrimination parameter reflects an item’s ability to differentiate among individuals with high and low underlying latent traits. In this study, the calculated discrimination parameter was corrected and used as the normal metric (D=1.702). We then plotted the total information function (TIF), which shows the test information for the ability.
Reliability and validity
The internal consistency of the total QOL-H scale was assessed using Cronbach’s alpha. Of the 199 individuals in the hikikomori group and the previous group, 100 participants responded to the QOL-H again two weeks later (time 2) to examine the test-retest reliability. The intraclass correlation (ICC) between the scores at time 1 and time 2 was calculated. As the anchor, we asked the extent to which subjective QOL and physical and mental health changed from time 1 to time 2 on a scale ranging from -5 (much worse) to 5 (much better), with 0 indicating no change. Data from participants whose responses to any item were less than -3 or greater than 3 were excluded from the analysis of test-retest reliability.
We confirmed the criterion-related validity of the QOL-H by comparing the total among the three groups using analysis of variance. We expected the scores of those in the control group and the previous group to be higher than those in the hikikomori group. To check the convergent validity, we calculated correlation coefficients between QOL-H scores and the other scales. We expected to find positive correlations greater than 0.30 between the QOL-H, ABS-H-SR, and SHS and negative correlations between the QOL-H, HQ-25, and J-PHQ-9 based on prior literature and theoretical considerations. This cutoff value was in line with general recommendations for medium (r>0.30) associations [28].
Ethical considerations
The study was approved by the local research ethics committee of Tokyo Future University to which the authors belong (approval number 112). Participants were informed that the submission of their responses would be regarded as consent. The study was carried out anonymously in consideration of the participants’ privacy.
RESULTS
The mean age of the hikikomori group was 44.58 (standard deviation [SD]=9.69) years, and 70.7% of them were male. The number of days out of home was highest in the control group, followed by the previous group and the hikikomori group. Significant differences were found between the three groups in all the scales—difficulty in social participation, social interaction behaviors, hikikomori characteristics, depressive symptom, and subjective happiness (Table 1).
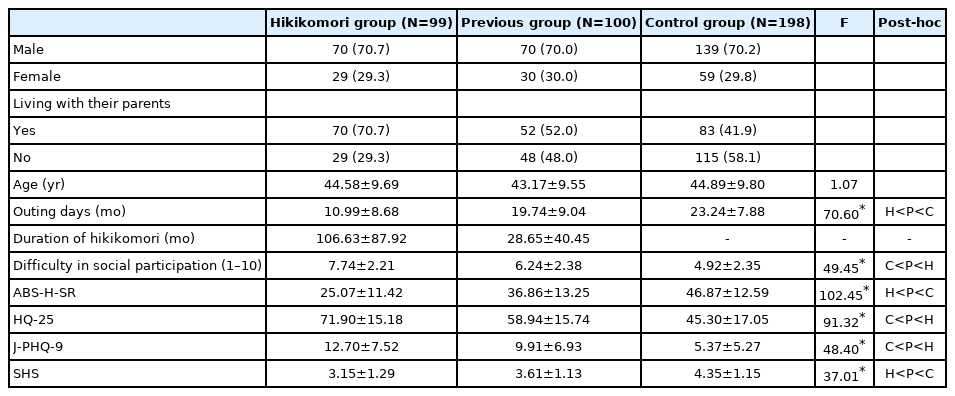
Demographics of participants
Selecting quality of life scale for hikikomori items
We excluded the three items that showed ceiling or floor effects based on the means and SDs (item 26, 2.21±0.89; item 28, 0.86±0.90; item 29, 0.78±0.80). Additionally, we excluded the two items with a coefficient lower than 0.30 by item-reminder correlations analysis.
The results of the scree plot from the EFA strongly supported a single factor, with the first eigenvalue over five times as large as that of the second factor and substantially larger than that of the others (17.49, 3.25, 2.18, 1.95, etc.). The factor loadings for the single-factor solution were all positive and ranged from 0.32 to 0.84. The Cronbach’s alphas were also high (α= 0.95) and mostly unchanged regardless of which items were deleted (0.949 to 0.952). These findings suggest that the QOLH met the unidimensionality assumption allowing us to proceed with the IRT analysis.
We analyzed the 45-items using IRT analysis to confirm discrimination and difficulty parameters. The results of IRT were discrimination parameter 0.32 to 1.47 and difficulty parameters b1=-4.40 to -0.55, b2=-1.56 to 2.06, b3=-0.55 to 5.49. Items with discrimination of less than 0.80 [29] were deleted, and finally, the QOL-H, consisting of 20 items, was developed.
Table 2 shows IRT parameters, factor loadings, and Cronbach’s α if the item is deleted from QOL-H. The results were discrimination parameter 0.85 to 1.76 and difficulty parameters b1=-3.02 to -0.60, b2=-0.26 to 2.22, b3=2.39 to 5.78 (Supplementary Figure 1 in the online-only Data Supplement). Inspection of the TIF indicated that the 20-item QOL-H had greater precision at around θ=0 to 1 on the QOL trait continuum (Figure 1).
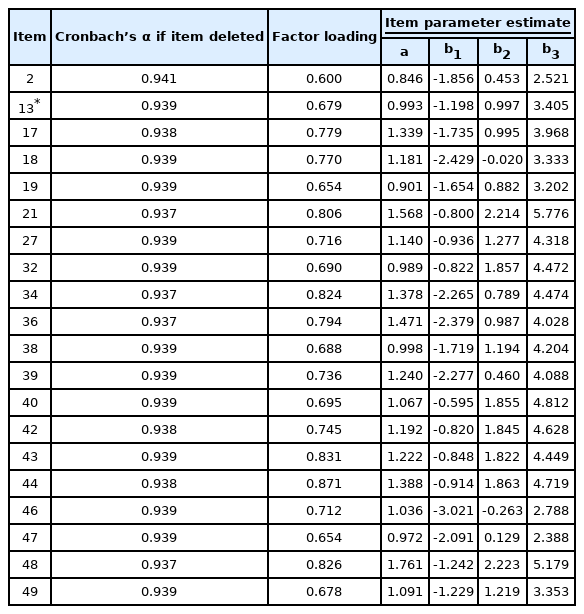
Item response theory parameters for the 20 items of the quality of life scale for hikikomori

