Effect of Parental Perception on the Prevalence of Adolescent Internet Gaming Disorder During the COVID-19 Pandemic
Article information

Abstract
Objective
During the coronavirus disease (COVID-19) pandemic, several studies have found that Internet usage and gaming times have increased among adolescents. Parents’ Internet literacy and attitudes toward Internet gaming have been reported to affect children’s Internet gaming disorder (IGD). We hypothesized that parents’ attitudes toward Internet use and gaming would affect the prevalence of IGD among adolescents.
Methods
A total of 199 mothers of children who played Internet games were surveyed online to gather information regarding their demographic characteristics, children’s Internet use patterns, psychological factors, and Internet gaming literacy.
Results
Among adolescents, increased Internet usage or gaming time was not associated with IGD, but the presence of attention deficit hyperactivity disorder (ADHD) was. Among parents, anxiety, depression, and family togetherness were not related to IGD, but a positive perception of gaming protected against the development of IGD, whereas a negative perception was a risk factor for IGD.
Conclusion
Increased gaming time neither causes nor correlates with IGD in adolescents, even though ADHD may be a risk factor for IGD. Parents’ positive or negative perceptions of gaming can be protective or present a risk factor, respectively, for their children’s development of IGD.
INTRODUCTION
The increase in Internet usage and gaming time during the coronavirus disease pandemic
Physical distancing and social isolation have been implemented worldwide to avoid the spread of the coronavirus disease (COVID-19). Since then, screen times, including Internet usage for work and academic activities, social network service usage, and Internet gaming, have significantly increased [1,2]. There have been contradictory takes on the correlation between increased Internet gaming time and problematic gaming behaviors [3]. Several studies have suggested that gaming time is a crucial factor for the increased risk of Internet gaming disorder (IGD) [4,5], while other studies have reported a weak correlation between the two [6,7]. Considering these differences, there is scientific interest in establishing whether IGD is related to increased Internet gaming time.
Risks and protective factors of IGD
Studies have suggested several factors associated with IGD in addition to Internet gaming patterns, including game genres and time spent playing [3,6]. Comorbid psychiatric diseases, including depression [8] and attention deficit hyperactivity disorder (ADHD) [9], are significant predictive factors for IGD. Several studies have suggested that the stress induced by interpersonal relationships, school performance, and problems in parent–child relationships could increase the prevalence of IGD [10-15]. Furthermore, if games are used mainly to cope with stress, it becomes a predictor of IGD [10]. Depression and anxiety in parents can also be linked to children’s IGD [11,12]. While a healthy parent–child relationship could serve as a protective factor against IGD [13], parental surveillance and conflict are risk factors [14,15].
Effects of parents’ gaming awareness on children’s IGD
In an online survey of 1,000 Korean adults, it was found that they perceived Internet games as obstacles to study, “just games,” a “stain on life,” and vaguely sinister [16]. Problematic parent–child relationships have been found to be significant predictors of children’s IGD [11-15], and parents’ attitudes toward and awareness of Internet gaming have also been reported to affect IGD [17-19]. Awareness, experience, and positive perceptions of Internet gaming among adults may reduce children’s vulnerability to IGD [20]. Nielsen et al. [17] reported that the quality of parental mediation could either negatively or positively impact children’s Internet use. Koning et al. [18] suggested that ineffective parental responses to children’s Internet gaming aggravates problematic Internet gaming behaviors. González-Bueso et al. [19] found that parental psychoeducation led to higher participation in IGD treatment in children.
Hypothesis
We hypothesized that, during the COVID-19 pandemic, Internet use and gaming would increase among adolescents. We also hypothesized that the prevalence of IGD would be associated with parents’ perceptions and awareness of the Internet and Internet gaming.
