Heart Rate Variability and Its Ability to Detect Worsening Suicidality in Adolescents: A Pilot Trial of Wearable Technology
Article information

Abstract
Objective
Suicide is the 2nd leading cause of death in adolescence, and acute pediatric mental health emergency department (ED) visits have doubled in the past decade. The objective of this study was to evaluate physiologic parameters relationship to suicide severity.
Methods
This was a prospective, observational study from April 2018 thru November 2019 in a tertiary care pediatric emergency department (ED) and inpatient pediatric psychiatric unit enrolling acutely suicidal adolescent patients. Patients wore a wrist device that used photoplethysmography for 7 days during their acute hospitalization to measure heart rate variability (HRV). During that time, Columbia Suicide Severity Scores (CSSRS) were assessed at 3 time points.
Results
There was complete device data and follow-up for 51 patients. There was an increase in the high frequency (HF) component of HRV in patients that had a 25% or greater decrease in their CSSRS (mean difference 11.89 ms/
Conclusion
We found an inverse correlation between parasympathetic activity measured through the HF component and suicidality in an acutely suicidal population of adolescents. Wearable technology may have the ability to improve outpatient monitoring for earlier detection and intervention.
INTRODUCTION
Suicide is the 2nd leading cause of death among adolescents, exponentially rising over the past decade and accounting for more than all other non-mental health diagnoses combined, excluding trauma [1]. Parents often utilize emergency departments (EDs) in an effort to help keep their adolescent safe when suicidal symptoms escalate. A recent nationally-representative study found that the number of ED visits for pediatric mental health complaints more than doubled in the most recent decade, now accounting for approximately 1.2 million annual visits [2]. This is a growing problem for EDs, as studies have shown that pediatric mental health patients require more resources than non-mental health patients and have lengths of stay counted in days, not hours [3,4]. Recidivism is a significant challenge, as up to 20% of unsuccessful adolescent suicide attempts will have a second attempt within 12 months of discharge, and 45% of pediatric mental health ED patients will have a subsequent visit for a similar complaint [5,6].
Given the significant public health burden, there is a critical need for improved outpatient monitoring that allows for early detection and intervention before an acute mental-health crisis results in a suicide attempt, associated ED visit, or hospitalization. Previous studies have identified physiologic markers that may help identify suicidal patients, including changes in heart rate or breathing related to stress [7-9]. Expanding on that work, it has been postulated that a dysregulation of the interplay of the parasympathetic and sympathetic branches of the autonomous nervous system is present in suicidal patients [10]. One physiologic marker for autonomic nervous system dysregulation is heart rate variability (HRV). There exist metrics focused on the parasympathetic branch, namely the high frequency component (HF) and separate metrics focused on the sympathetic branch. Prior research has found that patients with a history of suicidality demonstrate a decrease in their HF when undergoing stressful tasks [11,12]. This suggests that patients with suicidality may have impaired parasympathetic nervous system regulation. However, studies to date have been limited by measurements at a single time point and confined to laboratory settings where patients are connected to electrocardiographic (ECG) monitors. More recently, it has become possible to measure HRV through wrist-worn devices using photoplethysmography. This method has been shown to be accurate when compared to the gold standard of ECG and may be highly feasible in clinical practice among at-risk adolescents given the popularity of smartwatches [13]. A critical gap in current research is to identify changes in HRV during acute suicidal episodes in adolescents.
With that in mind, the objective of this study was to identify correlations between the HF component of HRV and severity of suicidality in a cohort of acutely suicidal, inpatient adolescents. Based on evidence from prior literature [11,12], we hypothesized that the primary predictor of HF metric would be inversely correlated with the primary outcome of Columbia Suicide Severity Score (CSSRS). Measuring HRV using wearable technology has the potential to be widely implemented and facilitate earlier detection of suicidal symptoms before they reach a crisis level among a large number of atrisk adolescents. This creates the ability to provide early detection and intervention, potentially reducing ED recidivism, acute hospitalizations and suicide attempts.
