Suicide Risk in Patients With Diabetes Varies by the Duration of Diabetes: The Korea National Health and Nutrition Examination Survey (2019)
Article information

Abstract
Objective
The objectives of this study were to investigate the suicide risk in diabetes patients and evaluate the variations in suicide risk by the duration of diabetes using a large population sample in South Korea.
Methods
Data from 6,296 adults in the 2019 Korea National Health and Nutrition Examination Survey were included. The suicidal ideation, suicide plans, and suicidal behavior of diabetes patients were compared to the general population. After classifying the patients into ≤1 year, 2 to 9 years, and ≥10 years of diabetes duration, we evaluated the relationship between the duration of diabetes and the suicide risk.
Results
Diabetes patients had higher prevalences of suicidal ideation (9.1%, p<0.001) and suicide plans (3.6%, p<0.001) than the general population. After adjusting for potential confounding factors, suicide plans (adjusted odds ratio [aOR]=2.926, 95% confidence interval [CI]=1.325–6.463) were significantly associated with diabetes. In the 2 to 9 years group of diabetes patients, we found an increase in the risk of suicidal ideation (aOR=2.035, 95% CI=1.129–3.670), suicide plans (aOR=3.507, 95% CI=1.538–7.996), and suicidal behavior (aOR=7.130, 95% CI=2.035–24.978) after adjusting for the covariates. However, no increases in suicide risk were observed ≤1 year and ≥10 years after diabetes diagnosis.
Conclusion
In adults, diabetes is associated with an increase in suicide risk. Suicide risk in diabetes patients showed an inverted U-shaped depending upon the duration of diabetes.
INTRODUCTION
Suicide is a major public health problem worldwide, especially in South Korea, given that it has the fourth-highest suicide rate in the world [1-3]. Suicide has a complex relationship with several factors [4], and there have been several new attempts to prevent suicide [5]. It is known that identifying highrisk suicide groups and managing crises in advance can help prevent suicides [6]. Moreover, a previous study showed that people with chronic diseases often experience psychological difficulties such as depression and anxiety, which can influence someone to commit suicide [7].
Diabetes is a major chronic disease. According to a recent survey conducted in Korea, 13.8% of adults over the age of 30 in South Korea have diabetes [8]. Based on many studies on the relationship between diabetes and depression, 10% of diabetes patients experience major depression, and diabetes patients experience twice as much depression as the general population [9-14]. But, there are few studies examining the relationship between diabetes and suicide risk, and most of them were targeted at type 1 diabetes only [15].
Several studies have also been conducted on the relationship between the duration of diabetes and mental health. A study of elderly diabetes patients in 2019 showed that people with longer durations of diabetes experienced greater degrees of depression [16]. However, another study of diabetes patients observed a high degree of depression in the early stage after the diagnosis of diabetes, but the degree of depression de- creased 10 to 20 years after the diagnosis of diabetes [13,17]. As such, there are various opinions on the relationship between the duration of diabetes and psychological difficulties. Also, there have not been many studies on the duration of diabetes and the risk of suicide.
Therefore, in this study, the suicidal ideation, suicide plans, and suicidal behavior of diabetes patients were compared to those in the general population using the 8th Korea National Health and Nutrition Examination Survey (KNHANES VIII), a nationwide survey conducted in South Korea. In addition, we classified the patients as having ≤1 year, 2 to 9 years, and ≥10 years of diabetes duration, and evaluated the relationship between the duration of diabetes and the risk of suicide.
METHODS
Study participants
This study utilized data obtained from the first year of the KNHANES VIII (2019). The KNHANES is a nationwide survey conducted by the South Korean Ministry of Health and Welfare since 1998. A trained interviewer obtains information about the subject’s health and nutritional status crosssectionally through face-to-face interviews.
In the KNHANES VIII (2019), among 10,859 targeted subjects, 8,110 participated in the survey, showing a participation rate of 74.7%. Since our study was conducted only on adults, a total of 6,296 out of 8,110 participants, excluding 1,504 under the age of 19 and 310 who did not have data on diabetes diagnosis, were included. Among these subjects, 2,795 were male and 3,501 were female (Figure 1). The survey protocol was approved by the Korea Centers for Disease Control and Prevention Institutional Review Board (IRB Nos. 2018-01-03-C-A).
