Association of Sociodemographic and Psychosocial Factors With COVID-19–Related Post-Traumatic Stress Disorder Risk Group Among Medical Students
Article information

Abstract
Objective
Several previous studies have reported the negative psychological impact of the coronavirus disease (COVID-19) pandemic on medical students worldwide. This study investigated the sociodemographic and psychosocial factors associated with COVID-19–related post-traumatic stress disorder (PTSD) risk among medical students in Daegu, a region that experienced a high concentration of infections.
Methods
A total of 270 students completed the self-reported questionnaires including COVID-19 exposure, psychological measurement, and sociodemographic factors. We evaluated the COVID-19–related PTSD risk group using the Korean version of the Impact of Event Scale-Revised. Logistic regression analysis was performed to evaluate the odds ratio for the COVID-19–related PTSD risk group in sociodemographic and psychosocial factors.
Results
The prevalence of the COVID-19–related PTSD risk group was 10.4% in medical students. Among sociodemographic factors, lower grades (specially, first-year medical students) and current smokers were associated with the COVID-19–related PTSD risk. Indirect exposure to COVID-19 was also associated with this risk. Meanwhile, having higher resilience, self-esteem, and social support were less likely to be associated with COVID-19–related PTSD risk.
Conclusion
This study suggested that it is necessary to develop a system for the screening and managing of COVID-19–related PTSD risk group among medical students, especially high-risk groups during the COVID-19 pandemic.
INTRODUCTION
In December 2019, the coronavirus was reported to cause fatal contagious pneumonia and has quickly spread from China to many other countries, including South Korea. The World Health Organization (WHO) declared the coronavirus disease (COVID-19) outbreak a global pandemic on March 11, 2020 [1]. In February 2020, the Daegu area of South Korea became a large-scale regional infection area as the number of confirmed cases increased rapidly in religious communities and long-term care facilities. Therefore, the Daegu area was declared a special disaster area [2].
Medical students have been suffering from academic stress due to the excessive burden of learning caused by repetitive tests, extreme competition, and grade retention. [3]. Previous studies conducted prior to the COVID-19 pandemic have found that medical students exhibit a significantly higher prevalence of mental health problems—such as depression and anxiety— than the general population [4-6]. Furthermore, amidst the fear and considerable uncertainty surrounding COVID-19, medical students, who requisitely need clinical experience, had to adapt to new educational environments such as remote elearning due to the postponement of the face-to-face clinical clerkship and may have suffered severe stress due to rapid changes in systems and environments [7].
Moreover, when such an epidemic occurs, the medical community’s primary concern is managing infectious diseases and improving the disease management systems [8]. During the outbreak, health care workers were also at risk as they accounted for 15%–18%—and in some cases, 20%—of the total infected population [9]. This lethal situation was the same for students attending classes in hospitals. Such outbreaks cause psychological stress among medical students. Most medical students experience anxiety, depression, and stress [10,11].
Given the severe psychological distress associated with the pandemic, mental health problems among current medical students could be serious. As these students are important resources for future medical care, their mental health problems could cause a decline in its quality [12]. Thus, there is a need for early screening, prevention, and treatment of medical students at risk of developing mental health problems associated with COVID-19.
Post-traumatic stress disorder (PTSD) is triggered by exposure to actual or threatened serious injury, death, or sexual violence, and is considered a secondary effect of the pandemic [13]. Previous studies on COVID-19 have shown that PTSD could occur during and after infectious diseases [14]. However, several risk and protective factors have been identified, but these findings have not been consistent [15]. Moreover, few studies examine the association of these factors with COVID-19–related PTSD risk among medical students. Therefore, this study investigated the prevalence of PTSD risk group associated with COVID-19 and the sociodemographic and psychosocial factors associated with it among medical students in Daegu, a region that experienced a high concentration of infections.
METHODS
Study design and participants
The Kyungpook National University School of Medicine has conducted mental health assessments for students annually since 2009. These assessments were conducted through self-reported questionnaires targeting students of three grades (premedical first-year, medical first-year, and medical thirdyear). The cross-sectional study was based on data from the medical students’ mental health assessment of Kyungpook National University School conducted in 2021. This crosssectional study sample consisted of 270 students who completed all questionnaires, including questions related to COVID-19 exposure, among those who participated in the 2021 survey (participation rate, 80.4%).
