Real-World Evidence for the Association Between Pneumonia-Related Intensive Care Unit Stay and Dementia
Article information

Abstract
Objective
There is limited clarity concerning the risk of dementia after pneumonia with intensive care unit (ICU) stay. We conducted a nationwide cohort study, which aimed to investigate the impact of dementia after pneumonia with and without intensive care unit admission.
Methods
Data was obtained from Taiwan’s National Health Insurance Research Database between 2000 and 2015. A total of 7,473 patients were identified as having pneumonia required ICU stay, along with 22,419 controls matched by sex and age. After adjusting for confounding factors, multivariate Cox regression model analysis was used to compare the risk of developing dementia during the 15-years follow-up period.
Results
The enrolled pneumonia patients with ICU admission had a dementia rate of 9.89%. Pneumonia patients without ICU admission had a dementia rate of 9.21%. The multivariate Cox regression model analysis revealed that the patients with ICU stay had the higher risk of dementia, with a crude hazard ratio of 3.371 (95% confidence interval, 3.093–3.675; p<0.001).
Conclusion
This study indicated that pneumonia with ICU stay is associated with an increased risk of dementia. A 3-fold risk of dementia was observed in patients admitted to the ICU compared to the control group.
INTRODUCTION
Pneumonia is the leading cause of morbidity and mortality Print ISSN 1738-3684 / On-line ISSN 1976-3026 OPEN ACCESS in the world, and was the third leading cause in Taiwan in 2017 [1]. It is a common infectious respiratory disease diagnosed based on clinical symptoms, physical signs, and chest radiographs. Majority of pneumonia patients can be treated as outpatients, and only less than 1% require hospitalization, or intensive care unit (ICU) admission [2]. Dementia is a progressive and incurable disorder characterized by decline in cognition [3,4]. In Taiwan, pneumonia becomes a heavy burden for the patient’s families, caregivers, communities, and the society [5,6].
Elderly pneumonia patients have functional and cognitive impairment [7,8]. ICU stay can influence the outcome of cognition [9]. Pneumonia resulting in ICU admission can lead to impaired cognition. One study has found that hospitalization with pneumonia, even in the well-functioning older adults is associated with increased risk of dementia [10]. Several studies have revealed the increased subsequent risk of cognitive function impairment or dementia in the critical settings. Another study has shown that, in a one-year follow up of 80 pneumonia patients who were hospitalized, moderate-to-severe impairment in multiple cognitive domains affected one-third of the patients aged ≥65 years and 20% of the younger patients (age <65 years), and another third of survivors had mild cognitive impairment. The most often noted cognitive deficits occurred in visuospatial function, attention, and memory [11]. A study in Sweden pointed out that older age and severity of acute illness, the severity of comorbidities, and the length of ICU and hospital stay were independent risk factors for the development of dementia. Although dementia is common among patients with sepsis with ICU stay, sepsis was not an independent risk factor [12]. Lastly, a study in Taiwan found that the risk of dementia, for the patients with acute respiratory failure who required the mechanical ventilations, increase with age and are higher in women than in men [13].
However, there is no clarity concerning the relationship between pneumonia with and without ICU admission for the risk of dementia. We hypothesize that pneumonia with ICU stay has synergistic effect on the risk of dementia. Therefore, this retrospective cohort study explores the risk of dementia after pneumonia with ICU stay.
METHODS
Data sources
In Taiwan, the National Health Insurance (NHI) was launched in 1995. As of June 2009, it had included contracts with 97% of medical services with approximately 23 million beneficiaries, or more than 99% of the entire population [14]. The details of this program were documented in several previous studies [6,15-29]. The National Health Insurance Research Database (NHIRD) contains comprehensive data of the beneficiaries. Individual identifies were encrypted before release for research under the Personal Information Protection Act.