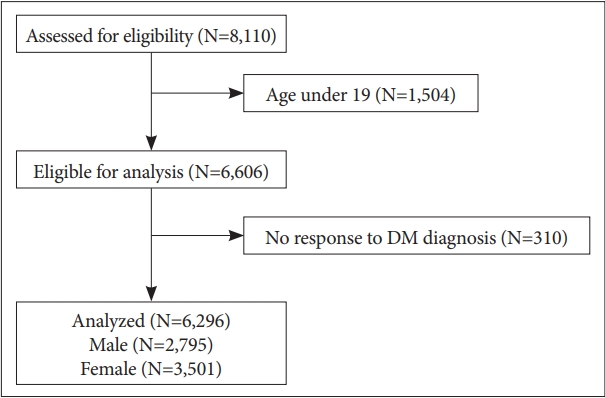
Flow diagram of subjects enrolled in the study. DM, diabetes mellitus.
Measurements and variables
The diagnosis of diabetes was determined by the answers to the self-reported question, “Have you ever been diagnosed with diabetes by a doctor?” The duration of diabetes was also confirmed by checking the age at which diabetes was first diagnosed through the question, “How old were you when you were first diagnosed with diabetes?” and calculating the difference from the age at the time of the investigation.
To assess suicide risk, the participants were asked the following questions: 1) suicidal ideation, “Have you ever seriously considered suicide in the past year?” (yes or no response); 2) suicide plan, “Have you made any specific plans to commit suicide in the past year?” (yes or no responses); and 3) suicidal behavior, “Have you actually attempted suicide in the past year?” (yes or no responses).
For covariates, sex, age, history of depressive disorder, marital status (married, single, divorced/separated/widowed), employment status (employed, unemployed), family income (low, low-moderate, moderate-high, high), the education level (≤elementary, middle school, high school, ≥college), smoking status (never, former, current), risky drinking (two or more times per week and three or more glasses per occasion), regular exercise (more than two hours and 30 minutes of moderate-intensity physical activity per week, or more than one hour and 15 minutes of high-intensity physical activity per week, or a mix of moderate-intensity and high-intensity physical activity), history of major cancer (stomach, liver, lung, colon, cervix, breast), and the number of chronic diseases (stroke, hypertension, ischemic heart disease, liver cirrhosis, chronic renal failure) were analyzed.
Statistical analysis
The KNHANES used two-stage stratified cluster sampling, not simple random sampling. Therefore, in this study, the data were analyzed by reflecting complex sampling, and an appropriate weight was assigned to each sample for analysis.
In this study, we cross-sectionally examined the differences in variables according to diabetes. The complex samples chisquared test was used to examine the differences between people diagnosed with diabetes and those who were not diagnosed with diabetes. Covariates were also adjusted using complex samples logistic regression analysis, and then the correlations between diabetes and suicide-related variables were examined. All data were analyzed using SPSS for Windows (Version 28.0; IBM Corp., Armonk, NY, USA).
RESULTS
Sociodemographic characteristics of the study population
The baseline sociodemographic characteristics of the study population are presented in Table 1. When comparing the di- abetes patients with the non-diabetes group, the diabetes patients were more likely to be male, older, alone (divorced/separated/ widowed), smokers, not doing regular exercise, unemployed, with lower income, and less education. These patients showed higher rates of depressive disorder, major cancer and chronic disease diagnosis. However, no statistical difference was observed in the rates of risky drinking between the diabetes group and the non-diabetes group.