COVID-19 exposure
To evaluate the extent of respondents’ exposure to COVID-19 in 2021, we asked the following questions: 1) Have you ever been tested for COVID-19? 2) Have you ever been selfquarantined due to COVID-19? 3) Have you ever been diagnosed with COVID-19? 4) Has anyone in your family or close acquaintances been self-quarantined due to COVID-19? and 5) Has anyone in your family or close acquaintances been diagnosed with COVID-19?
All COVID-19 exposure variables were assessed as binomial (yes or no). We defined at least one affirmative answer to the questions about self (Questions 1, 2, and 3) as having experienced direct exposure and at least one affirmative answer to the questions about family or close acquaintances (Questions 4 and 5) as having experienced indirect exposure. We considered respondents who responded “yes” to at least one of the five questions as the exposure group.
Psychological measurements
Impact of Event Scale-Revised
To assess the PTSD symptoms among participants, this study employed the Korean version of the Impact of Event Scale-Revised (IES-R-K) as translated from the IES-R by Eun et al. [16]. Although the IES-R was not intended as a diagnostic instrument, it is one of the most extensively used screening measures to assess the presence and severity of PTSD symptoms in clinical and non-clinical settings [17,18]. The IES-R has demonstrated high levels of internal consistency (the range of Cronbach’s alpha [α] for the subscales: 0.79–0.94) and testretest reliability (0.89–0.94) [19,20]. The IES-R has demonstrated high levels of internal consistency (the range of Cronbach’s α for the subscales: 0.79–0.94) and test-retest reliability (0.89– 0.94) [16].
The scale consists of 22 questions on hyperarousal, avoidance, intrusion, sleep and numbness with respect to particular stress events. Respondents rate how distressing each item has been for them in the last seven days using a five-point Likert scale from 0 (not at all) to 4 (extremely). Total scores of ≥25 in the Korean version of the IES-R are indicative of a diagnosis of PTSD, whereas scores of ≥18 are indicative of the presence of PTSD-like symptoms [16,21,22]. In this study, participants with IES-R-K scores of ≥25 were classified as COVID-19–related PTSD risk group.
Beck Depression Inventory-II
The Beck Depression Inventory-II (BDI-II) uses 21 items to evaluate the cognitive, behavioral, affective, and somatic components of depression and measures the type and degree of depression based on clinical depressive symptoms. This scale requires participants to select a statement that best describes their state over the past week. The items were rated on a fourpoint Likert-type scale ranging from 0 to 3. The higher the score, the more severe the depression. In the present study, the validated Korean version of the BDI-II was used to assess the occurrence and severity of depressive symptoms (Cronbach’s α=0.91) [23].
Beck Anxiety Inventory
The Beck Anxiety Inventory (BAI) was developed as a tool to measure anxiety-related symptoms such as thoughts, physical states, and panic states over the past week and was constructed to avoid confounding with depression. In total, 21 items were rated on a four-point Likert-type scale ranging from 0 (not at all) to 3 (very severe). The higher the total score, the more severe the anxiety-related symptoms. We used the standardized Korean version of the BAI-II (Cronbach’s α=0.91) [23].
Korean Smartphone Addiction Proneness Scale for Adults
The Korean Smartphone Addiction Proneness Scale for Adults, developed by the Korea National Information Society Agency, is a 15-item questionnaire used to measure smartphone addiction (Cronbach’s α=0.81) using four sub-factors: daily life impairment, virtual world orientation, withdrawal, and tolerance [24]. Items were rated on a scale from 1 (not at all) to 4 (extremely). The samples were classified into three groups according to the scoring criteria of the Korea National Information Society Agency. A high-risk user group obtains a total score of 44 or higher or that meets all 15 or more points of daily living disability, 13 or more points of withdrawal, and 13 or more points of tolerance. The potential-risk user group obtains a total score of 40–43 points or 14 or more points of daily living disability. Finally, a general user group belongs to neither of the abovementioned groups. In this study, we defined both the high-risk user group and the potential-risk user group as the risk group.