METHODS
This was a prospective, observational study from September 2017 thru November 2019 in a tertiary care pediatric emergency department and an inpatient pediatric psychiatric unit. These 2 locations are within different hospital systems, but located in close geographic proximity. The tertiary care children’s hospital where the emergency department is housed does not have an inpatient psychiatric unit, so many patients requiring admission are transferred to the enrolling inpatient pediatric psychiatric unit. Patients were eligible if they were between the ages of 13–19 years and presented to the ED or were admitted to the inpatient psychiatric unit for acute suicidality. Admission to the psychiatric facility was determined by the treating psychiatry team unrelated to the study. The indication for admission in this population is generally risk of self-harm and need for acute psychiatric interventions. Patients were excluded if they were in the Oregon Department of Human Services custody, acutely agitated as deemed by the primary medical team, were pregnant, had an initial CSSRS <4 (not suicidal), or had insufficient data quality for analysis. Acutely agitated patients were excluded due to the concern for self-harm with a study device and danger to the study team. The study was approved by the Institutional Review Board at both sites and registered with clinicaltrials.gov (NCT03030924). Informed consent was obtained from the patient or legal guardian and assent was obtained from patients <18 years.
Heart rate variability data collection
HRV data was collected from a wrist-worn device specifically developed for the study that the patient wore for 7 days while it continuously collected photoplethysmography data. HRV data requires beat detection at a consistent point in the cardiac cycle creating a situation where motion artifact is problematic. While prior literature using ECG has used longer durations of time [11,12], extended artifact-free data sets are difficult to achieve with wrist worn devices. The goal was therefore to obtain 1 minute tracings of artifact-free data each hour. Python 3 HRV-Analysis version 1.3 package available from pypi. org processed the photoplethysmography data. Artifact free data was defined as 1-minute segments at the start of every hour free of outliers and ectopic beats. If multiple artifact-free segments were available for a specific hour, the segment that was closest to 60 minutes from the prior segment and 60 minutes to the following segment was selected by the processing algorithm. This was to achieve the goal of 60 minutes between segments but ensuring artifact-free data. The optical signal was created and detected by an OSRAM SFH 7070 (Osram Opto Semiconductors Inc.). This combination optical detector and source includes two green (635 nm) photodiodes that flank the photodetector. The current through the photodiodes is controlled by a Texas Instruments AFE 4044, which also detects the output of the photodetector at 300 Hz using a 23-bit sigma delta converter with ambient light cancellation. All data were stored locally on the device until the study team received it back from the patient. The device data were uploaded and then filtered to remove baseline wander, such as that which occurs due to respiration, and the beats were detected using the Automatic Multiscale Peak Detection (AMPD) algorithm [14]. All waveforms and beat selections were manually reviewed by the study team prior to analysis to ensure artifact-free data (Figure 1).

Beat to beat detection.
Outcomes
At the time of enrollment, demographic data, including past history of an ED visit or inpatient admission for suicidality, formal mental health diagnoses of depression, suicidality or anxiety, daily psychotropic medications taken, gender, age, past non-mental health medical history were collected. Suicide severity was measured by the Columbia Suicide Severity Scale (CSSRS), which has been validated in suicidal adolescents [15]. To assess the relationship between HRV and suicidality, the CSSRS initial intake scale was administered at the time of enrollment. This scale was scored on a continuous scale, as done in prior adolescent ED suicide research [15]. The potential score breakdown by subsection was: suicidal ideation 0–5, intensity of ideation 3–25, and suicidal behavior 0–5 for a possible composite score of 0–35. A research coordinator followed up with the patients in the inpatient unit and administered the CSSRS scale at midweek (defined as day 3 or 4) and 7. If a patient was discharged from the hospital or ED prior to completion of the 7 days, they were able to continue wearing the device at home and still completed the Columbia Suicide Severity follow-up scales at midweek and 7.
Statistical methods
Descriptive statistics were calculated for demographic variables, including age, gender, previous admission to a psychiatric facility, previous ED visit for suicidality, days between enrollment in the study and ED visit, attempted self-harm for the current visit, location of enrollment and final assessment (inpatient or home). All data were examined for normality and transformed, as needed. HRV measurements were examined for outliers and across all raw HRV values we removed the highest 1% of data.