METHODS
Participants and recruitment process
Invitation e-mails were sent to registered members by an online research company, Embrain (Seoul, Korea). Each participant received a compensation of $15. In the first week, 100,000 e-mails were sent and 518 participants began the survey by the end of the week. By the end of the second week, 237 participants had submitted their responses. Of these 237, 38 were excluded due to incomplete answers. The inclusion criteria were as follows: 1) women with children who played Internet games, 2) women aged 30–50 years, and 3) children aged 12–18 years. The exclusion criteria were as follows: 1) history of psychiatric disorders, including schizophrenia, bipolar disorder, substance use disorder, and intellectual disability and 2) having children already diagnosed with IGD.
The Institutional Review Board of Chung-Ang University Hospital approved this study (IRB No. 2090005434). Informed consent was obtained from all the participants before participation.
Assessment
Participants were asked to provide data regarding their demographic characteristics, psychological factors, their children’s Internet use patterns, and their awareness of Internet gaming.
Demographic characteristics and Internet use pattern questionnaires
Demographic data included age, years of education, children’s age, gender, and academic level. Participants further provided data about their own duration of Internet usage and gaming, that of their children, and the differences between gaming times prior to and during the COVID-19 pandemic. The reasons why children play games were also investigated and divided into four categories: achievement: playing for game mastery, competition, receiving recognition/rewards, or gaining power within the game; social relationship: playing to interact with others and developing in-game relationships; coping: playing to cope with stress or boredom, distract from real-life problems, or escape from unpleasant feelings; and entertainment: playing to have a good time, getting excited, or relaxing [10].
Psychological scales
The participants provided information regarding their depression and anxiety symptoms, their children’s ADHD symptoms, and family togetherness. Depression was measured using the Center for Epidemiologic Studies-Depression Scale (CES-D) [21,22]. Anxiety was measured using the Korean version of the Beck Anxiety Inventory (BAI) [23,24]. The severity of ADHD symptoms was assessed using the Korean version of the DuPaul ADHD Rating Scale (K-ARS), parents’ version [25,26]. Family togetherness was measured using an excerpt from the family section of the School Success Profile developed by Bowen and Richman [27].
Internet Game Literacy Scale and knowledge of gaming
The Internet Game Literacy Scale examines whether individuals have a positive or negative perception of Internet games [28]. It consists of nine positive scales (e.g., “gaming can reduce stress,” and “people can develop friendships and social skills through games”) and nine negative scales (e.g., “gaming can induce violence” and “games ruin living patterns in reality”), using a 5-point Likert scale rating (1=“strongly disagree,” 2=“disagree,” 3=“neutral,” 4=“agree,” and 5=“strongly agree”). Cronbach’s alpha for the scale was=0.892 [28]. The participants were asked to evaluate their perception of the game based on the time before the COVID-19 pandemic. Knowledge of gaming was assessed based on whether mothers knew which games their children played.
Diagnosis of IGD
Participants were asked to complete the gaming diagnostic interviews before and during the COVID-19 pandemic. The gaming diagnostic questionnaire was originally developed as a semi-structured gaming diagnostic interview to establish a diagnosis of IGD and gaming disorders (GD). It comprises nine items that correspond to the nine diagnostic criteria for GDs [29,30]. In our study, the scale was modified to nine simple questions regarding participants’ perceptions of their children’s Internet gaming habits. The internal consistency of our modified gaming diagnostic questionnaire in the current study had a Cronbach’s alpha of 0.811. The children of participants who indicated that they demonstrated the presence of more than five out of nine criteria were diagnosed with IGD.
Statistical analysis
Demographic characteristics, including participants’ age and education as well as their children’s age and education, were analyzed using an independent t-test. The role of children’s gender was analyzed using a chi-square test. Psychological scales, including the CES-D, BAI, K-ARS parent version, and the Family Togetherness Scale were compared using independent t-tests. The Internet use patterns of participants and their children were compared using independent t-tests.
To determine the influence of mothers’ gaming awareness on IGD, we performed hierarchical logistic regression analyses using “changed to IGD group” as the dependent variable. The changed group was defined as children who did not demonstrate symptoms of IGD before the pandemic but began showing them during the pandemic. A discrete set of hierarchical variables was added: Model 1, child factors; Model 2, child factors + mothers’ factors; and Model 3, child factors + mothers’ factors + mothers’ knowledge of Internet gaming. The dependent variable—changed to IGD group—was coded as 1 and the non-changed group was coded as 0.