Alcohol Use Disorders Identification Test
The Alcohol Use Disorders Identification Test (AUDIT), developed by the WHO to screen at-risk drinkers, was used to measure alcohol addiction among medical students. The scale consists of 10 questions on drinking behaviors, dependence symptoms, and alcohol-related problems, and is evaluated on a 0-to-4-point scale. The Korean version of the AUDIT was based on the amount of Korean liquor and has been verified in the Korean population (Cronbach’s α=0.92) [25]. According to the Korean version of the standard, those who scored more than 20 points for men and 10 points for women were classified as high-risk drinking group (supposed alcohol use disorder group), and those who scored between 10 and 19 points for men and between 6 and 9 points for women were classified as risk drinking group [26]. And the general user group was the group that did not belong to either of the above two groups. We defined both high-risk drinking and risk drinking groups as the risk group in this study.
Perceived Stress Scale
The Perceived Stress Scale (PSS) is an instrument used to assess the level of stress experienced over the past month [27]. The current study used the Korean version of the PSS (Cronbach’s α=0.82) [28]. Ten items were rated on a scale from 0 (never) to 4 (very often). Questions 4, 5, 7, and 8 were back-scored as negative questions with a total range of 0–40 points. The higher the total score, the greater the perceived level of stress.
Connor-Davidson Resilience Scale
The Connor-Davidson Resilience Scale (CD-RISC) is an instrument that evaluates resilience related to coping skills in stressful events [29]. The Korean version of the CD-RISC with excellent internal consistency was developed in 2010 (Cronbach’s α>0.9) [30]. It consists of a total of 25 questions, and each item is rated on a scale from 0 (not at all) to 4 (extremely). The higher the total score, the greater the psychological resilience.
Rosenberg Self-esteem Scale
The Rosenberg Self-esteem Scale is an instrument that evaluates an individual’s self-esteem, that is, the level to which one respects oneself and the level to which one considers himself worthwhile [31]. A total of 10 questions are rated on a scale from 0 (not at all) to 3 (extremely), and questions 3, 5, 8, 9, and 10 are scored inversely. Higher scores indicate higher selfesteem. In the present study, the scale tool developed by Rosenberg [31] and cited by Yoo et al. [32] was used (Cronbach’s α=0.86).
Multidimensional Scale of Perceived Social Support
The Multidimensional Scale of Perceived Social Support (MSPSS) is an instrument that evaluates the degree to which people perceive that they are receiving appropriate social support. It consists of three domains of four questions each: family, friends, and meaningful others. The items are rated on a four-point Likert-type scale ranging from 1 (not at all) to 7 (extremely). The higher the score, the higher the perceived social support. We used the Korean version of the MSPSS (Cronbach’s α=0.90) [33,34].
Suicidality
We assessed suicidality using three questions. “Have you ever thought about committing suicide due to stress or psychological distress?” was used to assess lifetime suicidal ideas; “Are you currently thinking about committing suicide due to stress or psychological distress?” was used to assess current suicidal ideas; and “Have you ever attempted suicide due to stress or psychological distress?” was used to assess the lifetime suicide attempts.
Sociodemographic factors
We also gathered data on sociodemographic factors using a self-reported questionnaire: age, gender (men/women), grade (premedical first-year, medical first-year, medical third-year), living arrangement (living alone/not living alone), smoking (current smoker/non-smoker [including ex-smoker]), and alcohol drinking (at-risk drinking/normal). Additionally, regarding drinking behavior, the “at-risk drinking” group was classified according to the National Institute on Alcohol Abuse and Alcoholism guidelines (men, consuming four or more drinks on any day or 14 or more drinks per week; women, consuming three or more drinks on any day or seven or more drinks per week) [35].
Statistical analysis
The sociodemographic variables of the COVID-19–related PTSD risk group and the control group were also compared and analyzed using the independent t-test for continuous variables and the chi-square test for categorical variables. Between the COVID-19–related PTSD risk group and the control group, we analyzed the psychological variables using the chi-square test and analysis of covariance test after controlling for sociodemographic variables.
