Korean Validation of the Temperament Evaluation of Memphis, Pisa, Paris, and San Diego Autoquestionnaire
Article information

Abstract
Objective
The Temperament Evaluation of Memphis, Pisa, Paris, and San Diego Autoquestionnaire (TEMPS-A) has been validated in more than 30 languages and is noted for its broad application in research and clinical settings. This study presents the first attempt to examine the reliability and validity of the TEMPS-A in Korea.
Methods
A total of 540 non-clinical participants completed the Korean TEMPS-A, which was adapted from the original English version via a comprehensive translation procedure. Reliability was assessed using Cronbach’s α, and associations between temperaments were examined using Spearman’s correlation coefficient. Exploratory factor analysis (EFA) was performed, and differences in TEMPS-A scores between the gender- and age-based groups were examined using Kruskal-Wallis analysis.
Results
The Korean TEMPS-A exhibited excellent internal consistency (0.70–0.91) and significant correlations between subscales. EFA resulted in a two-factor structure: Factor I (depressive, cyclothymic, irritable, and anxious) and Factor II (hyperthymic). Gender and age group differences were observed.
Conclusion
Overall, our results suggest that TEMPS-A is a reliable and valid measure of affective temperaments for the Korean population. This study opens new possibilities for further research on affective temperaments and their related traits.
INTRODUCTION
The concept of temperaments can be traced back to the humoral theory developed by Hippocrates (5th century B.C.), which posits that individuals’ physical and psychological health are dependent on whether or not their four bodily fluids are in balance [1]. In addition, Hippocrates believed that each of these four humors (black bile, yellow bile, blood, and phlegm) represented a personality type: black bile was associated with a depressive temperament, yellow bile with cyclothymic, blood with hyperthymic, and phlegm with phlegmatic temperaments [1]. It was believed that when one humor predominates others, the temperament linked to that humor is expressed [1]. Kraepelin [2] took this notion and further theorized that there were four basic affective dispositions: depressive, cyclothymic, manic, and irritable. Kraepelin believed that these temperaments are subclinical manifestations of affective disorders [2]. In the modern era, Akiskal et al. [3] adapted Kraepelin’s theory to describe five disposition types (i.e., affective temperaments): depressive, cyclothymic, hyperthymic, irritable, and anxious.
Similar to Kraepelin [2], Akiskal and his collaborators [3,4] define affective temperaments as underlying traits of mood disorders or stable traits of mood disposition. However, Akiskal et al. [3] also acknowledge that affective temperaments have an evolutionary basis and may also serve some positive functions. For example, those with hyperthymic temperament are usually full of energy and require less sleep, allowing them to be more productive than others. Individuals with anxious temperament worry frequently and tend to be very cautious, which may be useful in keeping themselves and their family safe. Some items included in the Temperament Evaluation of Memphis, Pisa, Paris, and San Diego Autoquestionnaire (TEMPS-A) for depressive temperament such as “It is natural for me to be neat and organized,” which reflect social benefits for these individuals [3,5]. Akiskal et al. [3] developed the TEMPS-A to measure these five affective temperaments in both the general and clinical populations. TEMPS-A is a self-report, yesor-no type scale with 110 items for females and 109 items for males [3]. The number of items differ for females and males as a question regarding menstrual cycles was designated only for females. Item content for each temperament subscale includes emotional reactivity, cognitive, psychomotor, circadian, and social behavior sections [3].
Since its development, TEMPS-A has been translated and validated in more than 30 languages [6], including French [5,7], Polish [8], Italian [9], Arabic [10], Japanese [11,12], Mandarin [13], and Portuguese [14]. In addition, TEMPS-A can be utilized to compare and differentiate between mood disorders and between the non-clinical and clinical populations [15-17]. TEMPS-A has also shown efficacy in distinguishing between first-degree relatives of patients with bipolar disorder and non-clinical control participants without a history of mood disorders, even when these first-degree relatives did not show any symptoms [18]. This further demonstrates the utility of TEMPS-A and the important role TEMPS-A can play in the distinction of individuals at familial risk of mood disorders to inform clinical decisions (e.g., monitoring or psychoeducation). Moreover, TEMPS-A can be further utilized in clinical settings as an individual’s temperament can influence medication adherence, treatment response, and clinical course [19-23]. However, despite its significance in psychiatry, the TEMPS-A has not yet been translated and validated in Korean. Therefore, the objective of this study was to evaluate the reliability and validity of the TEMPS-A in a non-clinical Korean adult population.