Hierarchical regression analysis shows whether the variables of interest can account for significant variance in a dependent variable after considering all other variables. Each step of the logistic regression model was verified with χ2-values (model χ2 and step χ2) and goodness-of-fit indices (–2 log likelihood). Model χ2 and step χ2 can determine improvements observed in the model with predictors relative to the constant-only model or the prior model. To evaluate the actual usefulness of each model, classification accuracy tables were used to determine the relative influence of each model in predicting correlations with the changed group. In addition to the indices of the overall model fit, Nagelkerke’s R2 was evaluated as an approximate estimate of the variance in the dependent variable accounted for by the model. Wald statistics were used to test whether each individual factor had a significant relationship with the change to IGD. When a significant relationship was detected by the Wald test, interpretation of the coefficient was followed by determination of the odds ratio; that is, the ratio between the probability that the event (i.e., changed to IGD) would occur or not.
RESULTS
Demographic data and clinical scale scores
There were no significant differences in mothers’ ages, education, children’s ages, gender, education, children’s reasons for gaming, and Family Togetherness Scale between the unchanged and changed groups (Table 1). Compared to the unchanged group, the participants in the changed group showed higher K-ARS scores (t=-7.1, p<0.01), mothers’ CES-D score (t=-3.4, p<0.01), and mothers’ BAI scores (t=-3.7, p<0.01).

The comparison of variables influencing IGD in children in the changed to IGD and non-changed groups
There were no significant differences between the two groups in terms of Internet use and gaming before the pandemic; however, after the pandemic, the changed group reported longer Internet use time (t=-2.9, p<0.01) and gaming time (t=-2.6, p=0.01). For mothers’ Internet use time and Internet gaming time, there were no significant differences between the two groups, either before or after the pandemic. The mothers of children in the changed group reported decreased positive attitudes toward gaming (t=5.0, p<0.01), and increased negative perceptions (t=-5.9, p<0.01).
Hierarchical logistic regression analysis
Considering the value (d=2.14) of the Durbin–Watson test, there was no autocorrelation in the dataset. All three models employed in the current study were associated with the changed group.
In Model 1, model χ2 (45.8, p<0.01) and Nagelkerke’s R2 (0.375, 37.5% of variance in the dependent variable of the changed group) indicated that the model was adequate for predicting IGD. When the practical usefulness of the model was examined based on classification accuracy, seven variables in Model 1 enhanced the prediction accuracy of the group membership of the dependent variable to 90.5%. Regarding step χ2 (45.8, p<0.01), child factors were the predictive factors for IGD. In Model 2, model χ2 (51.3, p<0.01) and Nagelkerke’s R2 (0.415, 41.5% of variance in the dependent variable of the changed group) indicated that the model was adequate for predicting IGD. However, regarding step χ2 (5.5, p=0.48), mothers’ factors could not predict IGD in their children. In Model 3, model χ2 (79.1, p<0.01) and Nagelkerke’s R2 (0.599, 59.9% of variance in the dependent variable of the changed group) indicated that the model was adequate for predicting IGD. When the practical usefulness of the model was examined based on classification accuracy, 17 variables in Model 3 enhanced the prediction accuracy of the group membership of the dependent variable to 94.5%. Regarding step χ2 (27.8, p<0.01), mothers’ game perceptions were predictive of IGD in children.
According to the Wald statistics for all independent variables, potential predictors of IGD included higher K-ARS scores, lower scores on the positive Internet Game Literacy Scale, and higher scores on the negative Internet Game Literacy Scale (Table 2).
