The Association Between Alcohol Use and Suicidal Ideation Among Employees
Article information

Abstract
Objective
The risk of suicide is assessed by identifying the relationship between alcohol-use patterns and suicidal ideation in Korean employees.
Methods
The study involved 13,858 employees who underwent workplace mental health screening at the Workplace Mental Health Institute of Kangbuk Samsung Hospital over a 6-year period between 2014 and 2019. Analysis was performed separately for Alcohol Use Disorders Identification Test-Korea (AUDIT-K) items related to the frequency/volume of alcohol consumption (items 1 to 3, AUDIT-C) and those regarding alcohol dependence/related problems (items 4 to 10, AUDIT-D/P). Subjects were then classified into three groups on the basis of the presence or absence of clinical depression and suicidal ideation. The groups’ sociodemographic factors and clinical features of depression, anxiety, and alcohol-use patterns were analyzed with a chi-square test as well as one-way analysis of variance, followed by a post hoc test using the Bonferroni correction.
Results
AUDIT-K and AUDIT-D/P scores were significantly associated with the presence or absence of clinical depression as well as the presence or absence of suicidal ideation (p<0.05). However, no significant differences were found among the three groups with regard to the AUDIT-C score (p=0.054).
Conclusion
Identifying or treating alcohol dependence/related problems can help lower the occurrence of mental health problems, and suicidal ideation in particular, in employees and reduce social costs.
INTRODUCTION
The average employment rate in member countries of the Organization for Economic Cooperation and Development in 2019 was 68.7% [1]. According to data reported by the Korean government, the employment rate—the ratio of the working population to working-age population—for the same year was 66.8% [2]. Mental health problems in employees, who constitute a majority of the working-age population, can reduce the available workforce, lowering the productivity of both companies and the country. The Korea Health Insurance Policy Research Institute reported that mental health problems among employees in 2012 incurred a social cost of 8.2695 trillion Korean won [3].
Alcohol use is associated with a lot of harmful health problems and even contributes to death and disability [4]. But despite many problems of alcohol use, a culture of drinking has become widespread in Korea in which the annual drinking rate among adults reached 76.6% in 2018 [5]. Alcohol use can serve as one of the major risk factors for depression, and further death by suicide, which is revealed by many meta-analyses [6-9]. And the likelihood of death by suicide was reported to be approximately 10 times higher in persons with alcohol use disorder due to impulsiveness and cognitive error compared with members of the general population without drinking problems [10]. In addition, according to an emergency-room case-management report, 47.2% of those who attempted suicide had consumed alcohol at the time [11]. These findings suggest the importance of alcohol use in the adult suicide problem. However, most of current studies are targeting the general adult population and few studies conducted on employees who constitute the vast majority of the economically active population. And they were limited to a single group of workers, such as firefighters and soldiers [12,13].
In Korea, the suicide death rate is high, as shown in a 2019 report by Statistics Korea; in 2018, the number of suicides per 100,000 people was 26.6 which is much higher than the OECD average of 11.0 [1,14]. However, target populations in research on suicidal ideation in Korea have been limited largely to the young and elderly [15]. It is therefore necessary to investigate suicidal ideation among employees. A better understanding of the relationship between alcohol-use patterns and depression and suicidal ideation in employees may make possible early assessments of the risk of suicide on the basis of the alcohol use, even if an employee does not complain of suicidal ideation. We therefore conducted a cross-sectional examination of the relationship between alcohol use, depression, and suicidal ideation among the employed in Korea, where drinking culture is widespread.
METHODS
Study subjects
The study evaluated 15,360 male and female workers ranging in age from 20 to 65 years who underwent workplace mental health screening at the Workplace Mental Health Institute of Kangbuk Samsung Hospital over a 6-year period between 2014 and 2019. The subjects were office or manufacturing-facility workers at one of the country’s 52 public institutions or large companies. Of those, 1,502 workers who did not manifest clinical depression symptoms (a Center for Epidemiological Studies-Depression Scale score lower than 16 points) but had suicidal ideation were excluded. Data for a total of 13,858 workers were analyzed (Figure 1).