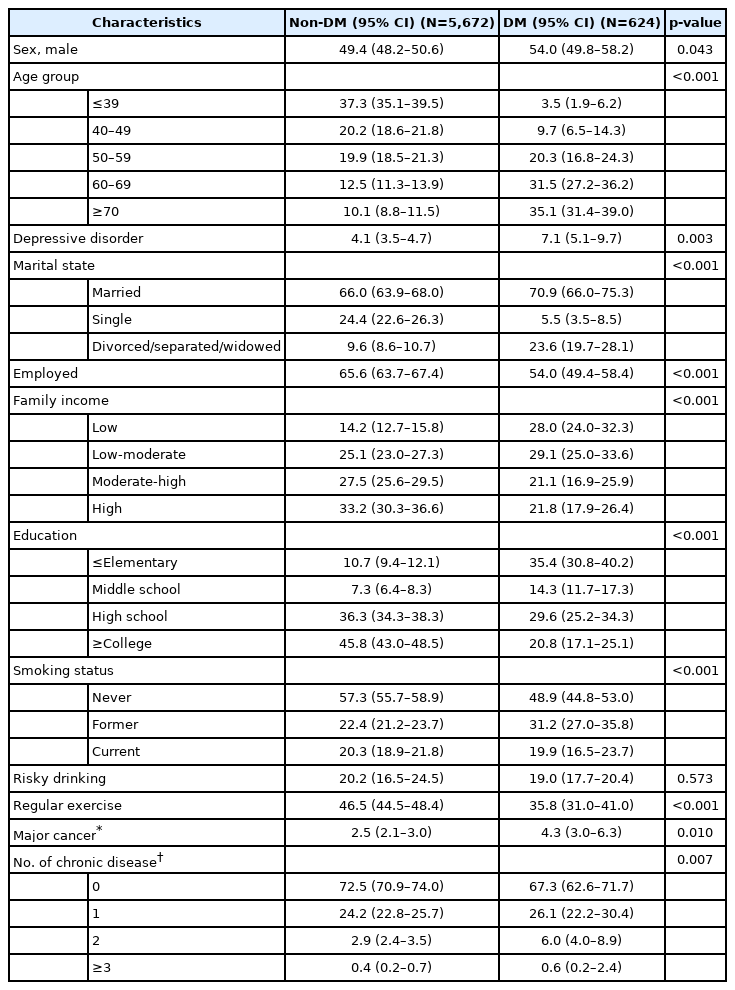
Sociodemographic characteristics of the study population (weighted)
Suicidality prevalence in diabetes patients
The prevalence of suicidality by diabetes status is presented in Table 2. Diabetes patients had significantly higher preva- lences of suicidal ideation (9.1%, p<0.001) and suicide plans (3.6%, p<0.001) than those without diabetes. However, in the case of suicidal behavior (1.0%, p=0.081), the prevalence was higher in diabetes patients, but this difference was not statistically significant.
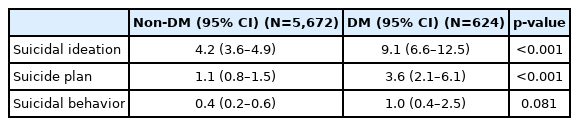
Suicidality of diabetes patients (weighted)
Association between diabetes and suicide risk
Table 3 shows the association between diabetes and suicide risk. In diabetes patients, the risk of suicidal ideation (odds ratio [OR]=2.285, 95% confidence interval [CI]=1.555–3.360) and suicide plans (OR=3.496, 95% CI=1.939–6.304) were significantly higher than those in the general population.
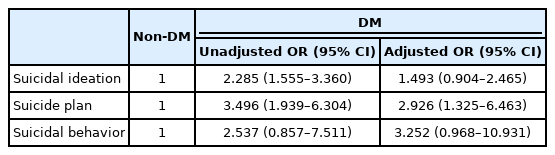
After adjusting for variables that differed between diabetes patients and the general population (sex, age, depressive disorder diagnosis, marital state, employment status, family income, education, smoking status, risky drinking, regular exercise, major cancer diagnosis, number of chronic diseases), suicide plans (adjusted odds ratio [aOR]=2.926, 95% CI= 1.325–6.463) were still significantly associated with diabetes. However, suicidal ideation (aOR=1.493, 95% CI=0.904–2.465) no longer showed a statistically significant association.
Association between diabetes and suicidality by diabetes duration
We divided the duration of diabetes into ≤1 year, 2 to 9 years, and ≥10 years and measured the association between the duration of diabetes and suicidality (Table 4). In the 2 to 9 years group, we found a significant increase in the risk of suicidal ideation (aOR=2.035, 95% CI=1.129–3.670), suicide plans (aOR= 3.507, 95% CI=1.538–7.996), and suicidal behavior (aOR= 7.130, 95% CI=2.035–24.978) after adjusting for covariates. However, in the ≤1 year group, no statistically increased risks in suicidal ideation (aOR=0.152, 95% CI=0.022–1.049), suicide plans (aOR=0.823, 95% CI=0.109–6.202) and suicidal behavior (aOR=2.999, 95% CI=0.275–32.693) were seen. Also, in the ≥10 years group, no significant differences were found in suicidal ideation (aOR=1.420, 95% CI=0.662–3.045) or suicide plans (aOR=2.941, 95% CI=0.812–10.654).