Additionally, we performed the logistic regression analysis to investigate the association of the COVID-19–related PTSD risk group with sociodemographic and psychosocial factors. The collinearity between independent variables was evaluated by calculating the variance inflation factor. The goodness-offit was evaluated using the Hosmer–Lemeshow test. All statistical analyses were also performed using the Statistical Package for Social Sciences (version 26.0; IBM Co., Armonk, NY, USA). For these analyses, a two-sided test at the level of 0.05, was used to evaluate statistical significance.
Ethics statement
All participants were fully informed about the aims and methods of the study and provided written informed consent before participation. The present study was approved by the Institutional Review Board of the Kyungpook National University School of Medicine (IRB No. 2021-0086).
RESULTS
In 2021, 10.4% of students were classified into the COVID-19–related PTSD risk group. The sociodemographic characteristics of the COVID-19–related PTSD risk group and the control group are presented in Table 1. There were differences between the two groups in terms of age, grade, smoking behavior, and COVID-19 indirect exposure. The mean age of the COVID-19–related PTSD risk group was 20.6 years, which was lower than the control group, 21.8 years. In the COVID-19–related PTSD risk group, the proportions of low-grade (premedical first-year, 35.7%; medical first-year, 57.1%), current smoker (25.0%), and indirect COVID-19 exposure (64.3%) were higher than in the control group (premedical first-year, 28.9%; medical first-year, 34.3%; current smoker, 10.3%; indirect COVID-19 exposure, 36.4%). However, the proportion of direct and total exposure to COVID-19 did not differ between the two groups.
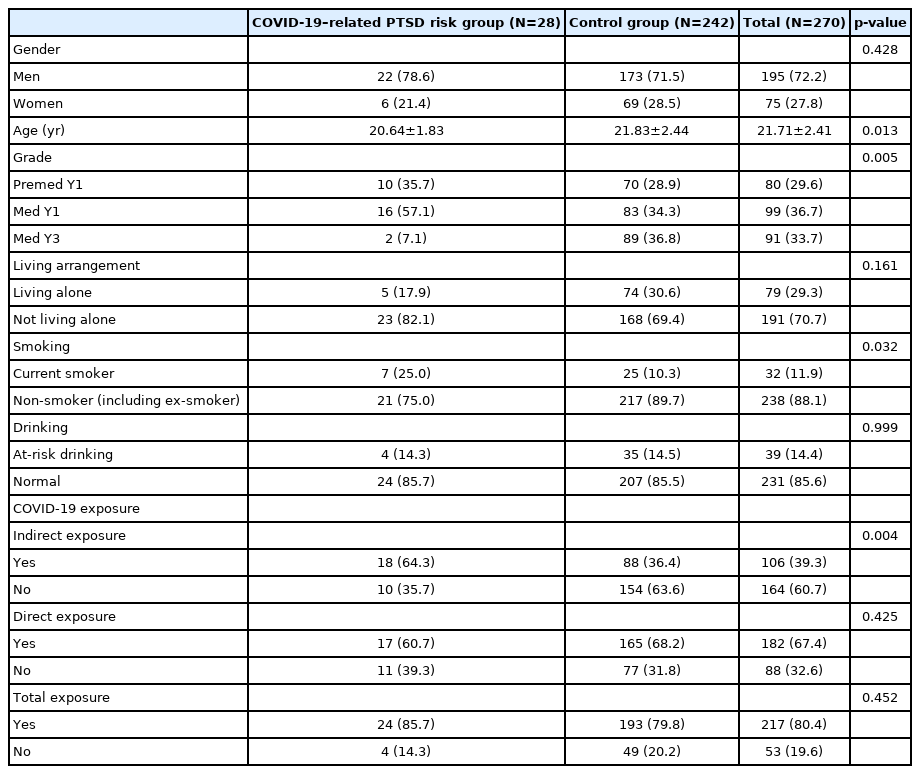
Sociodemographic characteristics of COVID-19–related PTSD risk group and control group (N=270)
Regarding psychological variables, there were differences between the COVID-19–related PTSD risk group and the control group. The mean scores for various psychological variables (depression, anxiety, stress, and smartphone use) were higher in the COVID-19–related PTSD risk group. Meanwhile, the mean scores for resilience, self-esteem, and social support were lower in the COVID-19–related PTSD risk group (Table 2).