To assess for adjusted differences in sqrt (HF) we conducted multiple regression. The primary predictor was the power of sqrt (HF) component on the primary outcome of CSSRS. Analyses were performed at a single point in time (first or second HRV measurement), during Day 1 of the study, or across all days with available data. A CSSRS of 15 or greater was used as a dichotomous variable, because it is approximately 50% of the total composite score and felt by the study team to most likely indicate a patient with significant suicidality. The second way was to identify the correlation between changes in the HF power and changes in CSSRS over time, which allows future work around HRV to be used as a diagnostic tool to monitor for improvement in suicidal behavior. Because patients were actively undergoing treatment outside the study, we aimed to identify HF correlations as the CSSRS improved. To assess suicidal severity changes over time, in particular improved symptoms, a decrease in the Columbia Suicide Score of 25% between 2 times points was used. Covariates included patient gender, age, prior suicide attempts, days between the ED visit and study enrollment, location of enrollment, hour of the day and circadian rhythm. We controlled for circadian rhythm, as previously described, in which the hour of the day was converted to angular format (radians) and then converted to trigonometric format via a Fourier transform pair (sine and cosine) [16].
The pragmatic use of this data is to identify high risk patients at time of measurement of HRV, but also to monitor for changes over time. A higher CSSRS correlated to increased suicide severity, while a decrease over time suggests reduced suicidality during the study time period. To control for the clustering of repeated measurements within a patient, for all models with more than one measurement per patient, we used mixed effects models with a random effect for patient. To assess model fit, we examined QQ plots, plots of residuals, and influence statistics. We performed a sensitivity analysis using only nighttime data (10 pm–6 am) as the data quality was expected to be much higher with decrease movement while people slept. The overall analysis goal was to evaluate correlations in HF power with CSSRS in 2 ways: The first was to use HF power to distinguish patients with a higher CSSRS from those with lower; this would allow future work around HRV as a diagnostic tool when patients first present to a clinician. The second was to evaluate correlations in changes of HF power with changes in CSSRS over time; this would allow future research around the utility of HRV as a monitoring tool for patients outside the hospital setting.
RESULTS
There were a total of 104 acutely suicidal adolescents enrolled in this study. As detailed in Figure 2, after exclusions, the final cohort consisted of 51 patients. The average age was 16.7 years (stdev 1.5 years) with a predominance of females (72.6%). Almost half of patients (47.1%) had a previous ED visit for a mental health complaint or inpatient psychiatric hospitalization. The majority (60.8%) were enrolled after presenting to the hospital following a suicide attempt. The patients were enrolled equally between the ED and inpatient psychiatric unit (45.1% vs. 54.9% respectively) and approximately half remained inpatients at the time of study completion 7 days after enrollment (Table 1). The majority of patients had CSSRS (69.4%) greater than or equal to 15. Figure 3 visualizes the percentage change of CSSRS from time of initial enrollment with the majority showing improvement as evidenced by a negative change. A decrease in CSSRS indicates improvement in their suicide severity.
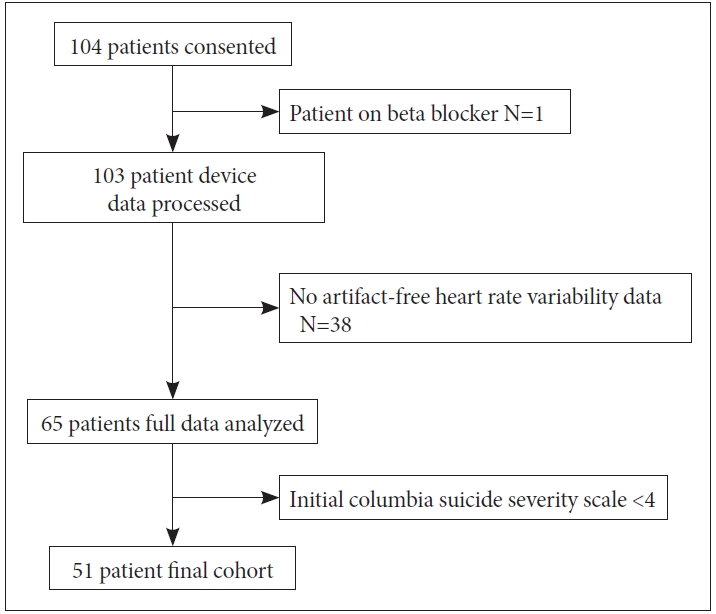
Final cohort enrollment.