DISCUSSION
In this study, we examined the relationship between diabetes and suicide risk in adults through a nationwide survey conducted in South Korea in 2019. Of the diabetes patients, 9.1% experienced suicidal ideation in the past year, which was more than twice that of the control group without diabetes. And, the prevalence of having a suicide plan in the past year was 3.6%, which was more than three times that of the control group. In the case of suicidal behavior prevalence, statistical differences were not identified between the diabetes patient group and the control group; however, it was difficult to find statistical significance due to the small number of people that experienced suicidal behavior. Our finding of an increase in the prevalence of suicidal ideation and suicide plans in diabetes patients was consistent with those in previous studies. According to Tabb et al. [18], the prevalence of suicidal ideation in patients with type 2 diabetes ranged from 2.5% to 51.4%.
Significant increases in risk were observed in suicidal ideation (OR=2.285, 95% CI=1.555–3.360) and suicide plans (OR=3.496, 95% CI=1.939–6.304) before adjustment. And when covariates that differed between the diabetes patients and the general population were adjusted, a statistically significant increase in risk was confirmed only for suicide plans (aOR=2.926, 95% CI=1.325–6.463). After adjustment, suicidal ideation (aOR=1.493, 95% CI=0.904–2.465) no longer showed a statistically significant increase in risk. These results differed from previous studies in which the risk of suicidal ideation was increased in diabetes patients [19]. Several reasons can be considered for the lack of increase in the risk of suicidal ideation in diabetes patients after adjustment. First, the small number of people who experienced suicidal ideation may have widened the range of the CI. This is likely to be confirmed statistically as the KNHANES VIII data are accumulated in the future. Second, most of the previous studies focused only on suicidal ideation without distinguishing between suicidal ideation and suicide plans. This methodological difference may have been the cause of the results differences between this study and previous studies. Third, the risk of suicidal ideation decreased significantly after adjustment (OR=2.285 → aOR= 1.493). This suggests that the sociodemographic factors used for adjustment may be associated with the suicidal ideation of diabetes patients. Indeed, there was a significant sociodemographic difference between the diabetes group and the general population in our study. Diabetes patients were more likely to be alone (divorced/separated/widowed), unemployed, and have lower household incomes. Diabetes patients also had higher rates of depressive disorder, major cancer, and chronic disease diagnosis compared to the general population. All of these factors were conditions shown to increase suicide risk in previous studies [20-24]. And it may have increased the risk of suicidal ideation and suicide plans in diabetes patients before the adjustment in our study as well.
The adjusted risk of suicide plans in diabetes patients (aOR= 2.926, 95% CI=1.325–6.463) was three times higher than that of the general population in our study. This relationship between diabetes and suicide can be interpreted through several previous studies. Diabetes is a chronic disease that causes great psychological difficulties, and diabetes patients have a high rate of experiencing psychological difficulties such as depression and anxiety [25-27]. In particular, depression is one of the main causes of the increasing suicide risk [28], and diabetes patients may experience more depression which could increase suicide risk than that of the general population. Several studies have been conducted on the relationship between diabetes and depression. First, consider the common factors associated with the onset of diabetes and depression. Diabetes and depression are commonly associated with activation of the hypothalamic- pituitary-adrenal axis (HPA axis). Chronic stress observed in depressed patients activates the HPA axis, which stimulates the sympathetic nervous system and promotes the secretion of noradrenaline from the adrenal medulla [29]. This hormone secretion and stimulation of the sympathetic nervous system can cause insulin resistance, promoting type 2 diabetes [29]. Therefore, the possibility that diabetes and depression share a common cause can be considered. Second, insulin resistance observed in diabetes can lead to depression [30]. Several studies have suggested that insulin resistance can cause depression in diabetes patients by changes in brain glucose metabolism and neuroinflammation [31,32]. A cohort study conducted in 2021 observed an increased incidence of major depressive disorders in people with insulin resistance [33]. These factors may have induced depressive symptoms in diabetes patients, which may have increased the risk of suicide.