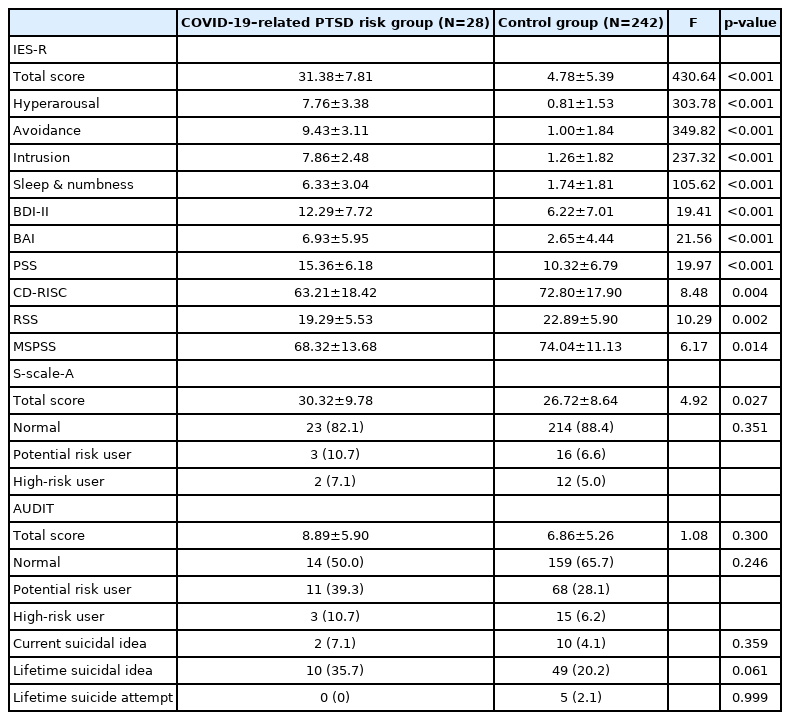
Psychological characteristics of COVID-19–related PTSD risk group and control group (N=270)
The odds ratios (ORs) of sociodemographic factors, COVID-19 exposure, psychosocial factors, and psychological variables for COVID-19–related PTSD risk are shown in Table 3. Being in lower grades (premedical first-year and medical firstyear), being a current smoker, and having experienced indirect COVID-19 exposure were associated with the COVID-19–related PTSD risk group. Moreover, having more depressive symptoms and anxiety symptoms, and having perceived higher stress was associated with the COVID-19–related PTSD risk group. On the other hand, having higher selfesteem, resilience, and social support and being older were less associated with the COVID-19–related PTSD risk group. When adjusted for COVID-19 exposure, and sociodemographic, psychosocial, and psychological variables, being a current smoker and higher stress were still associated with the COVID-19–related PTSD risk group. Additionally, older age was still less associated with the COVID-19–related PTSD risk group. Meanwhile, the statistical significance disappeared in the case of the lower-grade students and the indirect COVID19 exposure.