The NHIRD used the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes to record diagnoses. All dementia diagnoses were made by board-certified psychiatrists or neurologists. The presence of pneumonia was confirmed by clinical, laboratory, and imaging findings. Further, all types of pneumonia were included. The licensed medical record technicians verified the coding before claiming the reimbursements in hospitals and clinics. The NHI Administration appointed several experts for randomly reviewing the records of ambulatory care visits and inpatient claims to verify the accuracy of the diagnoses. In this study, we used the data from the Longitudinal Health Insurance Database (LHID) (2000–2015), a subset of the NHIRD, to investigate the association between pneumonia with an ICU stay and dementia over a 15-year period.
Ethical approval
This study was approved by the Institutional Review Board of the Tri-Service General Hospital (TSGH IRB No. 2-107-05-026). As patient identifiers were encrypted before their data were used for research purposes to protect confidentiality, the requirement for written or verbal consent from patients for data linkage was waived.
Study design and participants
This study used a matched-cohort design. From the LHID, we enrolled the patients diagnosed with pneumonia with ICU admission between January 1, 2000 and December 31, 2015. Pneumonia patients with ICU stay or dementia before 2000, lung abscess, empyema, and those <50 years of age were excluded (Figure 1A). All the ICD codes were listed in the Supplementary Table 1 (in the online-only Data Supplement). We identified 1:3 study subjects and controls without ICU admission (n=7,473 and n=22,419, respectively) in a frequencymatch for sex, age, and index year. The statistical power is up to 0.875.
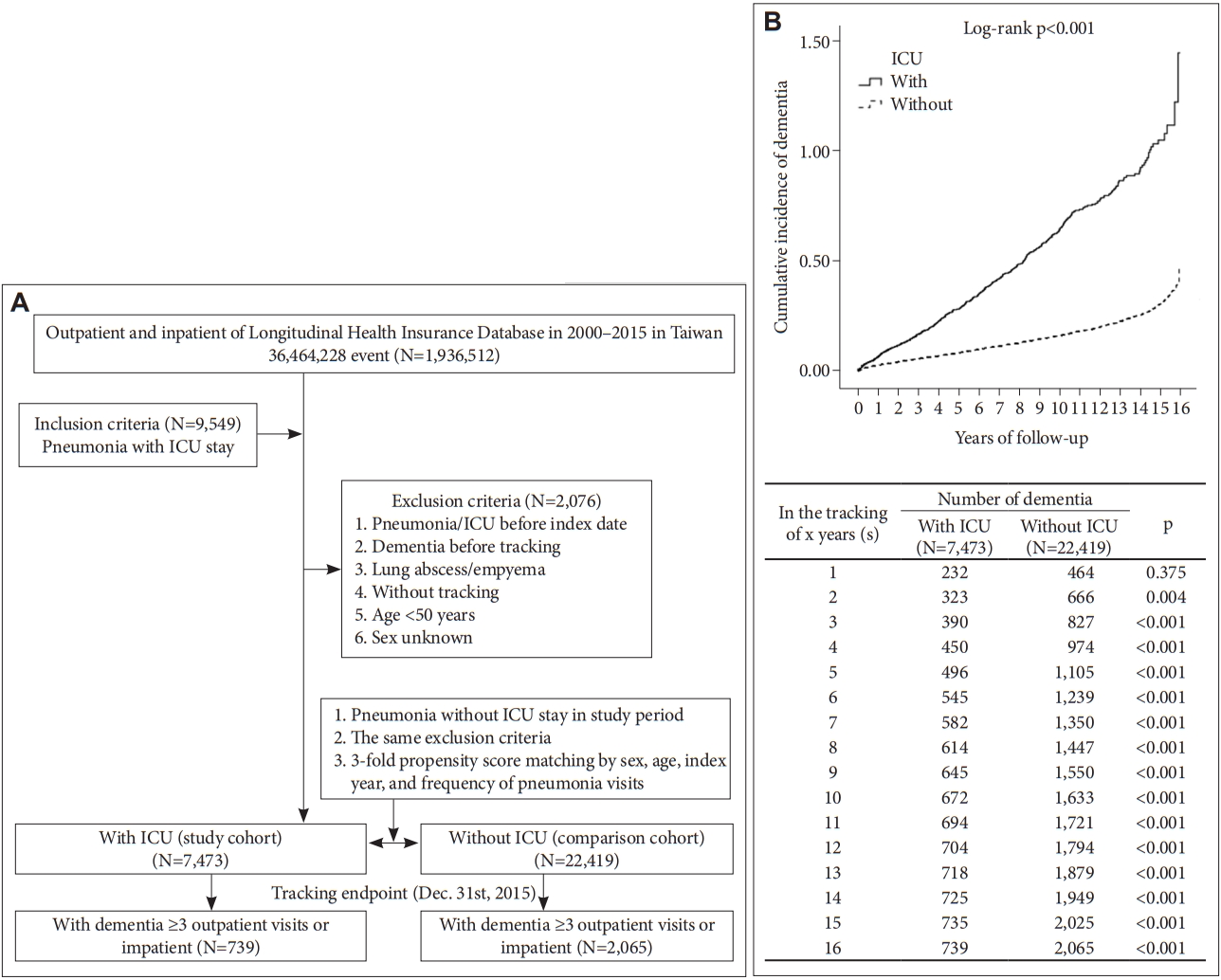
A: The flowchart of study sample selection. B: Kaplan–Meier for cumulative incidence of dementia among pneumonia patients aged 50 and over stratified by intensive care unit (ICU) with log-rank test.
Covariates and comorbidity
Covariates included sex, age group (50–64, ≥65 years), season (spring, summer, autumn, and winter), geographic area of residence (north, center, south, and east of Taiwan), level of care (medical center, regional, and local hospital), monthly insurance premium (in New Taiwan Dollars [NT$]: <18,000, 18,000–34,999, and ≥35,000), and urbanization level of residence (level 1–4). The urbanization level of residence was defined by the population, along with