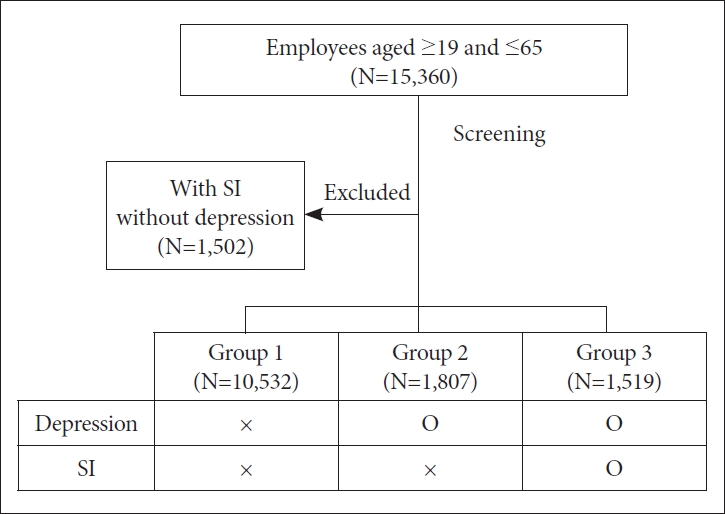
Classification of subjects into groups. Group 1: participants who had no clinical depression and no suicidal ideation; Group 2: participants who had clinical depression and no suicidal ideation; Group 3: participants who had clinical depression and suicidal ideation; O: with clinical depression or with suicidal ideation; X: without clinical depression or without suicidal ideation. SI, suicidal ideation.
The study was approved by the Kangbuk Samsung Hospital Institutional Review Board (IRB No. KBSMC 2019-01-042). Written consent forms were not obtained because the study was conducted using anonymized data only.
Measurements
Sociodemographic factors
Information on age, sex, marital status, education level, job title, and body mass index (BMI) of the study subjects was collected. Marital status included single, married, and others such as divorced, separated, or widowed. Education level either an associate degree or below or bachelor’s degree or above. Job title included staff, senior staff, assistant manager, manager, deputy general manager, general manager, executive, and others.
Assessment of alcohol consumption levels
Alcohol consumption was assessed using a version of the Alcohol Use Disorders Identification Test standardized for Koreans (AUDIT-K). The AUDIT-K consists of 10 items, including three regarding the frequency and volume of alcohol consumption in the past year, three regarding alcohol dependence, and four regarding problematic drinking behavior. Each item is given a score between 0 and 4 points [16]. In this study, analysis was performed separately for the AUDIT-K items related to the frequency/volume of alcohol consumption and those regarding alcohol dependence/related problems. The items regarding the frequency/volume of alcohol consumption are items 1 through 3, which have already been used as a screening tool for alcohol use disorder and were defined as AUDIT-alcohol consumption questions (AUDIT-C) in a study by Bush et al. [17]. The remaining AUDIT-K items, 4 through 10, were defined as alcohol dependence/related problem questions (AUDIT-D/P). This study aimed to examine whether AUDIT-D/P scores are significantly associated with suicidal ideation in employees, as compared to those for AUDIT-C.
Assessment of suicidal ideation
Suicidal ideation was assessed using one of the items regarding suicidal ideation and suicide attempts included in the Korea National Health and Nutrition Examination Survey: “Have you had a suicidal thought in the past year?.” [18] Subjects selected one of the following answers: “I have never had such thoughts,” “I have sometimes had such thoughts,” and “I almost always have such thoughts.” The subjects who responded that they never had suicidal thoughts were classified as not having suicidal ideation, and those who responded that they sometimes or almost always have suicidal thoughts were classified as having suicidal ideation.
Assessment of depression
Depression was assessed using the Korean version of the Center for Epidemiological Studies-Depression Scale (CES-D) [19], which is the most widely used screening test for the evaluation of the level of depression in adults. The CES-D is a self-reporting test comprising 20 items. The higher the total score, the more severe the depression. In this study, to increase the sensitivity in screening for depression, those with a total CES-D score of 16 or higher were deemed clinically depressed [20].
Classification of subjects into groups
Of the 15,360 subjects, the 10,532 who were not determined to be clinically depressed (due to a CES-D score below 16) and responded that they did not have suicidal thoughts were assigned to Group 1; the 1,807 who were determined to be clinically depressed (due to a CES-D score of 16 or higher) and responded that they did not have suicidal thoughts were assigned to Group 2; and the 1,519 who were determined to be clinically depressed (a CES-D score of 16 or higher) and responded that they had suicidal thoughts were assigned to Group 3. There is a temporal discordance between suicidal thoughts and clinical depression assessments [18,19].