METHODS
Participants
A total of 540 healthy participants from the general population took part in this study. Participants were equally recruited by gender and age group over a span of two weeks in July 2021 through an online survey. A survey including demographic questions and TEMPS-A items was developed and SurveyBilly, an online survey distribution platform, was utilized to collect the data. An online survey was chosen to reach a large, diverse range of respondents in a time- and cost-efficient manner. Participants were excluded from the study if they self-reported a history of psychiatric diagnosis. The sample consisted of 270 men and 270 women aged between 19 and 60 years. Before participating in the present study, all participants were informed about the purpose of the study. This study was approved by the Institutional Review Board of Seoul National University Bundang Hospital (protocol code X-2107-696-903, approved July 1, 2021). Informed consent was waived as researchers did not have direct access to participants’ personal information, and anonymized survey data were used for analyses.
Methods
The full TEMPS-A questionnaire consisting of 110 questions (109 for men) was used to assess five temperament traits (depressive, cyclothymic, hyperthymic, irritable, and anxious). All TEMPS-A items were scored dichotomously: “Yes=1” and “No=0.” Items belonging to each subscale were as follows: depressive temperament consists of items 1–21 (21 questions), cyclothymic temperament consists of items 22–42 (21 questions), hyperthymic temperament consists of items 43–63 (21 questions), irritable temperament consists of items 64–84 (21 questions for women and 20 questions for men), and anxious temperament consists of items 85–110 (26 questions). Item 84 asks specifically about temperament before menstrual cycles, and was designated only for women.
The original questionnaire was first translated into Korean and subsequently back-translated into English by a certified bilingual translator. The latter translation was approved by the first author of the original English version (H. S. Akiskal) and two board-certified psychiatrists (J-MW and WM), and the final version was modified appropriately.
Statistical analysis
The scores for each temperament were represented by mean values (sum of variables’ scores belonging to the subscale/number of variables [nv]: [V1+V2+....+Vn]/nv). The normality of the distribution of the analyzed variables was verified using the Shapiro–Wilk analysis. Because the parameters did not conform to the normal distribution, non-parametric analyses were performed in correlation tests among the subscales (Spearman’s rank correlation coefficient) and tests for differences in TEMPS-A scores between gender and age groups (Kruskal-Wallis analysis).
The internal consistency of the full questionnaire and its subscales was measured using Cronbach’s α, a reliability coefficient. Exploratory factor analysis was performed using principal component analysis (PCA) with varimax rotation. R 3.5.1 (R Foundation for Statistical Computing, Vienna, Austria; http://R-project.org/) software was used for all the analyses.
RESULTS
Clinical and demographic characteristics
The mean age of the participants was 39.53 years (standard deviation [SD]=10.92), and 50% were women. Other clinical and demographic characteristics are shown in Table 1.
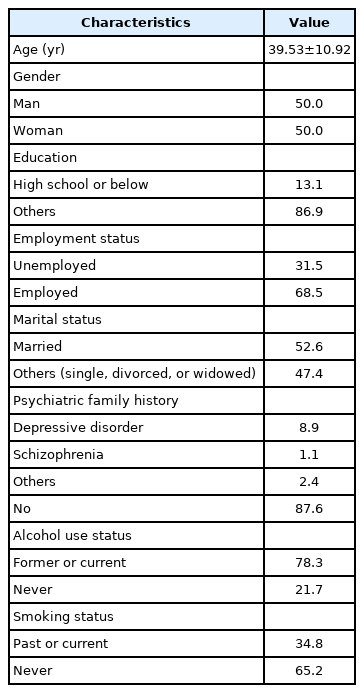
Clinical and demographic characteristics of subjects (N=540)
Reliability analysis
The Cronbach’s alpha coefficients for each temperament (depressive, cyclothymic, hyperthymic, irritable, and anxious) and the full questionnaire are provided in Table 2. All subscales showed an alpha coefficient of 0.7 or above: depressive (α=0.70), cyclothymic (α=0.86), hyperthymic (α=0.85), irritable (α=0.83), and anxious (α=0.89). The total internal consistency value for the Korean TEMPS-A was 0.91.