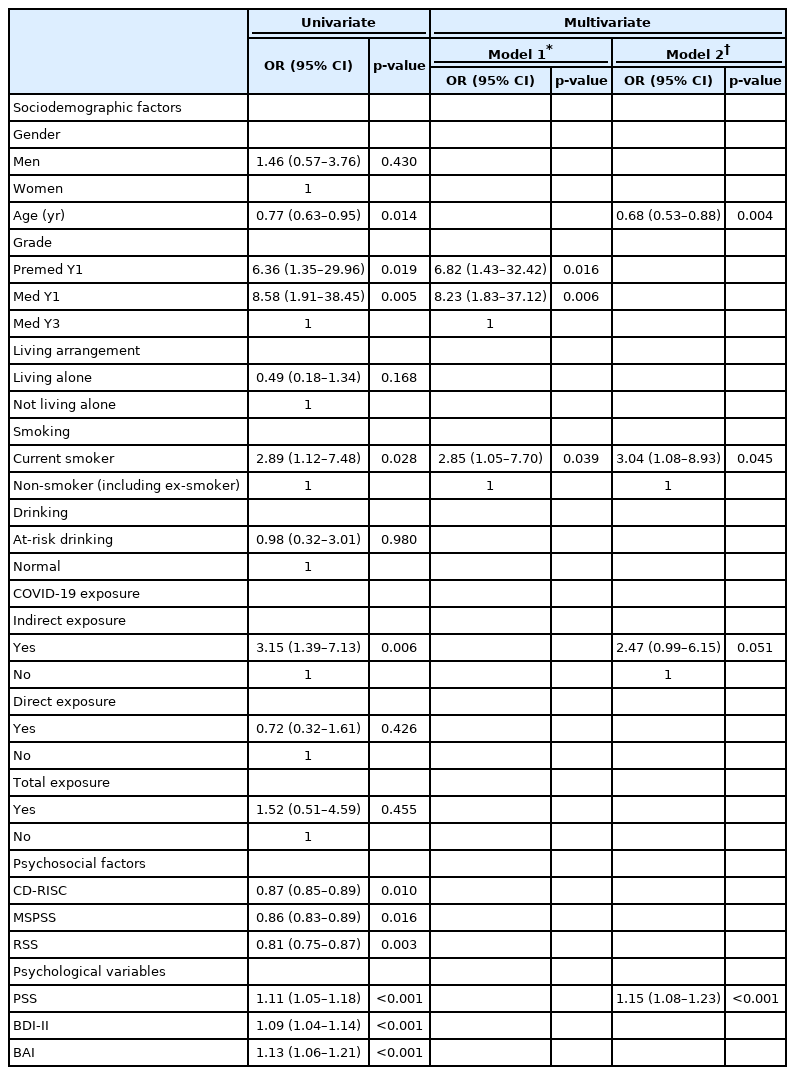
Results of univariate and multivariate logistic regression of sociodemographic factors and psychosocial factors associated with COVID-19–related post-traumatic stress disorder risk group
DISCUSSION
We investigated the sociodemographic and psychosocial factors related to PTSD risk group associated with COVID-19 among medical students. Being in a lower grade (especially, medical first-year), having experienced indirect exposure to COVID-19, and being a current smoker were associated with the COVID-19–related PTSD risk. Meanwhile, having higher self-esteem, resilience, and social support and being older were less associated with the COVID-19–related PTSD risk group.
For the respondents in 2021, we classified them into the COVID-19–related PTSD risk group and the control group according to the IES-R-K scale. In 2021, 10.4% of students were in the COVID-19–related PTSD risk group. This result was slightly lower than those of previous studies. In the US study using the Primary Care PTSD Screen for DSM-5 scale, 25.4% of medical students were screened positive for PTSD risk [36]. Another study using the IES-R scale reported that 22.7% of Indian medical students experienced a moderate psychological impact of COVID-19 [37]. Moreover, a Malaysian study found that 17.5% of students experienced COVID-19’s psychological impact [38]. Regarding the difference in prevalence, considering the differences in sample size and distribution (i.e. grade, gender), measurement scale, and sociocultural backgrounds is necessary. This difference may also be due to pandemic severity by country. In the data analysis from 35 countries, a significant and positive correlation was found between the prevalence of PTSD symptoms and the logarithm of the COVID-19 case fatality rate [39]. At the time of the survey, Korea belonged to a group of countries with relatively low COVID-19 mortality [40,41]; hence, the prevalence of COVID-19–related PTSD risk could be considered slightly lower than that of other countries.
In addition, the result of this study was slightly lower than those of a previous meta-analysis that reported a 15% PTSD risk prevalence in the general population during the COVID-19 pandemic in 2020 [42]. The reason for this difference can be considered based on the results of previous studies on infectious diseases (e.g., Ebola, severe acute respiratory syndrome, COVID-19) [43-45]. Medical students receive specialized education and possess greater medical knowledge than other students, and knowledge of diseases’ causes, prevention, and treatment helps reduce the anxiety related to—and psychological impact of—an outbreak. However, the prevalence is not low; hence, we should focus on the COVID-19–related PTSD risk among medical students, who are an important resource for future medical care.