Clinical features in other mental health areas
The Korean version of the Beck Anxiety Inventory (BAI) [21] and the World Health Organization Quality of Life (WHO-QOL) [22] tools were used to assess anxiety and quality of life, respectively. To assess stress, the Perceived Stress Scale (PSS) [23], the Daily Life Stressors Scale (DLSS) [24], and the Korean Occupational Stress Scale (KOSS) [25] were used. Finally, the Korean version of the Connor-Davidson Resilience Scale (K-CD-RISC) [26] was administered to assess resilience.
Statistical analysis
All measurements were written through a questionnaire, then we coded and anonymized. The data were analyzed using PASW Statistics for Windows, Version 18.0 (SPSS Inc., Chicago, IL, USA) A p value<0.05 was considered significant. First, to examine the sociodemographic factors and characteristics on major variables, descriptive statistics were computed for each variable. Subjects were the assigned to groups on the basis of the presence or absence of clinical depression and suicidal ideation. Those without clinical depression and suicidal ideation (Group 1), those with clinical depression but without suicidal ideation (Group 2), and those with both clinical depression and suicidal ideation (Group 3). The groups’ sociodemographic factors and clinical features of depression, anxiety, and alcohol consumption were analyzed with chi-square tests as well as one-way analysis of variance, followed by post hoc tests using the Bonferroni correction. We also performed multiple logistic regression models to evaluate the association between groups and clinical features; CES-D, BAI, WHO-QOL, PSS, DLSS, KOSS, K-CD-RISC, AUDIT-K.
RESULTS
Sociodemographic factors
Of the 13,858 subjects, 8,216 (59.3%) were male and 5,642 (40.7%) were female. In total, 3,326 subjects scored 16 or higher on the CES-D, and were determined to have significant depression symptoms; of these, 1,519 reported having suicidal thoughts. Accordingly, 10,532 subjects were assigned to Group 1 (a CES-D score below 16 and no suicidal ideations), 1,807 to Group 2 (a CES-D score of 16 or higher and no suicidal ideations), and 1,519 to Group 3 (a CES-D score of 16 or higher and suicidal ideations) (Figure 1). The results of a comparison of the groups are presented in Table 1. Moving from Groups 1 to 3, the proportion of female subjects increased (p<0.001), the proportion of married subjects decreased (p<0.001), and the proportion of subjects with less education increased (p<0.001). In addition, the proportion of subjects with a lower job title such as staff and senior staff increased compared with the proportion of subjects who were mid- or high-level managers (p<0.001) (Table 1).
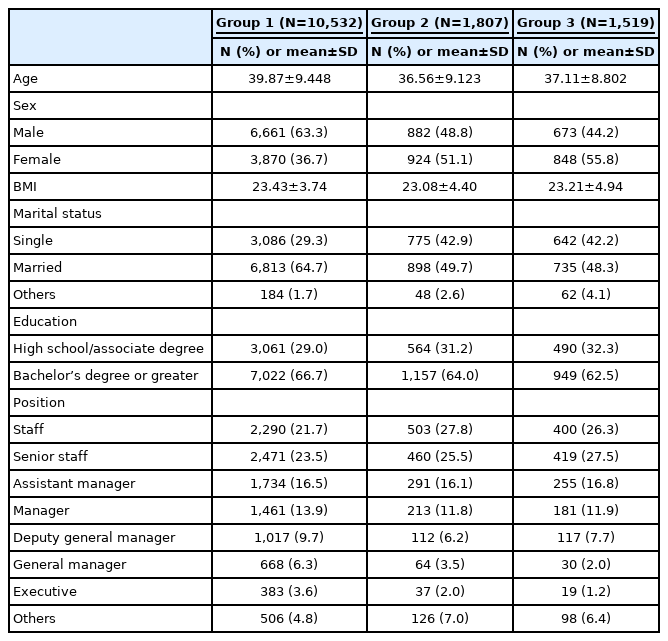
Sociodemographic characteristics of employees
Mental health clinical features
CES-D scores were 5.57±4.17 points for Group 1, 23.26±7.43 for Group 2, and 27.32±9.36 for Group 3. Likewise, BAI scores (which are indicative of the level of anxiety) and of the various scales measuring job stress (KOSS), perceived stress (PSS), and stress in a variety of everyday events (DLSS) were elevated in Group 2 compared with Group 1, and in Group 3 compared with Group 2 (p<0.001). Between-group differences were found to be significant (p<0.001) in the post hoc test, as well. The higher the K-CD-RISC and WHO-QOL scores, the higher the levels of resilience and quality of life, respectively. In both measures, the scores were highest in Group 1 and lowest in Group 3. The differences were statistically significant (p<0.001) (Table 2).