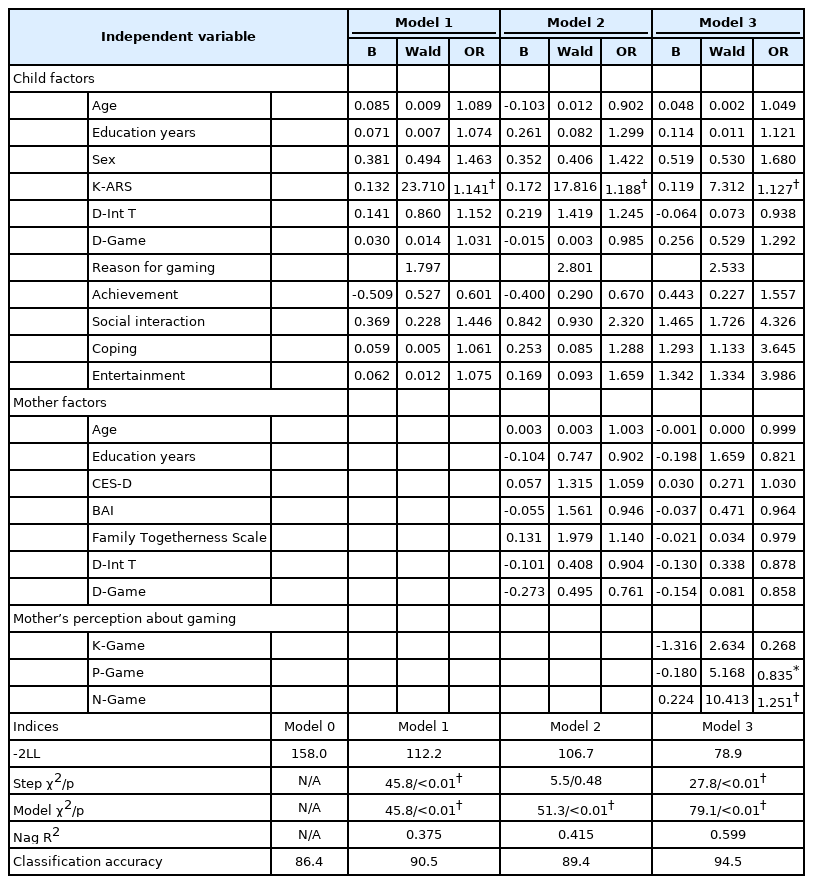
Results of the hierarchical logistic regression analysis
DISCUSSION
In this study, adolescents’ increased Internet usage and gaming were not found to be correlated with IGD; however, their experience of ADHD symptoms was found to be an associated factor. Parents’ anxiety, depression, and family togetherness were not related to IGD. However, mothers’ positive perceptions of gaming acted as a protective factor against IGD, and negative perceptions acted as a risk factor.
Children’s factors: ADHD
Diagnoses of ADHD were significantly related to the development of IGD during the COVID-19 pandemic. This finding is consistent with previous studies stating that IGD is associated with attention problems and impulsivity [9,31,32]. Early screening for ADHD and therapeutic intervention in children are expected to lower the risk of IGD. In our study, the increase in Internet usage and gaming time were separately associated with IGD, but this association disappeared when they were analyzed together in a multivariate analysis. In previous studies, the relationship between the time spent playing games and problematic gaming behaviors has been contradictory. Several previous studies have shown a weak-to-moderate correlation between gaming time and IGD [4,6,7]. Similarly, King et al. [33] and Király et al. [34] have expressed concerns about children’s increasing Internet usage and gaming during the COVID-19 pandemic, when problematic gaming behaviors increased. However, other studies found that increased gaming time was not associated with problematic gaming behaviors [35,36]. Some researchers have pointed out the possibility of gaming time as a confounding variable for problematic gaming behaviors, citing programmers as examples of individuals who spend significant time using the Internet or gaming without negative consequences [35,37].
Mothers’ factors: positive and negative gaming perceptions
To the best of our knowledge, this is the first study to investigate the impact of parental views on children’s IGD. Mothers’ positive perceptions of gaming acted as a protective factor against the development of IGD in children, whereas negative perceptions were risk factors for its development.