Total information function for the quality of life scale for hikikomori.
Reliability and validity
The Cronbach’s alpha for the QOL-H indicated high internal consistency (α=0.94). The ICC, using data from 91 participants with responses to both anchor items ranging from -3 to 3, showed high test-retest reliability (0.86; 95% confidence interval, 0.80 to 0.91).
Significant differences were found between all groups (F (2, 394)=56.75, p<0.001; Table 3). Post-hoc analyses showed that QOL-H scores were highest in the control group, followed by the previous group and the hikikomori group.

Means, standard deviations, analysis of variance results, and effect sizes for the 20-item quality of life scale for hikikomori
As expected, the QOL-H were significantly and positively correlated with the ABS-H-SR (r=0.57), SHS (r=0.64) and negatively correlated with HQ-25 (r=-0.42), J-PHQ-9 (r=-0.70), which confirmed the convergent validity (Table 4).

Correlations with the scores of the quality of life scale for hikikomori (N=199)
DISCUSSION
This study aimed to develop a scale to assess the QOL specific to hikikomori and confirm its psychometric properties, including the item trait, reliability, and validity.
The average IRT discrimination parameter was 1.19 and showed that the QOL-H had good measurement accuracy of assessing QOL of individuals who experienced hikikomori. TIF indicates that this scale has high measurement accuracy when QOL is around average or slightly high. Among the 20 items of QOL-H, item 48 (I feel that my life is meaningful) had the highest discrimination, followed by item 21 (I am satisfied with myself). This may be due to the relevance of these items to overall QOL. Items 21 and 48 showed high item difficulty in b3; a high QOL is required to score highly on these items. Item 32 (I am satisfied with my ability to work), and item 40 (I am satisfied with my sociability) had high measurement accuracy when QOL was higher than average, which may be because these items are directly related to the characteristics of hikikomori. The difficulty level of item 46 (I can take part in relaxing day-to-day activities) and item 47 (I can easily engage in activities outside my home) were relatively low compared to the other items, and there was a peak in measurement accuracy when QOL was a little low. This result may indicate that increasing the relaxing activities in one’s life may improve QOL for people with hikikomori, especially those who have low QOL.
This study indicated that QOL-H had sufficient internal consistency, test-retest reliability, and convergent validity. In the present study, we used emotional and behavioral variables to examine convergent validity, but further studies are needed to examine the relationship of QOL-H with objective functioning in life or QOL as rated by a third party such as a clinician or researcher. Furthermore, future studies should also examine whether QOL-H can sensitively reflect changes in QOL. The results of criterion-related validity suggest that QOL-H is sensitive to the differences in QOL between people who have experienced hikikomori and those who have not, and between people who currently have hikikomori and those who have recovered from it.
However, the study has some limitations. First, the sample bias cannot be denied. This study is web-based research, and web-based research has the benefit of increasing access to hikikomori people. However, people who are not familiar with the Internet would not have been included in the participants of this study. Second, the average age of the participants was over 40 years old, and there were relatively few young participants. Therefore, the findings of this study can only be interpreted in light of these characteristics of the participants in this study. Further, future studies are needed to confirm whether the findings of this study will be reflected in countries other than Japan. It should be examined whether QOL-H can measure QOL appropriately for culturally different hikikomori because their cognition or lifestyle may differ by culture even if they show similar behavioral characteristics [30]. Lastly, another limitation is that existing scales such as the Lubben Social Network Scale [31] were not used in assessing the difficulty in social participation to reduce the burden on the participants.
Psychosocial interventions for people with hikikomori should focus on QOL as well as on psychiatric symptoms and psycho-behavioral characteristics. The QOL-H developed in this study had sufficient reliability, validity, and high discrimination. The QOL-H can be useful in assessing the QOL of people with hikikomori in order to develop psychosocial intervention for people with hikikomori and monitoring its effects.
Supplementary Materials
The online-only Data Supplement is available with this article at https://doi.org/10.30773/pi.2021.0348.
Item information curve.
Notes
Availability of Data and Material
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Conflicts of Interest
The authors have no potential conflicts of interest to disclose.
Author Contributions
Conceptualization: Shunsuke Nonaka, Motohiro Sakai. Data curation: Shunsuke Nonaka. Formal analysis: Shunsuke Nonaka. Funding acquisition: Shunsuke Nonaka. Investigation: Shunsuke Nonaka. Methodology: Shunsuke Nonaka. Project administration: Shunsuke Nonaka. Resources: Shunsuke Nonaka. Software: Shunsuke Nonaka. Supervision: Motohiro Sakai. Validation: Shunsuke Nonaka. Visualization: Shunsuke Nonaka. Writing—original draft: Shunsuke Nonaka. Writing—review & editing: Shunsuke Nonaka, Motohiro Sakai.
Funding Statement
This work was supported by JSPS KAKENHI (Grant Numbers: 20K14199) and by Tokyo Future University. The funding source had no role in the study design; the collection, analysis, and interpretation of data; the writing of the report; or the decision to submit the article for publication.
Acknowledgements
We would like to thank the participants of this study. We would like to thank Editage (www.editage.jp) for English language editing.