Psychiatric clinical features between groups
Analysis of the link between suicidal ideation and alcohol
Both AUDIT-K and AUDIT-D/P scores were significantly associated with the presence or absence of clinical depression as well as the presence or absence of suicidal ideation (Table 3). However, there was no significant difference among the three groups with regard to the AUDIT-C score (p=0.054).

Individual AUDIT-K factor analysis of groups
When analysis was performed on individual AUDIT-K items, only item 1 of those included in AUDIT-C (“How frequently do you drink?”) was associated with suicidal ideation (p=0.001), and none of the remaining AUDIT-C items were associated with either suicidal ideation or clinical depression. In contrast, most AUDIT-D/P items were associated with suicidal ideation and clinical depression, with two exceptions: item 6 was not associated with suicidal ideation (p=0.134) and item 9 was not associated with clinical depression (p=0.231) (Table 3).
With regard to alcohol use, both the rate of drinking and drinking behavior as well as physiological sensitivity to alcohol varied by sex and age. Consequently, additional analysis was performed after the data were grouped by the participants’ sex and age (ages 20–29, 30–39, and 40 years old and older) (Table 4). In the additional analyses, AUDIT-D/P was also significantly associated with suicidal ideation in all sex and age groups (p<0.05), with the exception of men in their 30s (p=0.213). AUDIT-D/P was also significantly associated with clinical depression in all sex and age groups (p<0.05), with the exception of women in their 30s (p=0.055) (Table 4).
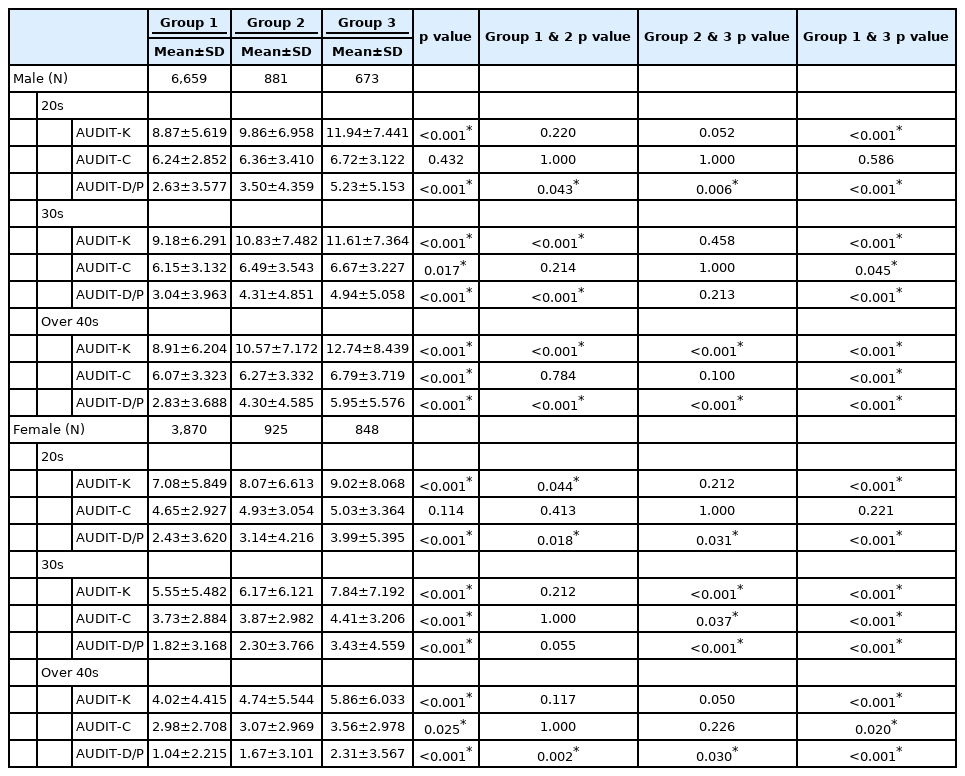
AUDIT-K–specific factor analysis by age groups
DISCUSSION
The present study examined various factors associated with suicidal ideation in employees, including depression, anxiety, stress and alcohol. The findings demonstrated that alcohol dependence/related problems after drinking in particular, were linked to both depression and suicidal ideation. Regarding the effect of drinking on suicidal ideation, Gallyer et al. [12] found in a study of 944 firefighters that drinking problems as well as workplace stress were linked to suicidal ideation. In a study of 1,582 soldiers, Cohen et al. [13] reported that alcohol dependence and depression interacted with each other to increase the risk of suicidal ideation. However, previous studies [12,13] were limited to specific occupations such as firefighters and soldiers, and no studies categorized the frequency/volume of alcohol consumption and alcohol dependence/related problems according to alcohol-use patterns. This study is the first to show a link between alcohol use and suicidal ideation using data from more than 15,000 workers across several occupations. Worker suicides incur a great social cost and induce a great deal of mental stress in colleagues [27]. The present study shows which alcohol-use patterns are linked to suicidal ideation, focusing on workers in Korea, where drinking culture is widespread.
