INTRODUCTION
Obsessive-compulsive disorder (OCD) is characterized by repetitive and intrusive thoughts, images, or impulses and maladaptive compulsive behaviors that interfere with an individualŌĆÖs life [1,2]. Accumulating evidence has highlighted the cerebello-thalamic circuit, along with the cortico-striatothalamo-cortical circuitry, in that they contribute to various cognitive dysfunctions commonly found in OCD patients [3-6]. The cerebellum is known to communicate with various brain areas through afferent and efferent white matter (WM) bundles. In particular, the cerebello-thalamic tract, the only efferent WM bundle that connects the cerebellum and the thalamus, has been reported to modulate not only motor functions but also higher cognitive functions such as visuospatial cognition, executive function, and linguistic processing [7-9].
Recent functional magnetic resonance imaging (fMRI) studies have reported altered cerebello-thalamic functional connectivity or network patterns [10-15] in patients with OCD, and some studies have reported a relationship with OC symptom severity [12,15]. These previous functional studies highlighted the functional dysconnectivity between the cerebellum and the thalamus in the pathophysiology and cognitive dysfunctions in OCD [16-19]. However, cerebello-thalamic WM tract integrity that may underly that cerebello-thalamic functional dysconnectivity has not yet been sufficiently studied.
To date, the majority of previous diffusion tensor imaging (DTI) studies in OCD used hypothesis-free whole-brain comparison analysis (i.e., tract-based spatial statistics [TBSS]) to identify specific regions of WM alterations across the whole brain and reported compromised integrity in several WM regions in OCD patients including the superior cerebellar peduncle (SCP) [11,20]. The SCP is known as the cerebello-thalamic tract, the tract connecting the dentate nucleus, one of the deep cerebellar nuclei, and the thalamus [21-24]. However, those findings may not be sufficient to determine whether the WM integrity of the cerebello-thalamic tract is actually altered in OCD, as those findings are derived from hypothesis-free whole-brain comparison analysis, making it difficult to distinguish between the cerebello-thalamic tract and adjacent WM fibers, such as the central tegmental tract or medial longitudinal fasciculus [25,26]. Probabilistic tractography is an approach that allows specific tracing of anatomical connections between different brain regions [27,28], and is relatively appropriate for examining the WM integrity of the entire tract [29,30]. Thus, using probabilistic tractography, structural fingerprints of the cerebello-thalamic tract can be more reliably and reproducibly reconstructed and quantified than existing hypothesisfree whole-brain analysis, in that probabilistic tractography examines changes in the diffusion index of the entire tract rather than measuring regional diffusion index changes, as in hypothesis-free whole-brain analysis [31]. To our knowledge, however, there have been no studies to date examining the integrity of the cerebello-thalamic tract by applying probabilistic tractography in OCD.
This study aimed to elucidate whether aberrant WM integrity of the cerebello-thalamic tract is observed in medicationfree OCD patients using probabilistic tractography compared to that of healthy controls (HCs) [31]. Taking into consideration previous functional [16,32-35] and structural studies in OCD [11,20], we hypothesized that the WM integrity of the cerebello-thalamic tract is compromised in medication-free OCD patients compared to HCs. Specifically, we expected that decreased fractional anisotropy (FA) and increased mean diffusivity (MD) and radial diffusivity (RD) would be observed in the cerebello-thalamic tract of OCD patients.
METHODS
Participants
A total of 107 medication-free OCD patients (age range 13-48 years) and 110 age-, sex-, and handedness-matched HCs (age range 17-48 years) participated in this study. OCD patients were recruited from the OCD clinic at Seoul National University Hospital (SNUH), of which 45 patients were drugnaïve, and 62 had been unmedicated for more than four weeks prior to study participation [36]. Since we included only medication-free or drug-naïve OCD patients in this study, drug effects were considered to be controlled for, and therefore we did not include information about drug use in this paper. Diagnosis of OCD and comorbid psychiatric disorders was assessed according to the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) [37] criteria by certified psychiatrists. For OCD patients, OC symptom severity and accompanying depression and anxiety symptoms were assessed with the Yale-Brown Obsessive-Compulsive Scale, Hamilton Rating Scale for Depression, and Hamilton Rating Scale for Anxiety, respectively [38-40]. HCs were recruited from online advertisements and were screened using the Structural Clinical Interview for DSM-IV Nonpatient Edition [41]. HCs were excluded when they had any first- to third-degree relatives with psychotic disorders. Exclusion criteria for all subjects were intellectual disability (IQ <70), history of severe head injury accompanying loss of consciousness, neurological disorder, substance abuse (except nicotine), and severe medical illness that could affect cognitive functioning.