various indicators of the level of political, economic, cultural, and metropolitan development. Urbanization level 1 was defined as a population over 1,250,000 with a specific designation as political, economic, cultural, and metropolitan development. Level 2 was defined as a population between 500,000 and 1,249,999, which played an important role in the political system, economy, and culture. Levels 3 and 4 were defined as a population between 149,999 and 499,999, and <149,999, respectively [30].
The selected comorbidities were based on the patient’s data: hypertension (HTN), diabetes mellitus (DM), atrial fibrillation (AF), stroke, cerebral atherosclerosis, other atherosclerosis, fracture of lower limbs, cancer, asthma, chronic obstructive pulmonary disease (COPD), bronchiectasis, idiopathic pulmonary fibrosis (IPF), coronary artery disease (CAD), acute respiratory failure, acute kidney injury (AKI), chronic kidney disease (CKD), hemodialysis (HD), obesity, liver cirrhosis, heart failure (HF), ventilator dependency, and immunocompromised conditions. The ICD codes of comorbidities were listed in the Supplementary Table 1 (in the online-only Data Supplement). The Charlson Comorbidity Index, dementia re moved (CCI_R), HTN, DM, AF, stroke, cerebral atherosclerosis, other atherosclerosis, cancer, COPD, bronchiectasis, IPF, CAD, acute respiratory failure, AKI, CKD, liver cirrhosis, and HF.
Study outcomes
Individuals from the study were followed from the index date until the onset of overall dementia, withdrawal from the NHI program, or until the end of year 2015. The study subjects were grouped as having Alzheimer dementia (AD), vascular dementia (VaD), and other degenerative dementia. The ICD codes of dementia were listed in the Supplementary Table 1 (in the online-only Data Supplement).
Statistical analysis
All statistical analyses were performed using the SPSS software version 22 (IBM Corp., Armonk, NY, USA). χ2 and ttests were used to evaluate the distribution of categorical and continuous variables, respectively, using the Fisher’s exact test. Multivariate cox proportional hazard regression analysis was used to determine the risk of dementia, since death can act as a competing risk factor. The results were presented as a hazard ratio (HR) with 95% confidence interval (CI). The differences in the risk of dementia between the study and control groups were estimated using the Kaplan–Meier method with the log-rank test. A two-tailed p value<0.05 was considered as statistical significance.