When examining suicide risk according to the duration of diabetes classified as ≤1 year, 2 to 9 years, and ≥10 years, only the 2 to 9 years group showed statistically significant increases in the ORs in all three categories of suicidal ideation, suicide plans, and suicidal behavior. However, an increase in suicide risk was not be observed in the ≤1 year and ≥10 year postdiabetes diagnosis groups. The suicide risk had an inverted U-shape depending upon the duration of diabetes. These results may be due to residual confounding factors, but could also reflect the true association between diabetes duration and suicide risk. Most likely, patients with diabetes mellitus for ≤1 year would have their blood sugar controlled with a small amount of oral antidiabetic medication and a lower incidence of major diabetic complications. In these conditions, although patients might experience adaptation problems, it would not increase the suicide risk. However, in the case of patients with diabetes mellitus for 2 to 9 years, as diabetes progresses, the dose and complexity of antidiabetic medications may gradually increase, including the use of insulin injections. Patients in this phase may also suffer psychological stress due to the failure of blood sugar control or lifestyle changes needed to manage diabetes. According to a previous study on the occurrence of complications in diabetes patients in South Korea in 2020, years 2 to 9 were the period when most diabetes complications occurred [34]. These factors could impose a great psychological burden on diabetes patients and contribute to the increase in suicide risk in the group with diabetes mellitus between 2 to 9 years. More than 10 years after a diabetes diagnosis, patients may gradually adapt to diabetes management, which explains why no increase in suicide risk was observed in the patients in this period.
Our study had several strengths. There have only been a few studies on the relationship between the duration of diabetes and suicide risk. In 2014, a study investigated the relation ship between suicidal ideation and diabetes regimens, diabetes duration, and HbA1c levels. The risk of suicidal ideation was found to increase as the duration of diabetes increased. However, in that study, the duration of diabetes was classified only as <5 years and ≥5 years [35]. By applying different classifications to subdivide the duration of diabetes, we were able to use additional factors to interpret how diabetes and suicide were related in a time-dependent way.
Furthermore, most other studies that dealt with the relationship between the duration of diabetes and psychological difficulties only looked at the relationship between the duration of diabetes and depression, not suicide. According to Almeida et al. [17], the relationship between diabetes duration and depression had a J-shape in 2016. In that study, when the duration of diabetes was less than 10 years, the degree of depression experienced by patients was relatively high, but like when the duration of diabetes was 10 to 20 years, the degree of depression was somewhat decreased [17]. In a study on the relationship between chronic diseases and depression in 2017, patients with diabetes, the only chronic disease studied, did not show an increase in depression immediately after their diagnosis, but the depressive symptoms gradually increased over time [36]. These results may also be related to our results, in that, a significant increase in suicide risk was not observed in the groups with a duration of diabetes of ≤1 year and ≥10 years, but the suicide risk increased in the group with a disease duration of 2 to 9 years.
This study had several limitations. First, as this study is a cross-sectional study, it is difficult to confirm the causal relationship between diabetes and suicide risk. Since previous studies reported a bidirectional relationship between diabetes and depression [10], additional research is needed to confirm the causal relationship between diabetes and suicide risk. Second, we could not measure the psychological burden of diabetes patients, such as depression and anxiety, which may have an association with suicide risk. Third, this study could not consider the severity of diabetes and the status of diabetes treatment. The more severe the diabetes is, the more diabetes complications will occur in patients, which could cause greater psychological stress in diabetes patients. Fourth, although this study adjusted for several confounding factors between diabetes patients and controls, there may still be confounding factors that have not been considered. In particular, the treatment status and the medication effects of comorbid diseases could be confounding factors that we did not consider, and these factors might have influenced our results. Fifth, the questionnaire used in this study asked the respondents to answer “yes” or “no” to suicidal ideation, suicide plans, and suicidal behavior. Therefore, the degree of suicide risk could not be measured.
Despite these limitations, we were able to obtain new results on the changes in suicide risk according to the duration of diabetes through a nationwide survey in this study. These results have not been reported previously and further studies are needed. In addition, medical staff should be aware of the suicide risk observed in diabetes patients when treating diabetes patients to offer appropriate interventions.
Notes
Availability of Data and Material
The datasets generated or analyzed during the study are available from the corresponding author on reasonable request.
Conflicts of Interest
Yoo Hyun Um, a contributing editor of the Psychiatry Investigation, was not involved in the editorial evaluation or decision to publish this article. All remaining authors have declared no conflicts of interest.
Author Contributions
Conceptualization: all authors. Data curation: Young-Chan Kim, Tae-Won Kim. Formal analysis: Young-Chan Kim, Yoo Hyun Um. Investigation: Young-Chan Kim, Sung-Min Kim. Methodology: Jong-Hyun Jeong. Supervision: Ho-Jun Seo, Seung-Chul Hong. Writing—original draft: Young-Chan Kim. Writing—review & editing: Jong-Hyun Jeong.
Funding Statement
None