Written informed consent was obtained from all subjects in accordance with the Declaration of Helsinki after they were given a thorough explanation of the study procedure (IRB no. H-1201-008-392). For those who were less than 18 years old, written informed consent was obtained from both participants and their parents. This study was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board of SNUH (IRB no. H-2201-054-1289).
Image acquisition
All subject data were acquired using a 3T MRI scanner (Magnetom Trio; Siemens, Erlangen, Germany). T1-weighted imaging (T1WI) and diffusion-weighted imaging (DWI) data were acquired. T1WI data were acquired in the sagittal section using a three-dimensional magnetization-prepared rapid acquisition echo sequence (voxel size=1├Ś0.98├Ś0.98 mm3, repetition time [TR]=1,670 ms, echo time [TE]=1.89 ms, field of view [FOV]=250 mm, flip angle=9┬░, and 208 slices). DWI images were acquired in the axial section using echo-planar imaging (voxel size=1.9├Ś1.9├Ś3.5 mm3, TR=11,400 ms, TE=88 ms, matrix=128├Ś128, and FOV=240 mm). Diffusion-sensitizing gradient echo encoding was applied in 64 gradient directions (b-value=1,000 s/mm2). Non-DWI (B0) volume was acquired at the beginning of each scan.
Image processing
T1WI data were preprocessed using FreeSurfer version 7.1.0 to extract brain tissue from the whole head image (https://surfer.nmr.mgh.harvard.edu/). All preprocessing steps were conducted according to the automated FreeSurfer pipeline. Using FLIRT with a mutual information cost function and FNIRT with transformation matrices that were obtained from the linear method, each T1WI data point was registered to the Montreal Neurological Institute (MNI) standard space (2├Ś2├Ś2 mm3) [42].
DWI data was preprocessed using the Functional MRI of the Brain Software Library (FSL version 6.0.5; https://www.fmrib.ox.ac.uk/fsl) to remove nonbrain tissue [43] and correct eddy-current induced distortions as well as head motion [44]. We visually inspected all data for major artifacts. When registering the T1WI data to the diffusion-weighted space, b0 images of each subject were used as references. Initially, we created affine matrices to transform T1WI data to diffusionweighted space using FLIRT with a mutual information cost function. Then, these metrices were combined with transforms that were previously created from T1WI nonlinear registration to the MNI space [42].
Probabilistic tractography and diffusion index calculation
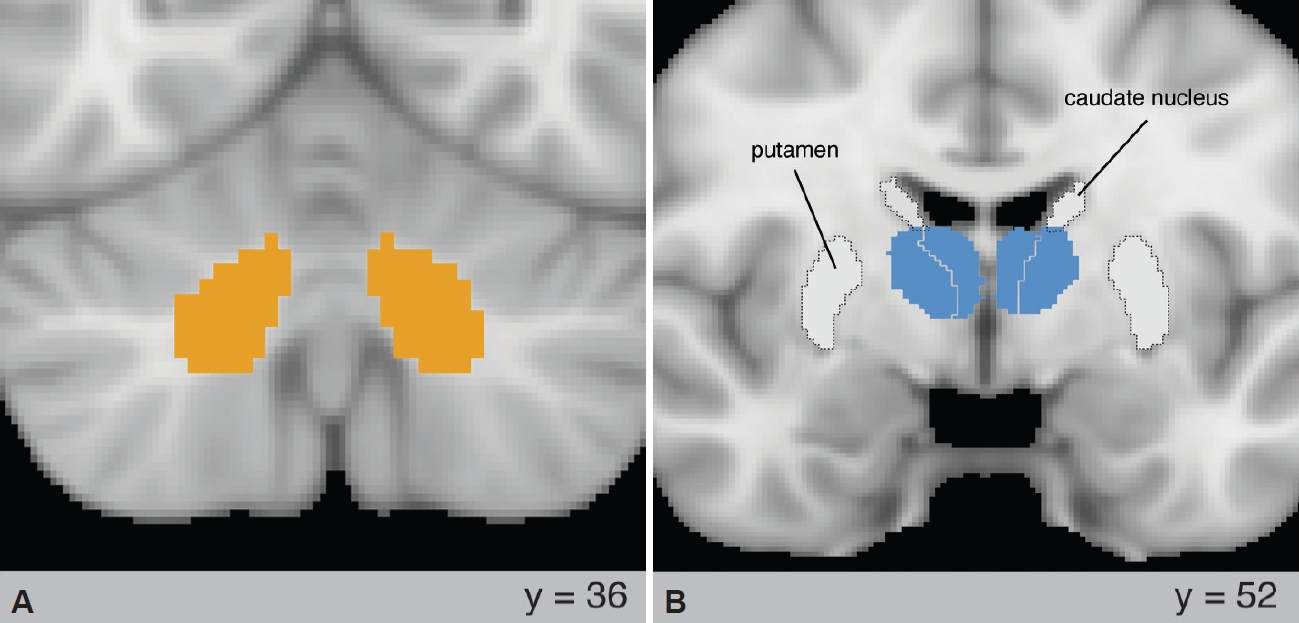