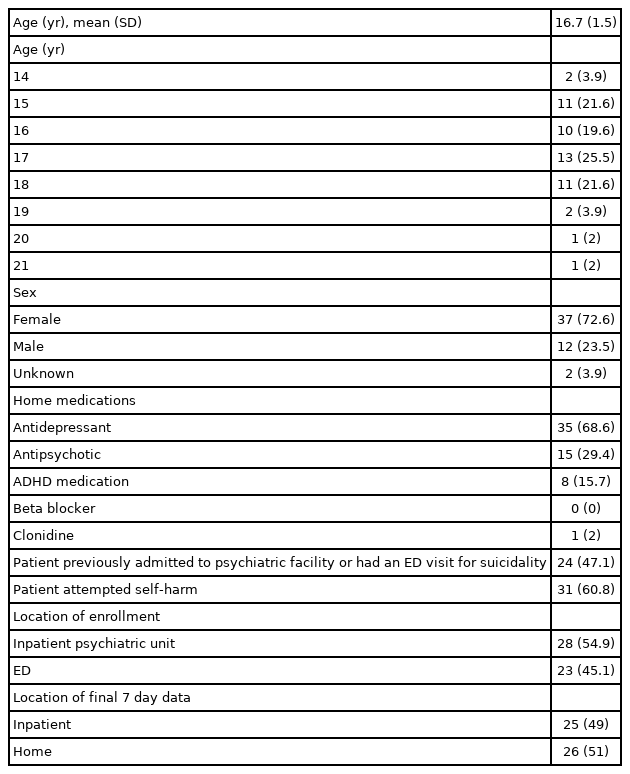
Patient and enrollment characteristics (N=51)
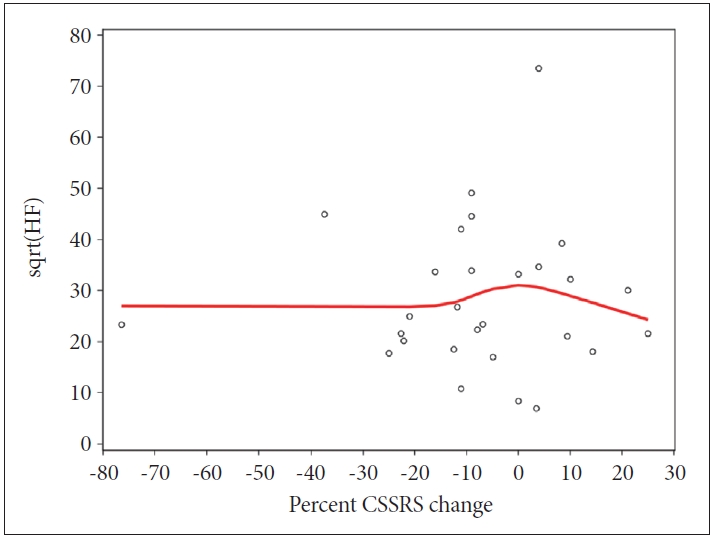
Columbia suicide score change over time. CSSRS, Columbia Suicide Severity Score (negative is a decrease in score, ie. Improved suicide severity); sqrt(HF), square root of the high frequency component.