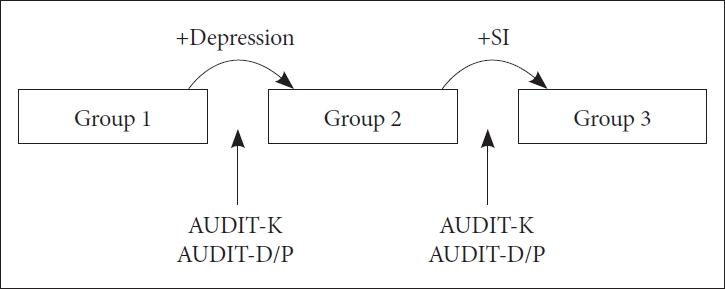
In analyses of all subjects, AUDIT-D/P but not AUDIT-C was associated with clinical depression and suicidal ideation (Figure 2). In analyses of the subjects grouped by age and sex, AUDIT-D/P scores were associated with clinical depression in all age and sex groups, except for women in their 30s, whereas AUDIT-C scores were not associated with clinical depression in any of the groups. This finding suggests that depression is linked to alcohol dependence and other related problematic behaviors, rather than the frequency and volume of alcohol consumption. In addition, suicidal ideation was associated with AUDIT-D/P scores in all age and sex groups, except for men in their 30s. These findings are largely in line with the results of analysis performed on all subjects. Depression and alcohol-use disorders are interrelated diseases and the temporal relationship is complex [28,29]. The findings of this study should be interpreted with caution. The researchers considered the following reasons for the links between AUDIT-D/P scores (identified as such for the first time in this study) and depression as well as suicidal ideation. First, regarding the association between alcohol dependence and depression, a model of self-administration of alcohol [30] can be considered. The model of self-administration of alcohol refers to self-medication through the consumption of alcohol due to depression. According to the model, to avoid negative feelings such as depression, a drinker consumes progressively larger amounts of alcohol to experience the same level of intoxication, or the individual’s tolerance to alcohol increases such that the effect of the same amount of alcohol is reduced. This results in dependence. Second, regarding problematic drinking behaviors, previous studies in which persons who exhibited problematic behaviors after drinking were compared with those without such problems have found that the risk of major depressive disorder was high in the former [31]. We therefore speculated that clinical depression and suicidal ideation are more likely to occur in drinkers with clear signs of alcohol-related problematic behaviors, because these behaviors caused by alcohol use induce persistent rumination in the drinker, giving rise to further problems, such as low self-esteem.
Comparison between groups. Group 1: participants who had no clinical depression and no suicidal ideation; Group 2: participants who had clinical depression and no suicidal ideation; Group 3: participants who had clinical depression and suicidal ideation. SI, suicidal ideation; AUDIT-K, Alcohol Use Disorders Identification Test-Korea; AUDIT-C, Alcohol Use Disorders Identification-Alcohol Consumption Score; AUDIT-D/P, Alcohol Use Disorders Identification-Alcohol Dependent-related Problem Score.