To evaluate WM integrity of the cerebello-thalamic tract, FSL probabilistic tractography [45] for each side of the brain with default option of the probtrackx2 GPU (curvature threshold=78┬░, streamlines per voxel=5,000, maximal number of steps=275, step length=0.5 mm, loopcheck, and one-way condition) was conducted using the ipsilateral dentate nucleus [46], taken from the probabilistic atlas of the cerebellum [47] at a 50% threshold, as a seed region (Figure 1A), and the contralateral thalamus, taken from the Oxford Thalamic Connectivity Atlas [48] at a 50% threshold, as both target region and waypoint (Figure 1B) [31]. For the cerebello-thalamic tract, to prevent interference with cerebellar regions other than the dentate nucleus, the cerebellar vermis was used as an exclusion mask. In addition, to increase the probability accuracy of the cerebello-thalamic tract, the contralateral thalamus and dentate nucleus were chosen as exclusion masks on each side of the cerebello-thalamic tract. Three diffusion indices (FA, MD, and RD) were extracted from both sides of the cerebello-thalamic tract. We applied a 15% probability threshold to estimate each cerebello-thalamic WM tract more accurately and to solve the limitation in resolution of our diffusion images and the problem of the crossing fibers caused by the low resolution of our images. As a result of the tractography, there were subjects that were drawn only on one side or not on either side of the cerebello-thalamic tract. A total of 6 subjects were drawn on one side or not on either side, including 1 OCD patient and 5 HCs, all of whom were excluded from the study. The numbers of participants included in the final analysis were 106 OCD patients (71 male and 35 female, age range 13-48 years) and 105 HCs (66 male and 39 female, age range 17-48 years).
Statistical analysis
All statistical analyses were conducted using R version 4.0.3 (https://www.r-project.org). For demographics, independent sample t-tests or chi-square tests were conducted to examine the difference between patients with OCD and HCs. A significance level of p<0.05 was used for all statistical analyses. To test for significant group differences in the cerebello-thalamic tract between patients with OCD and HCs, we conducted analysis of covariance (ANCOVA) with age and sex as covariates. The results were corrected for multiple comparisons of the 6 tests (3 diffusion indices ├Ś 2 sides of the cerebello-thalamic tract) using the Bonferroni correction. To investigate the effects of comorbidity, we divided the OCD group into 36 OCD patients with depressive disorder (34.0%) and 61 OCD patients without depressive disorder (57.5%). To identify group effects, we conducted ANCOVA with age and sex as covariates to test the three diffusion indices, and the results were corrected for multiple comparisons of the 6 tests using the Bonferroni correction.
RESULTS
Demographic characteristics of the participants are presented in Table 1. There were no statistically significant group differences in demographic characteristics between patients with OCD and HCs.