Reliability analysis results based on the Cronbach’s alpha
Correlations within the scales of TEMPS-A
The results of the correlation analyses among the subscales are presented in Table 3. All correlations among temperaments were significant. Another notable finding was that only the hyperthymic temperament demonstrated negative correlations with other temperaments. Hyperthymic temperament was negatively correlated with depressive (r=-0.43, p<0.001), anxious (r=-0.23, p<0.001), irritable (r=-0.09, p<0.05), and cyclothymic temperaments (r=-0.10, p<0.05). Depressive temperament was significantly positively correlated with cyclothymic (r=0.53, p<0.001), irritable (r=0.48, p<0.001), and anxious temperaments (r=0.60, p<0.001). The highest positive correlations were demonstrated between cyclothymic and irritable temperaments (r=0.65, p<0.001), cyclothymic and anxious temperaments (r=0.65, p<0.001), and irritable and anxious temperaments (r=0.65, p<0.001).

Correlations between the subscales of TEMPS-A
Exploratory factor analysis
Table 4 presents the results of the exploratory factor analysis, which was conducted using PCA with varimax rotation. Factor loadings higher than 0.6 were grouped, resulting in two superfactors. Factor I (46.1%) consisted of depressive, cyclothymic, irritable, and anxious temperaments, while Factor II (18.4%) only included hyperthymic temperament. Figure 1 demonstrates the projection of the PCA results, and Supplementary Figure 1 (in the online-only Data Supplement) demonstrates the path diagram of the PCA results.

Results of the exploratory factor analysis (varimax rotation)
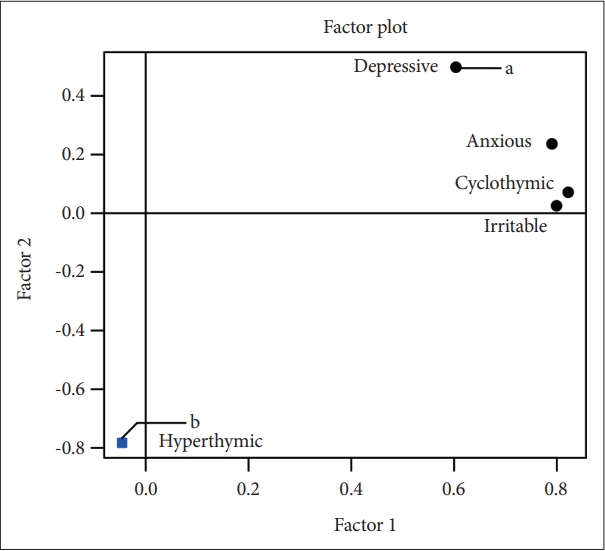
Projection of five temperaments on the plane of Factor 1 and Factor 2 from principal component analysis (varimax rotation). A black dot represents a temperament belonging to Factor I and a blue square represents a temperament belonging to Factor II. a, Factor I: depressive, cyclothymic, irritable, and anxious temperaments; b, Factor II: hyperthymic temperament.
Group differences in TEMPS-A scores in the Korean population
Using the Kruskal-Wallis test, significant differences in TEMPS-A scores were found between the two genders and across the four age groups (20s, 30s, 40s, and 50s). Figure 2 displays the results of specific post hoc comparisons using the Dunn’s test. Supplementary Table 1 (in the online-only Data Supplement) shows the mean and SD of TEMPS-A scores between genders and Supplementary Table 2 (in the online-only Data Supplement) shows the mean, SD, median, and interquartile range of TEMPS-A scores between age groups.