The AUDIT-K scores differed significantly between the group with both depression and suicidal ideation (Group 3) and the group with neither (Group 1). This is in line with the findings of a previous study in which a logistic regression analysis was performed on data taken from employees, and which reported that the AUDIT-K score was associated with both depressive mood and suicidal ideation (Figure 2) [32].
Because previous studies have found that drinking behavior differs between men and women [33,34], we examined the association of drinking behavior with suicidal ideation and clinical depression for men and women separately. All mean scores of the AUDIT-K, AUDIT-C, and AUDIT-D/P items were statistically significantly higher in men than in women. This likely is a function of either gender-differentiated socialization due to conventional gender roles, as shown in a study by Schulte et al. [33], or a difference in behavioral tendencies of men and women when stressed—that is, women tend to use adaptive strategies (such as talking with close friends), whereas men tend to use a non-adaptive and avoidance strategies (such as drinking), as shown in a study by Parry et al. [35]. In addition, from a physiological perspective, alcohol (which is not fat-soluble) remains in the blood for longer in women than in men, resulting in higher blood-alcohol levels as women have a higher percentage of body fat and a lower body water percentage [36]. Compared with men, women avoid drinking because there will be greater physical damage due to alcohol consumption. This may produce a gender difference with regard to the overall frequency and volume of alcohol consumption.
The study has a few limitations. First, it was based on data collected via a self-reporting questionnaire, and not on structured interviews conducted by clinicians. However, the questionnaire items used in the study are commonly utilized; the CES-D and the AUDIT-K are widely used to screen for depression and alcohol dependence, respectively. Second, the subjects of the study were among those who underwent workplace mental health screening at Kangbuk Samsung Hospital, limiting the generalizability of the findings to other workers. Third, the study was cross-sectional in design, no causal relationship between suicidal ideation and alcohol use pattern could be identified. Accordingly, future studies should take confounding factors fully into consideration. Finally, the questionnaires included past-year suicidal ideations and past-week depression. Therefore, it has been possible to have suicidal ideation over the past year, even without the current coexisting depression. So we excluded 1,502 people to eliminate temporal inconsistencies.
The strengths of the present study are as follows. First, it is the first to investigate the link between clinical depression and suicidal ideation in employees separately by the frequency/volume of alcohol consumption and dependence/related problems. Second, far more subjects (>15,000) were involved compared with previous studies, which typically involved only a few thousand. Third, this study targeted multiple occupational groups of office and manufacturing workers at large companies. Previous studies focused on a single occupation, and no study included several subjects working at a number of different institutions as was done in the present study. Our results may provide helpful insights into the understanding of depression and alcohol use pattern in employees, compared with other studies.
In conclusion, this study included a large number of subjects and a wide range of occupations to investigate the relationship between alcohol use and suicidal ideation. The results are can be generalized to all workers, unlike those of previous studies. This was a cross-sectional study and the causal relationship between suicidal ideation and alcohol consumption cannot be derived based on the study findings alone. However, identifying or treating alcohol dependence/related problems is likely to help lower the occurrence of mental health problems, and suicidal ideation in particular, in employees while reducing social costs. From the perspective of the suicidal process, we studied the suicidal thoughts of workers, but we expect it to be deeply related to their deaths by suicide [37]. Clinicians specialized in mental health in workers should be sensitive to the interrelationship between suicidal ideation and alcohol consumption. Additionally, follow-up research should be conducted to identify any causal relationships between suicidal ideation and drinking behavior in workers by controlling various variables.
Notes
Availability of Data and Material
The datasets generated or analyzed during the study are available from the corresponding author on reasonable request.
The authors have no potential conflicts of interest to disclose.
Author Contributions
Conceptualization: Sung Joon Cho, Sang-Won Jeon. Data curation: Mikyung Sim. Formal analysis: Mikyung Sim, Jinmi Seol. Investigation: Miji Lee, Sung Joon Cho. Methodology: Sung Joon Cho, Sang-Won Jeon. Project administration: Young-Chul Shin. Validation: Sang-Won Jeon, Sung Joon Cho, Jae-Hyun Park. Writing—original draft: Miji Lee, Ung Lee, Mikyung Sim, Jinmi Seol. Writing—review & editing: Jae-Hyun Park, Young-Chul Shin, Kang-Seob Oh, Dong-Won Shin, Sang-Won Jeon, Sung Joon Cho.
Funding Statement
None