RESULTS
Baseline characteristics
The cohort study comprised pneumonia patients with ICU stay (n=7,473) and without ICU stay (n=22,419). The study revealed the proportion of outcomes among exposure groups concerning sex, age, marital status, education, insured premium, comorbidities, frequency of pneumonia visit, season, area of residence, urbanization, and level of care. Compared with control group, ICU stay patients tended to have higher rate of stroke, cancer, acute respiratory failure, CKD, liver cirrhosis, ventilator dependency, HD, as well as a higher CCI_R. However, ICU stay patients had a lower proportion of HTN, DM, other atherosclerosis, fracture of lower limbs, COPD, bronchiectasis, CAD, and HF. Considering the season, location, urbanization level, and level of care, the ratio was higher among summer and autumn, northern and southern Taiwan, highest (level 1) urbanization level, and medical center and regional hospital, respectively, in the ICU group (Table 1).

Characteristics of participants at the baseline
Kaplan–Meier model for the cumulative risk of dementia
There were 739 individuals out of 7,473 (9.89%) with development of dementia in the study group. Development of dementia was observed among 2,065 individuals out of 22,419 (9.21%) in the control group. The Kaplan–Meier analysis for the cumulative incidence of dementia in the study and control groups was significant (log rank p<0.001; Figure 1B).
The risk of dementia for the patients with pneumonia with intensive care unit stay
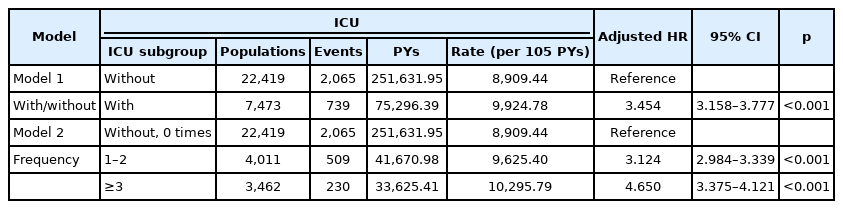
The multivariable Cox proportional regression analysis showed the association with the risk of developing dementia (Table 2). The crude HR was 3.371 (95% CI, 3.093–3.675; p< 0.001). After adjusting sex, age, comorbidities, frequency of pneumonia visits, season, urbanization level of residence, and level of care, the adjusted HR was 3.454 (95% CI, 3.158–3.777; p<0.001). Similarly, male sex, old age, HTN, DM, stroke, cerebral atherosclerosis, cancer, CAD, AKI without HD, liver cirrhosis, HF, and ventilator dependency were associated with higher risk. Further, no difference was observed with the complication of CCI_R.

Factors for risk of dementia by using multivariable Cox proportional regression model
Sensitivity analysis
With regard to the frequency of ICU stay, the adjusted HRs of patients with pneumonia with an ICU stay of one or two admissions and ≥3 admissions were 3.124 (95% CI, 2.984– 3.339; p<0.001), and 4.650 (95% CI, 3.375–4.121; p<0.001), respectively, in comparison with that of the control group. The frequency of pneumonia visits ≥3 times also had higher risk compared to 1–2 visits. Besides, autumn, urbanization level 1, 2, medical center, and regional hospital were associated with an elevated risk compared to the control group, with the exception of urbanization level 3 (Table 3).
Factors of dementia in different models by using the multivariate Cox regression analysis
Subgroup analyses
A subgroup analysis was also performed. The assessment of dementia risk according to sex, age group, monthly premiums, comorbidity status, seasons of treatment, urban levels and the areas of residence, and the levels of medical care are shown in Table 4. In the majority of groups formed based on sex, age, monthly premiums, seasons of treatment, urban levels and the areas of residence, and levels of medical care, patients with pneumonia with ICU stay had a higher risk of dementia, compared with the controls, with the exception of patients with monthly insured premium ≥35,000 NT$. In addition, the majority of comorbid and non-comorbid patients, antidepressant users had a higher risk for dementia compared with the controls, with the exception of subjects without obesity (Table 4).