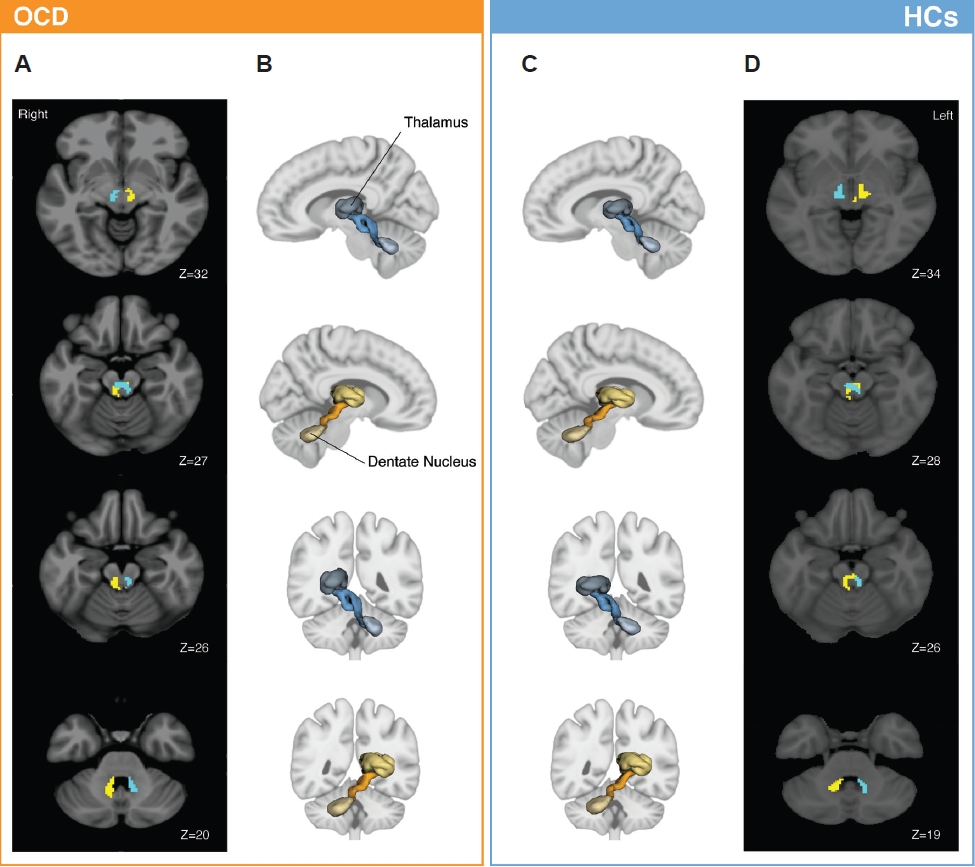
The bilateral cerebello-thalamic tracts were successfully reconstructed in 106 patients with OCD and 105 HCs (Figure 2A and B). In line with previous studies, our study also shows that the bilateral cerebello-thalamic tracts intersect each other in the midbrain area (Figure 2C and D), which is an anatomical characteristic of the cerebello-thalamic tract [21,23,31,49].
ANCOVA results of the three diffusion indices (FA, MD, and RD) from the bilateral cerebello-thalamic tract between the participants with OCD and HCs revealed that MD (F=7.98, Bonferroni corrected p=0.016) and RD (F=7.31, Bonferroni corrected p=0.031) of the right cerebello-thalamic tract at a 15% threshold were significantly increased in participants with OCD compared with the HCs (Figure 3). However, there was no significant difference for FA in the bilateral cerebellothalamic tract between groups (Bonferroni corrected p>0.999). The results of the ANCOVA comparing diffusion indices between groups are summarized in Table 2. The p-values were Bonferroni corrected for 6 tests in these analyses for multiple comparisons.
For comorbid effects of depressive disorder in patients with OCD, there were no significant differences in the three diffusion indices of the bilateral cerebello-thalamic tract between OCD patients with depressive disorder and those without depressive disorder (Supplementary Table 1 in the online-only Data Supplement). Thus, we conclude that compromised WM integrity of the right cerebello-thalamic tract may not be affected by comorbidity in patients with OCD.
DISCUSSION
To our knowledge, this is the first study to identify compromised cerebello-thalamic WM integrity in patients with OCD using probabilistic tractography. We evaluated three diffusion indices (FA, MD and RD) as markers of aberrant WM integrity in the cerebello-thalamic tract and revealed that compromised WM integrity in the right cerebello-thalamic tract was associated with increased MD and RD in OCD patients, whereas FA in the left and right cerebello-thalamic tracts in OCD patients did not differ from that in HCs. Our results demonstrate structural abnormalities in the right cerebello-thalamic tract of medication-free OCD patients, suggesting the possibility that these microstructural abnormalities in the right cerebello-thalamic tract may be related to the pathophysiology of OCD.