There were a total 1,215 HRV segments across 51 patients available for analysis across all days, and 697 HRV segments available across 51 patients on day 1. Model fit was acceptable for all regression models. Due to heteroskedastisicity, we used a sandwich estimator for variance in all models. No outliers or leverage values were identified. To accomplish the study objective, HRV measurements were focused on the transformed sqrt (HF). Tables 2 and 3 detail the association between HF and CSSRS as assessed by the regression models including both the initial CSSRS and HF and change in CSSRS and HF HRV during the study period (a decrease of at least 25% during the study period). Among patients who had a second CSSRS (29 of the 51 patients), approximately one quarter of patients (n=7) had a 25% decrease in the CSSRS after the initial enrollment. This resulted in 478 HRV measurements during all hours and 177 HRV measurements at nighttime. The sqrt (HF) component significantly increased over time in patients that had at least a 25% decrease in their CSSRS (nighttime mean difference 11.89 ms/

Adjusted association of heart rate variability with suicidality
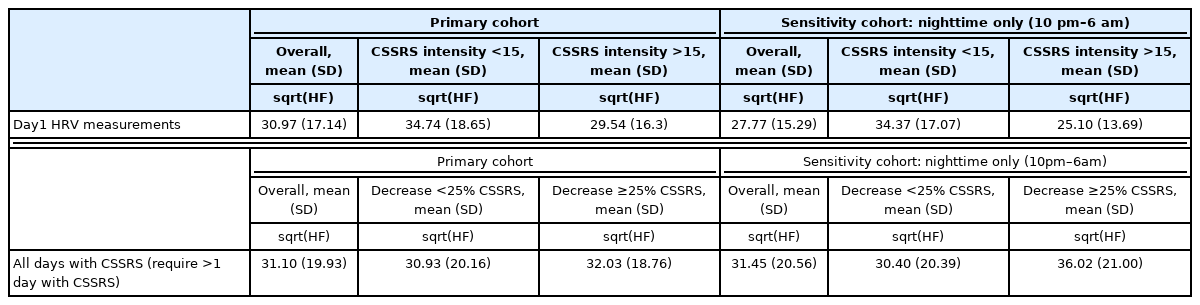
Unadjusted sqrt(HF) measurements
DISCUSSION
This novel study was consistent with our hypothesis and found a significant negative association between the HF power, which measures the parasympathetic branch of the autonomous nervous system, and the CSSRS in a population of acutely suicidal adolescents using a wearable technology. This finding indicates that increasing suicidality is associated with decreased parasympathetic tone. The lifetime prevalence of a suicide attempt in adolescence is currently over 20% [17]. For this reason, suicide prevention is a critical national public health priority especially among adolescents [18]. This study addresses the large unmet need and uses an innovative approach to meet this challenge. A socially-acceptable, easy-to-use technology that is continuously available to measure HRV at various points in the day, such as smartwatches, should be evaluated as a tool to identify worsening parasympathetic function, and associated suicidality, in real time. This would allow for preventive measures to be implemented when needed such as biofeedback or coping skills to decrease suicide attempts, suicide-related ED visits, and suicide-related mortality. The smartwatch is a wearable biosensor platform that has high social acceptability among adolescents, allowing discreet monitoring that would not be embarrassing or associated with increased stigma from peers.
The rationale for this work stems from previous cross-sectional studies evaluating HRV in patients with mental health problems as a biomarker of the autonomic nervous system; in particular parasympathetic activity through the HF power of HRV. Across multiple study designs and research teams, the findings have consistently found an association between the HF and suicidality [12,19,20]. These studies have found that the HF power was lower in patients with worse depression and suicidality or a history of suicide attempts compared to normal patients. Our study is unique in that it was conducted among acutely suicidal patients, used photoplethysmography to measure HRV, and included longitudinal measurements.
One significant clinical impact wearable technology that monitors physiologic parameters, such as HRV, can have is to identify dynamic changes in suicidality beyond single timepoint measurements. Previous studies have investigated more dynamic changes in HRV by using stress-inducing tasks in the laboratory setting while monitoring HRV. A large systematic review in adults included studies measuring HRV during stressful situations in patients with clinical depression [21]. These studies focused on well-validated stress tasks and generally found that among depressed individuals, there was hypo-reactivity of the parasympathetic system during stressors, as evidenced by lower HF power. One study attempted to evaluate both resting HRV and stress-induced HRV’s relation to active suicidal ideation [22]. They found decreased HF power was predictive of higher suicide severity scores. Another study examined changes in the HF HRV power during a stress-induced task and differentiated suicide attempters from suicide ideators without an attempt [11]. This type of research is pivotal to the clinical hope of identifying the latter group before progressing to a suicide attempt. In that study, while there were no differences between groups in anger and stress measures at baseline, following a social stressor, they found that attempters had a lower HF during the stress test than non-attempters. These studies corroborate our findings of lower HF HRV being associated with increased severity of suicidality.