In previous studies, healthy parent–child relationships have been cited as a preventive factor against IGD; however, contentious relationships led to an increase in children’s problematic gaming behaviors [13-15,31,38]. However, in this study, family togetherness was not associated with IGD. This finding may be because our data did not include sufficient participants to confirm the effects of family cohesion. Additionally, previous studies did not examine parental perceptions of gaming, which was a significant factor in our study; hence, this factor and family cohesion may influence each other, contributing to the significant effect of the former and non-significant effect of the latter found in our study. Moreover, it is possible that family togetherness did not play a significant role due to socio-environmental changes such as increased time spent with family members during the COVID-19 pandemic.
Children’s problematic gaming behaviors may increase when parents have negative perceptions of gaming [18,38-40]. Several studies have shown that children’s and parents’ perceptions of gaming differ, which can trigger further conflicts between them. In a study conducted by Kutner et al. [39], parents reported concern about the effects of games on their children, but lacked knowledge of the types of games their children played and the actual and experienced effects of them. Koning et al. [18] found that increasing communication between parents and boys regarding Internet use could worsen the symptoms of IGD, as their different perceptions intensified conflict over gaming. In a study conducted by Eklund and Helmersson Bergmark [40], parents who believed games to be addictive were more restrictive in dealing with their children. Da Charlie et al. [38] suggested that children’s pathological gaming could increase to cope with increasing family conflict.
Our results show that improving parental perceptions of Internet use and gaming could reduce children’s problematic gaming behaviors. Bonnaire et al. [41] emphasized that it is important for parents to correct negative perceptions of games and recognize their positive aspects in the course of adolescents’ IGD treatments. Limited experience of using the Internet or online gaming could contribute to parents’ negative perceptions; for instance, Vroman et al. [42] found that elderly people with no experience of online activities expressed being “frightened” and “anxious” about technology. A study conducted by Castilla et al. [43] showed that users with no information and communication technology experience, who received eight sessions of computer training, demonstrated increased confidence, interest, and positive perceptions of technology. Considering these findings, it can be expected that properly educating parents about the Internet and online gaming may reduce their negative perceptions and help them recognize the positive aspects of the online world. Future studies are required to examine the impact of parental technological education on perceptions of the Internet and gaming, and subsequently on children’s problematic gaming behaviors and IGD.
Limitations
Our study had several limitations. First, it is based on data collected from mothers; thus, it may differ from experiences reported by children themselves. However, in previous studies, parents’ judgment of IGD symptoms had shown significant reliability and consistency with judgments from adolescent gamers [44], and we expect that there will be no significant differences between the data we obtained from mothers and self-reports from their children. Second, depression and anxiety in children are also considered risk factors for IGD [45]. However, the current study did not investigate these factors. Future research should consider these factors. Third, there may be a recall bias, as we retrospectively collected data regarding the pre-COVID-19 period. Prospective studies on the effects of parents’ perceptions of gaming on children’s IGD are required. Fourth, it may be difficult to generalize our results to a relatively small number of patients with IGD.
In conclusion, increased time spent gaming does not cause IGD among adolescents, but the presence of ADHD may be a risk factor for their development of IGD. Parents’ positive or negative perceptions of gaming can be either a protective or risk factor for the development of IGD in children. Providing parents with Internet and gaming education can reduce negative perceptions of gaming, which can reduce children’s experiences and symptoms of IGD.
Notes
Availability of Data and Material
The datasets generated or analyzed during the study are available from the corresponding author on reasonable request.
Conflicts of Interest
The authors have no potential conflicts of interest to disclose.
Author Contributions
Conceptualization: Doug Hyun Han, Seo-Koo Yoo. Data curation: Soyeon Lee, Sun Mi Kim. Formal analysis: Doug Hyun Han, Seo-Koo Yoo. Funding acquisition: Doug Hyun Han. Investigation: Doug Hyun Han. Methodology: Doug Hyun Han, Seo-Koo Yoo. Project administration: Soyeon Lee. Validation: Soyeon Lee. Writing—original draft: Doug Hyun Han, Young Don Son. Writing—review & editing: Sun Mi Kim, Young Don Son.
Funding Statement
The current study was supported by funding from the Korean Association of Game Industry 2020. This work was supported by a National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIT) (NRF-2020R1A4A1019623).