In this study, OCD patients showed significantly increased MD and RD in the right cerebello-thalamic tract compared to HCs, whereas there was no significant group difference in FA between OCD patients and HCs. Conventionally, unchanged FA is regarded as equivalent to WM integrity [24,50]. However, since FA is a relative measure of diffusivity, if the diffusion changes proportionally along the three eigenvectors, the sensitivity of FA may decrease, so FA alone is not enough to determine the WM integrity of the tract [51]. Thus, MD and RD, which are absolute measures that can provide quantitative information about WM integrity changes, should be considered in addition to FA. Increased MD can be explained by expansion of the extracellular space and increased water diffusivity due to abnormal cytoarchitecture or neuroinflammation, suggesting immaturity or degeneration of the cerebello-thalamic tract in patients with OCD [52-55]. In addition, increased RD usually indicates damage to myelination of axons in WM, suggesting dys- or demyelination of axons or altered myelin integrity in OCD patients [56,57]. Therefore, although it is difficult to conclude that WM integrity of the cerebello-thalamic tract is aberrated in OCD patients with intact FA values, our results of increased MD and RD in the right cerebello-thalamic tract may suggest increased overall water diffusivity due to abnormal cytoarchitecture in the tract, given that abnormal cytoarchitecture or neuronal inflammation, represented by increased MD, and dys- or demyelination of axons or altered myelin integrity, represented by increased RD, may affect WM structure.
To date, two DTI studies using whole-brain TBSS have reported cerebello-thalamic WM abnormalities in OCD patients [11,20]. In line with the current study results, Jayarajan et al. [20] reported that OCD patients showed increased RD in the WM region overlapping with the right cerebello-thalamic tract compared to HCs, but no significant group differences were found in FA values [20]. On the other hand, Tikoo et al. [11] reported significantly lower FA and higher MD in WM regions overlapping with the left cerebello-thalamic tract in OCD patients than in HCs. The discrepancy between this study and that by Tikoo et al. [11] may be due to differences in imaging analysis technique (i.e., tractography vs. TBSS) and sample sizes (i.e., 106 OCD patients in this study vs. 10 OCD patients in the study by Tikoo et al. [11]). The tractography approach allows better delineation of the WM tract than the TBSS approach; it reduces the partial volume effects and analyzes specific WM tracts as a whole rather than limiting it to small regions overlapping WM tracts. Thus, the current study results obtained using tractography in a large number of OCD patients may better explain cerebello-thalamic tract abnormalities in OCD patients than previous studies.
Previous fMRI studies have consistently reported that altered cerebello-thalamic connectivity was related to cognitive impairments found in OCD patients [7-9]. In addition, previous studies have shown that functional networks, including cerebello-thalamic circuits, were associated with OC symptom severity or OC-like behavior [11,58,59]. The current study findings, which reported increased MD and RD values in the right cerebello-thalamic tract in OCD patients, may provide structural background for those functional studies. Although future studies may focus on the direct association between OC symptomatology or cognition and impaired WM structural abnormalities of the cerebello-thalamic tract, the current study results suggest that microstructural abnormalities in the right cerebello-thalamic tract may underlie OCD pathophysiology, such as OC symptoms or cognitive impairments.
This study has several limitations. First, our results may be limited by MRI acquisition. A single B0 image and nonisotropic voxel shape might have had a slight influence on the process of WM tract reconstruction, such as fiber orientation or diffusivity mapping. During image acquisition, cardiac pulsation was not controlled, which could induce body movements. However, we excluded the subjects with images with critical artifacts through the visual inspection of every participantŌĆÖs DWI. Second, we did not perform correlation analysis between altered diffusion indices and OC symptom severity or neurocognitive function test results. Thus, interpretation regarding the current study finding of an underlying structural abnormality of OCD pathophysiology, such as symptoms or cognitive dysfunction, should be further supported by correlation analysis.
The current study indicated significantly higher MD and RD of the right cerebello-thalamic tract in patients with OCD, compared to HCs. Although there was no change in FA representing WM integrity, the increases in other diffusivity measures could indicate that the microstructure of cerebello-thalamic WM connections is possibly impaired, such as through axonal degeneration or demyelination. Based on previous fMRI studies for OCD-related behaviors, the impaired WM microstructure may underlie not only altered activity patterns between the cerebellum and the thalamus but also their behavioral dysfunction in OCD patients. Using probabilistic tractography, we reconstructed cerebello-thalamic WM connections more finely in individual subjects and subsequently measured diffusion indices. We only included medication-free patients with OCD to minimize confounding effects of psychotropic medications on WM structure60 as well as using relatively large samples. Overall, the altered WM structure between the cerebellum and the thalamus may reflect their neural dysfunction, thus suggesting an anatomical underpinning of behavioral impairments in patients with OCD.