While several studies have shown a significant inverse correlation between the HF and depression/suicidality in laboratory settings, this study is significant in that it found similar results in acutely suicidal adolescents admitted to the hospital or ED. The next phase to this area of research would be to intermittently measure HRV longitudinally and as part of a system to alert patients and their loved ones to autonomic dysregulation and higher risk of increasing suicidality. There are several potential interventions patients could implement upon receiving an alert. One area of research has focused on the impact of biofeedback, such as breathing, targeted to change HRV in patients with mental health disorders [23-25]. This could be employed using a mobile application in conjunction with an alert for worsening HF HRV. Previous studies have shown the ability to utilize biofeedback guided by dynamic changes in HRV resulting in improved overall symptoms [24,26,27]. Wearable technology, especially in conjunction with smartphones, can also collect other biosignals and monitor other elements of behavior that could be incorporated into machine learning applications to improve the predictive ability of an algorithm [28,29].
This pilot study has similar findings to past literature, but does have a number of limitations. As detailed in Figure 1, we excluded a number of patients due to poor data quality. The majority of excluded patients were at the beginning of the study while the technical aspects of the study PPG device were evaluated in adolescent suicidal patients. After identification of technical issues, the remaining enrollments resulted in improved data quality. Accurate measurements of HRV need relatively long segments of artifact-free data. Notably, the majority of data collection problems were during the initial phase of the study, while the usability and other device features were being optimized such as how tight the wristband needed to be secured to the wrist. There was a higher proportion of available nighttime data (63.3% vs. 43.0% of hourly segments on day 1) compared to daytime, which highlights the impact of motion. The inverse correlation was found in both nighttime only and all hours, but stronger at night. This may be secondary to better quality data or inherent circadian rhythm, although this was controlled for. This study focused on the HF HRV data, but other HRV metrics that focus on vagal tone as demonstrated in prior studies should be evaluated in a larger sample size to confirm or refute the findings of this pilot study [30,31]. Another limitation is that we limited our HRV-analysis segments to one-minute intervals of artifact-free data. This is different from past studies that have collected data over longer periods of time, but was necessary to obtain precise HRV measurements in a real-world scenario using PPG. Our study design used a validated, clinical standard (Columbia Suicide Severity Score) as a measure of suicide severity. However, there is inherent subjectivity to this score, and it begs the question if some patients answer falsely to try and leave the hospital sooner with low scores. We believe this is lower likelihood as patients were explicitly told by the research team that their results would not directly change clinical care. It is noteworthy that we excluded a small number of patients who had extremely low scores on their baseline CSSRS, even though they were admitted for acute suicidality. The dichotomous clinical cutoffs we chose for analysis were to detect relatively large clinical changes. However, it may be of interest in the future to detect smaller changes in suicidality that can be accomplished with larger studies. Lastly, we did not enroll a cohort of healthy controls in our study, as each patient served as their own baseline to compare their changes to over the week study period. Future studies evaluating a single baseline measurement should include healthy controls or patients with a mental health history who are not currently suicidal.
This pilot study in acutely suicidal adolescents showed a statistically significant inverse correlation between the HF HRV and CSSRS measured by photoplethysmography using a wrist-worn device. This association was found both in comparisons using a single point in time, as well as when analyzed as a change over time. Given that many adolescent patients have a repeat visit to the ED or suicide attempt after an initial visit, the ability to detect worsening suicidality in this high-risk population may have positive impacts on patient outcomes and the healthcare system. Further research will need to confirm this relationship in larger cohorts of acutely suicidal adolescents.
Notes
Availability of Data and Material
The datasets generated or analyzed during the study are available from the corresponding author on reasonable request.
The authors have no potential conflicts of interest to disclose.
Author Contributions
Conceptualization: David C. Sheridan, Steven Baker, Matthew Hansen. Data curation: David C. Sheridan, Steven Baker, Ryan Dehart, Nancy Le. Formal analysis: Amber Lin. Funding acquisiton: Craig D. Newgard, David C. Sheridan. Investigation: David C. Sheridan, Nancy Le. Methodology: David C. Sheridan, Matthew Hansen, Steven Baker, Larisa G. Tereshchenko, Bonnie Nagel. Project administration: Nancy Le. Resources: David C. Sheridan. Software: Ryan Dehart, Steven Baker. Supervision: Craig D. Newgard, Bonnie Nagel. Validation: David C. Sheridan, Amber Lin. Writing—original draft: David C. Sheridan. Writing—Reviewing and editing: all authors.
Funding Statement
This was funded by the National Institute of Mental Health K12 award; Oregon Care Emergency Care Research MultiDisciplinary Training Program Award#5K12HL133115.