Subgroup analysis for the risk of dementia
Types of dementia after pneumonia with intensive care unit stay
Concerning the types of dementia, the adjusted HRs of pneumonia with ICU stay were 5.209, 2.913, and 3.381, in AD, VaD, and other degenerative dementia, respectively (all the p< 0.001) (Table 5). Despite excluding dementia occurred in the first 2 years after ICU admission, every type of dementia in the study groups were associated with higher risk than the controls. Especially in the AD group, the adjusted HR was up to 7.222 (p<0.001).

Factors of dementia subgroup and sensitivity analysis by using Cox regression
DISCUSSION
Pneumonia, intensive care unit stay and the risk of dementia
The present study has several noteworthy findings. First, in a 15-year follow-up, it was observed that the subjects with pneumonia with ICU stay had a nearly three-fold increased risk of developing dementia, compared with the controls. Second, ICU stay is associated with the risk of different types of dementia, including the AD, VaD, and other degenerative dementia. Third, the Kaplan–Meier analysis showed that a 2-year period was required to achieve significant adjusted HR until the end of follow-up. Fourth, we found that several comorbidities were associated an increased risk of dementia, including the sensitivity analysis which revealed that even though we excluded dementia that occurred in the first 2 years after ICU admission, the study groups were still associated with a higher risk compared to the rest. Fifth, we found that more ICU stays were associated with higher risk of developing dementia. To the best of our knowledge, this is the first nationwide, matched cohort study that focused on the association between pneumonia with ICU stay and the risk of dementia.
We found that subsequent dementia among pneumonia patients was positively associated with the male sex and older age. This finding was consistent with the findings of previous studies: a previous cohort study revealed the pneumonia in creased the risk of dementia [11]. However, the present study has several unique points: First, we focused on the patients with pneumonia and ICU stay, compared to the previous study findings which focused on the association between ICU stay and dementia [10,12,13,31]. Second, we conducted subgroup and sensitivity analysis to support this association. Third, we also found that the number of times of pneumonia-related ICU stay, comorbidities, the season wherein pneumonia was treated, the urbanization level, and level of care, were independently associated with the risk of dementia.
Possible mechanisms for the increased risk of dementia in charcoal-burning suicide attempters
The mechanism by which pneumonia patients who were admitted in an ICU had higher cases of dementia, compared to the control, remains unclear. Pneumonia-related hypoxia may contribute to subsequent cognitive impairment, as it induces oxidative stress and neuronal apoptosis, especially in the hippocampus and cerebellum, which are more sensitive to hypoxia [32-34]. Moreover, pneumonia could trigger the release of inflammatory cytokines [35], which lead to neurodegenerative changes [36,37]. Other mechanisms attributable to pneumonia call also influence cognition [38]. Delirium is another issue that worsens long-term global cognition and executive function. It is easily noted with patients with ICU stay, since delirium could predispose the patients to long term cognitive impairment associated with inflammation and neuronal apoptosis [39,40]. Further studies are needed to investigate the association between pneumonia with ICU admission and dementia. In addition, the ill health of the patients in the ICU might contribute the risk of dementia [10,12,13,31].
Types of dementia
In this sample, 2,804/29,892 enrolled subjects (9.38%) had developed dementia including 739/7,473 in the study group (9.89%) and 2,065/22,419 (9.21%) in the controls. The prevalence around 2%–5% for the population aged >65 years in the community studies [41]. Whether ICU stay or not, it revealed the prevalence of patients with pneumonia beyond the average, and aggravated with ICU admission. In Taiwan, several previous studies disclosed that AD was the most common type of dementia, accounting for 40%–60% of all dementias, followed by VaD, and degenerative dementia, which account for 20%–30% and 7%–15% of all dementias, respectively [42,43]. The results reflected the higher risk among AD, VaD, and other degenerative dementia, especially in the AD group. Furthermore, the risk of AD increased significantly, around 7-fold, in the sensitivity analysis. This study finding potentially suggest that ICU stay and pneumonia might hasten the development of dementia in the future.