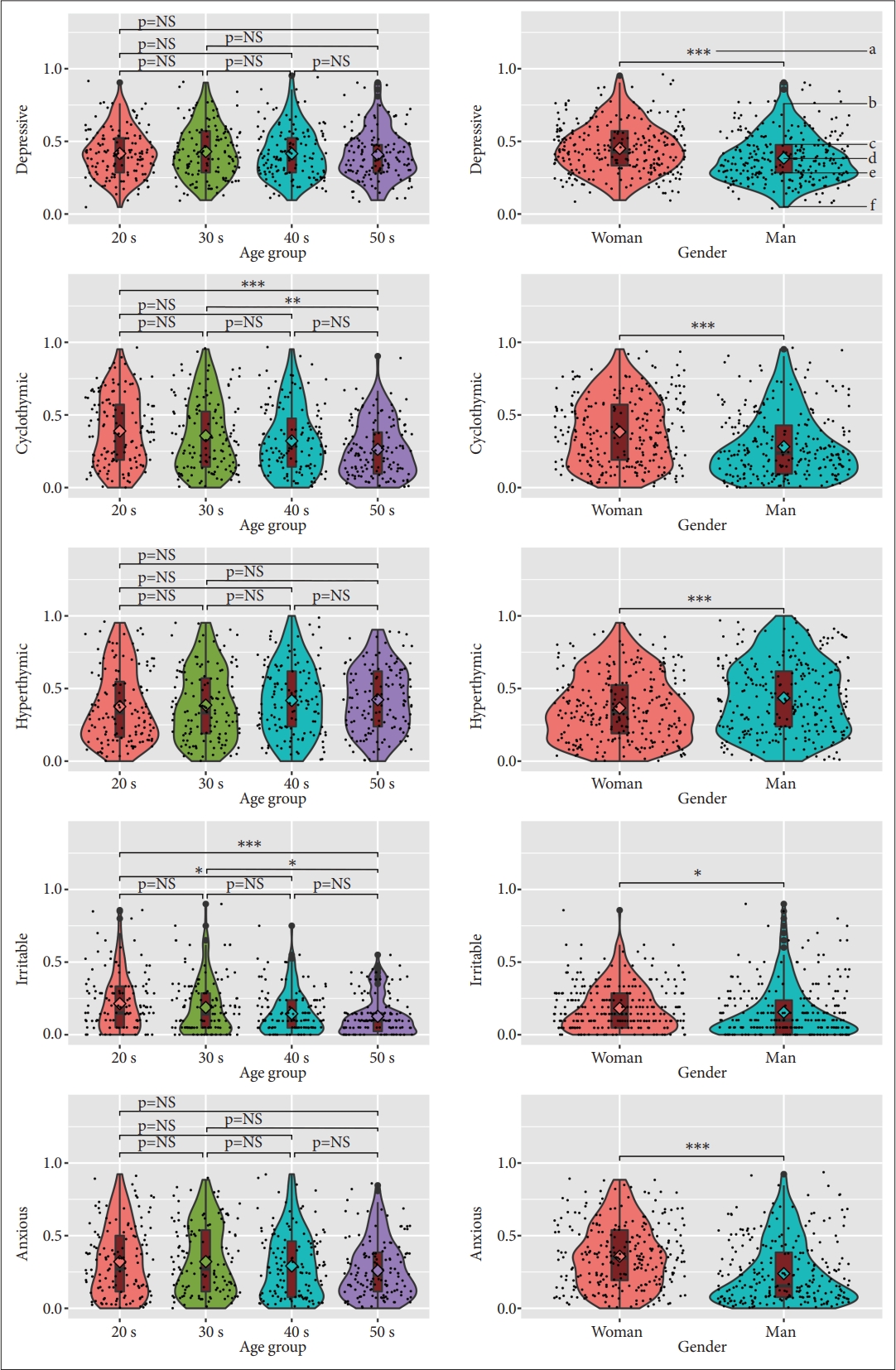
Violin plots for distribution of five temperaments according to age or gender. *p<0.05; **p<0.01; ***p<0.001. a, p-value of Kruskal–Wallis analysis; b, upper adjacent value; c, third quartile (75%ile); d, median; e, first quartile (25%ile); f, lower adjacent value; NS, no significance.
Significant differences were found across all five TEMPS-A subscales between the two genders. Depressive (p<0.001), cyclothymic (p<0.001), irritable (p<0.05), and anxious (p<0.001) scores were significantly higher in women than in men, whereas hyperthymic (p<0.001) scores were significantly higher in men than in women.
Only two temperament subscales demonstrated significant differences in TEMPS-A scores among the age groups. In cyclothymic temperament, the mean score of the 50s group was significantly lower than that of the 20s (p<0.001) and 30s group (p<0.01). In addition, in irritable temperament, the mean score of the 50s group was significantly lower than the 20s (p<0.001) and 30s groups (p<0.05), while the 40s group demonstrated a lower mean score than the 20s group (p<0.05).
DISCUSSION
Our results suggest that the Korean translation of the TEMPS-A demonstrates good reliability and validity. The reliability of the Korean TEMPS-A was proven to be satisfactory, with high internal consistency for each subscale and the scale as a whole (Table 2). The Cronbach’s alpha value for each subscale was equal to or greater than the commonly accepted standard of 0.70 [24] for depressive, cyclothymic, hyperthymic, irritable, and anxious temperaments. The full scale demonstrated a Cronbach’s alpha coefficient of 0.91, thus showing high internal consistency.
Other findings relating to validity, such as correlations between temperaments, exploratory factor analysis outcomes, and gender differences in scores, were consistent with previous studies [8,10,13,14,25-28]. The depressive, cyclothymic, irritable, and anxious temperaments showed positive and moderate to high correlations with each other and negatively correlated with the hyperthymic temperament (Table 3). In our study, the highest positive correlations were reported between cyclothymic temperament and irritable temperament, cyclothymic and anxious temperaments, and irritable and anxious temperaments. This was consistent with the validation studies conducted in the Lebanese [10], German [25], Portuguese [14], Japanese [12], and Buenos Aires populations [28], which also found moderate to strong correlations between the aforementioned three pairs of temperaments.
The strong correlation between the cyclothymic and irritable temperament can be explained by studies that report connections between cyclothymic characteristics and irritability symptoms. Regarding clinical applications of affective temperaments, Kraepelin and Akiskal, as well as other clinical researchers, have highlighted a link between cyclothymic temperament and bipolar disorder, and some even view cyclothymic temperament as a genetic diathesis for bipolar disorder [29-32]. In turn, bipolar disorder frequently coexists with irritability, and individuals diagnosed with bipolar disorder demonstrate higher scores on the irritable temperament of TEMPS-A than those with major depressive disorder [33]. As per the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition [34], irritable mood is also a qualifying criterion for depressive, hypomanic, and manic episodes. In addition, cyclothymic and irritable temperament show similar daily and clinical outcomes, both demonstrating associations with increased negative affect, perceived stress, engagement in risky and impulsive behavior, and increased rates of bipolar disorder and borderline personality disorder [35,36]. Moreover, irritability is sometimes subsumed under the concept of mood instability (also called mood lability or emotional lability), which is a key feature of cyclothymic temperament [37]. In fact, in earlier studies of affective temperaments, Akiskal et al. [38] posited that irritable temperament might include overlapping components of depressive, cyclothymic, and hyperthymic temperaments. Akiskal et al. [38] found that individuals who demonstrated dominant irritable temperament also reported moderate scores on the other three temperaments. In addition, certain items included in the irritable scale, such as being critical, expressing complaints frequently, and feeling dysphoric restlessness, were endorsed more often by individuals who demonstrated dominant depressive, cyclothymic, or hyperthymic temperaments than those with irritable temperament.
The strong correlation between cyclothymic and anxious temperaments also falls parallel to the theoretical considerations. In clinical settings, this association has been demonstrated in mood disorder patients with panic disorder and agoraphobia comorbidity, reporting significantly higher rates of cyclothymic temperament than other patients with mood disorders who were not additionally diagnosed with such anxiety disorders [39]. Furthermore, individuals with cyclothymic temperament reported more self-perceived anxiety and depression as well as having a first-degree relative with anxiety and depression [40], providing support for the notion that there may be a genetic relationship between cyclothymic temperament and anxiety disorder.
The relationship between irritable and anxious temperaments has also been alluded to in the literature. First, irritability is included as a possible symptom of generalized anxiety disorder [34], and irritability during adolescence predicted the diagnosis of generalized anxiety disorder 20 years later [41], demonstrating a longitudinal and stable relationship between irritability and anxiety. In addition, a direct link between irritability and anxiety severity was observed in children diagnosed with any anxiety disorder [42]. Another study demonstrated the unique link between anxiety and irritability by showing that they interact to influence amygdala-medial prefrontal cortex connectivity [43].
As expected, hyperthymic temperament was negatively correlated with all other temperaments (Table 3). The strongest negative correlation was observed between hyperthymic and depressive temperaments. Since hyperthymic temperament has been shown to be protective against many psychiatric disorders, including major depression [44], and since similar results have been reported by other validation studies [8,25-28], this was in line with our expectations.