Socioeconomic factors in the risk of dementia in pneumonia with intensive care unit stay
Our study showed that urbanization level might influence the risk of dementia. The urbanization level 1–3 had the lower risk than level 4, and the results were consistent with those obtained in previous study [44-46]. There were many possible factors, which may have led to dementia, including education [44], living environment [45], air pollution, and noise pollution levels [46]. We also found the level of hospital would also influence the risk of dementia. Patients that lived in the hospital center or regional hospital were at a higher risk of dementia than those in the local hospital.
Strengths of this study
This study had several strengths: First, the diagnosis of pneumonia [47] in the NHIRD has had been previously validated, as well as the validation of several other respiratory diseases, such as asthma [48], sleep apnea [47], and tuberculosis49 has been conducted. Second, one previous study has validated the diagnoses of psychiatric disorders in the NHIRD [50].
Limitations of this study
Limitations of this study The study had some limitations: First, we used ICD-9 code to identify pneumonia, however, previous study showed a reasonable accuracy [51]. Second, patients diagnosed with dementia were identified from the insurance claims data. Nevertheless, data on severity stage and the impact on their caregivers were not available. Types of dementias were indemnified from the ICD codes in these claims data. Third, in this claims dataset, there are no records for the differentiation the community-acquired from nosocomial pneumonia. Fourth, even though only newly diagnosed dementia wound be included in the follow-up period, a protopathic bias, wherein the initiation of an exposure occurred in response to an undiagnosed disease under study, should also be considered since some of the patients with pneumonia had cognitive decline prior to their ICU stay. Finally, the baseline of cognitive function of patients is lacking. Although we used a model to identify dementia occurred in first 2 years, the model could not be completely related to the point of mild cognitive decline before the screening.
In conclusion, pneumonia patients with ICU stay are at a three-fold risk of the development of dementia compared to patients in the control group. Therefore, further studies to elucidate the mechanisms underlying this association are needed.
Supplementary Materials
The online-only Data Supplement is available with this article at https://doi.org/10.30773/pi.2021.0277.
ICD-9-CM codes of the diagnosis
Notes
Availability of Data and Material
Data are available from the National Health Insurance Research Database (NHIRD) published by the Taiwan National Health Insurance (NHI) Administration. Due to legal restrictions imposed by the government of Taiwan in relation to the “Personal Information Protection Act”, data cannot be made publicly available. Requests for data can be sent as a formal proposal to the NHIRD (https://dep.mohw.gov.tw/dos/np-2497-113.html ).
Conflicts of Interest
The authors have no potential conflicts of interest to disclose.
Author Contributions
Conceptualization: all authors. Data curation: all authors. Formal analysis: Wu-Chien Chien, Chi-Hsian Chung. Funding acquisition: all authors. Investigation: all authors. Methodology: all authors. Project administration: all authors. Resources: Chung-Kan Peng, Wu-Chien Chien, Nian-Sheng Tzeng. Software: Chi-Hsian Chung. Supervision: Chung-Kan Peng, Nian-Sheng Tzeng. Validation: Nian-Sheng Tzeng. Visualization: Chi-Hsian Chung. Writing—original draft: Chun-Han Wu. Writing—review & editing: Chung-Kan Peng, Nian-Sheng Tzeng.
Funding Statement
This work was supported by the Medical Affairs Bureau, the Ministry of Defense of Taiwan (MAB-107-084 and MNDMAB- D-111-075), the TriService General Hospital Research Foundation (TSGH-C108-003, TSGHC108-027, TSGH-C108-151, TSGH-B-109-010, TSGH-B-111-018, and TSGH-D-111-121), and the Taoyuan Armed Forces General Hospital (TYAFGH-A-110-020).