Corresponding with these results, the exploratory factor analysis via PCA produced two factors, the first being a “superfactor” that consists of depressive, cyclothymic, irritable, and anxious temperament, and the second containing hyperthymic temperament (Table 4 and Figure 1). This finding is similar to the original English version, in which Akiskal and Akiskal [45] found that dysthymic, cyclothymic, and irritable temperament loaded strongly onto Factor I, while hyperthymic temperament loaded only onto Factor II. Even when exploratory factor analysis was conducted in validation studies of different languages and cultures, Akiskal and Akiskal [29] noted that the hyperthymic temperament was independent of the other four factors. The Buenos Aires study conducted by Vázquez et al. [28], and a validation study conducted in Mandarin by Lin et al. [13], also found a two-factor structure. The twosided divide between temperaments can be further explained by a Hungarian TEMPS-A study in which the s-allele of the serotonin transporter gene 5-HTTLPR was found to be significantly associated with higher scores on the depressive, cyclothymic, irritable, and anxious subscales of the TEMPS-A, but not with the hyperthymic temperament scores [46]. This finding also provides evidence for the relevance of TEMPS-A in genetic and biological investigations of affective temperaments and psychiatric disorders.
It should be noted that the hyperthymic temperament loaded negatively onto Factor II in the current study, while Vázquez et al. [28] and Lin et al. [13] found the hyperthymic temperament to load positively on Factor II. Although our results still demonstrate that the hyperthymic subscale is distinct from and orthogonal to the four other subscales, as reflected in the projection of our PCA results (Figure 1), this poses the question of how to interpret the factors in terms of clinical applications. In Vázquez et al.’s [28] and Lin et al.’s [13] research, the positive loadings of depressive, cyclothymic, irritable, and anxious subscales on Factor I and the positive loading of the hyperthymic subscale on Factor II illustrate that Factor I is a general, negative temperamental construct, while Factor II is a more positive construct. In our study, as the hyperthymic temperament loaded negatively onto Factor II, it may be thought of as an independent, negative factor that is related to the difficulty of feeling positive moods and experiencing high amounts of energy, whereas Factor I is an overall negative temperamental construct that contains depressive, cyclothymic, irritable, and anxious subscales and is similar to neuroticism.
Gender-based score differences were similar to those of other national studies on TEMPS-A, with the exception of irritable temperament. In our study, men scored higher on the hyperthymic subscale, while women scored higher on the depressive, cyclothymic, and anxious subscales. However, we found that women scored higher than men on the irritable subscale, which was contrary to most countries’ findings [8,10,13,14,25,26,28]. One possible explanation is that, in Korea, irritability is culturally accepted as a characteristic associated with women. There is still an enforced gender norm in Korea, in which men should be “cool” and should “brush off” emotional events while women are thought to be more “sensitive” and “sentimental.” This may be related to how core cultural values are more strongly associated with man stereotypes than with woman stereotypes: since Korea follows a collectivist culture, men are believed to be more communal and to value group harmony [47]. As irritability may harm group harmony and weaken social ties, Korean men may be discouraged from expressing their irritable temperament. Similarly, Kim et al. [48] found that Korean females scored higher than males on the Sentimentality value of the Temperament and Character Inventory, while males scored higher than females on the Cooperativeness subscale, further indicating that cultural norms can affect gender differences in temperament.
In terms of age-based differences in affective temperament, it was difficult to compare our findings with other validation studies, as only a few investigated age differences. However, it was clear that cultural factors played a role in the temperament scores of various age groups. For the mean scores of cyclothymic temperament, there was a continuous decreasing pattern from the youngest age group (the 20s group) to the oldest age group (the 50s group), but only the differences between the 50s group and the 20s and the 30s groups were significant. The decreasing pattern of cyclothymic temperament scores was in line with the findings of other cultures [10,14]. With irritable temperament, the mean scores decreased with age, but this difference only reached significance for the 50s group with the 20s and the 30s group, and between the 40s group and the 20s group. While the Lebanese-Arabic population similarly demonstrated that the mean irritable scores decreased with age [10], Portuguese [14] and Mandarin [13] validation studies did not show significant age differences for the irritable subscale. Since the impact of culture on affective temperaments has been demonstrated previously [49], the distinct pattern of age group differences illustrated in our study was not an issue of concern. We speculate that this decreasing pattern of cyclothymic and irritable scores with age may be due to greater emotional regulation ability and less impulsivity in older adults. In a review chapter, Kryla-Lighthall and Mather [50] discuss the role of cognitive control in emotion regulation of older adults and how it aids the decrease of negative affect and increase of positive affect via selective attention and executive processing. In a study investigating age differences in emotion regulation, Orgeta [51] explains that older adults reported lower scores in the Difficulties in Emotion Regulation Scale, especially demonstrating greater access to emotion regulation strategies and less difficulty with impulse control. These studies suggest that older adults may report less intense cyclothymic and irritable temperaments as they have gained greater ability to regulate their emotions (i.e., the ups and downs of cyclothymic temperament) and greater ability to refrain from impulsive and emotional responses to negative stimuli (i.e., irascible behaviors in irritable temperament).
The limitations of our study are as follows: First, as the survey was completed online and the participant data were anonymized, no follow-up clinician interview was conducted to confirm the participants’ history of psychiatric diagnoses. Another related limitation is that while online surveys allow us to reach a large and diverse range of respondents in theory, practical issues may prevent the sample in being representative of the general population. For example, individuals must be literate and have access to the internet in order to participate in online surveys. In addition, as we only received the anonymized data of respondents, there was limited demographic data available (i.e., only age and gender) and we were not able to verify the diversity of occupations or geographical location in our sample. For instance, groups of people in a certain institution could have responded to the survey, compromising the diversity of the sample. Moreover, the data did not conform to a normal distribution, and we had to utilize non-parametric methods of analysis, which may be less efficient than parametric tests. Moreover, as TEMPS-A is a long questionnaire consisting of 110 items (109 for men), fatigue could have been a negative factor; it may have influenced participants to haphazardly answer for the sake of completing the survey as quickly as possible. Despite these limitations, as the results of this study are similar to those of other validation studies conducted in various cultures and languages, it supports the hypothesis of TEMPS-A being a reliable and valid measure of affective temperaments in the Korean population.
In conclusion, in summary, the Korean version of the TEMPSA demonstrated good reliability and validity in a non-clinical Korean sample. The exploratory factor analysis revealed two factors: one “superfactor” that contained depressive, cyclothymic, irritable, and anxious temperaments and a second factor that only included the hyperthymic temperament. Gender differences in TEMPS-A scores were similar to those of other validation studies in various languages. Future studies are needed to test the TEMPS-A in larger Korean samples. For instance, TEMPS-A scores of non-clinical participants with confirmed absence of psychiatric illnesses may be compared to those of patients with different psychiatric disorders. With the consideration of affective temperaments as dimensions, subsequent studies may also investigate the affective temperaments’ influence on lifestyle factors, social outcomes, subclinical traits, or response to medication. With the Korean TEMPS-A as a validated addition to the progressing field of affective temperaments, international efforts to examine cultural effects on temperaments may be studied. Associations between certain temperaments and culture-bound syndromes (e.g., hwa-byung in Korea [34,52]) may also be examined, contributing to the psychiatric field at large.
Supplementary Materials
The online-only Data Supplement is available with this article at https://doi.org/10.30773/pi.2022.0089.
Mean and standard deviation of TEMPS-A scores between genders
M, SD, median, and interquartile range of TEMPS-A scores between age groups
Path diagram of the five temperaments on the plane of Factor 1 and Factor 2 from principal component analysis (varimax rotation). Same color of the line represents belonging to the same factor. The thickness of the line represents the strength of association.
Notes
Availability of Data and Material
The datasets generated or analyzed during the study are available from the corresponding author on reasonable request.
Conflicts of Interest
The authors have no potential conflicts of interest to disclose.
Author Contributions
Conceptualization: Hyeona Yu, Joohyun Yoon, Tae Hyon Ha, Woojae Myung. Data curation: Hyeona Yu, Chan Woo Lee, Ji Yoon Park, Yoonjeong Jang, Yun Seong Park, Hyun A Ryoo, Nayoung Cho, Sunghee Oh, Tae Hyon Ha, Woojae Myung. Formal analysis: Hyeona Yu. Funding acquisition: Woojae Myung. Investigation: Hyeona Yu, Joohyun Yoon, Tae Hyon Ha, Woojae Myung. Methodology: Hyeona Yu, Joohyun Yoon, Tae Hyon Ha, Woojae Myung. Project administration: Tae Hyon Ha, Woojae Myung. Resources: Woojae Myung. Supervision: Tae Hyon Ha, Woojae Myung. Visualization: Hyeona Yu, Woojae Myung. Writing—original draft: Hyeona Yu, Joohyun Yoon. Writing—review & editing: all authors.
Funding Statement
This work was supported by the SNUBH Research Fund (grant no. 09- 2020-003; WM). This work was also supported by a National Research Foundation (NRF) of Korea Grant, funded by the Korean government (NRF-2021R1A2C4001779; WM). This research was also supported by a grant of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health and Welfare, South Korea (grant number HI19C0416; WM).