The OR for COVID-19–related PTSD risk was highest in the medical first-year students, followed by the premedical first-year students. Among the three grades, medical thirdyear students were less likely to be associated with the COVID-19–related PTSD risk group. This could be partially due to a more realistic assessment of COVID-19 risk caused by maturity, time spent in the hospital, and interaction with clinical lecturers and medical staff [45]. Meanwhile, first-year medical students have experienced the most learning changes in the situation with the largest amount of learning because, unlike other grades, all classes have been moved online due to COVID-19. Therefore, first-year medical students do not experience campus life at all, and lack personal contact with peers and professors. Good social relationships allow students to perceive adequate support from friends and society, which is conducive to mental health [46]. Because of the current pandemic, first-year medical students have very limited social interaction, which makes it difficult to manage their mental health properly. For the premedical first-year students, it is important to consider that the first year of the university is a special transition period for students to establish their identity and social networks [47]. As the premedical first-year students mostly take online classes, they also lack social contact. This makes it difficult to form new relationships with peers and adapt to the changing university environment, which has a detrimental effect on mental health. For these reasons, premedical and medical first-year students are more likely to be influenced by COVID-19 [48]. Meanwhile, when adjusted for even psychological variables along with sociodemographic and psychosocial factors, the association of lower-grade students (premedical and medical first-year) and COVID-19–related PTSD risk group disappeared. This means that PTSD risk among lower grade students is closely related to psychological variables. Accordingly, it could be seen that, especially in the case of medical first-year students, it is necessary to pay more attention to PTSD risk and also depression and anxiety symptoms and stress.
Current smoking was associated with the COVID-19–related PTSD risk group. This finding is similar to previous studies showing that PTSD symptoms were more likely to be reported in smokers during the pandemic [49]. Continued smoking sensitizes the neurobiological stress response systems, resulting in an increased vulnerability to developing PTSD after exposure to a life-threatening situation [50]. In addition, smoking could be used to alleviate PTSD symptoms, that is, to decrease physiological arousal, or conversely to stimulate someone experiencing uncomfortable feelings of numbness or detachment [51].
Having a family member or close acquaintances diagnosed with COVID-19 or self-quarantined (i.e., indirect exposure) was associated with the COVID-19–related PTSD risk group. This may be related to concern about the health of the infected and the fear of becoming a suspected or confirmed case given their contact level [52]. On the other hand, having experienced direct exposure was not associated with the COVID-19–related PTSD risk group. Previous studies have reported that vulnerability to PTSD is caused by a combination of genetic and environmental factors (gene-environment interaction) [53,54]. Genetics explained 30% of PTSD cases even after controlling for trauma exposure [55]. PTSD symptom manifestations could be different even if the exposure to COVID-19 is the same [54]. Meanwhile, at the time of this study, most third-year medical students got tested the COVID-19 virus test—defined as direct exposure in this study—as a routine screening test for the clinical clerkship at the hospital. Considering the possibility that the association of direct exposure with the COVID-19–related PTSD risk group may have attenuated and disappeared is necessary. Hence, the results need cautious interpretation for ascertaining direct exposure’s association with COVID-19–related PTSD risk group. Moreover, confirming the causality between trauma exposure and the COVID-19–related PTSD risk is difficult in a cross-sectional study, and thus, conducting a large-scale longitudinal study considering various factors including neurobiological and genetic risk factors is necessary to overcome this limitation.
Identifying these sociodemographic and COVID-19–related factors is important to improve prediction and potential prevention strategies [53]. Moreover, we should find ways to address PTSD risk associated with COVID-19 among medical students, including identifying protective factors for the COVID-19–related PTSD risk group. In this study, exhibiting lower resilience increased the likelihood of being in the COVID-19–related PTSD risk group. A previous study among Chinese college students also showed that COVID-19–related stressful experiences and acute stress disorders could be mediated by resilience [54]. Resilience refers to the ability to effectively cope and adapt to adverse situations positively [55,56]. Resilient individuals use positive emotions to alleviate the effects of stress and show differences in their capacity to adapt to a stressful event [55]. This study’s result could be explained as follows: Resilient individuals are more capable of dealing with fears arising from COVID-19 stresses as well as experiencing positive emotions and thoughts, which allows them to actively cope with stress and further mitigate PTSD symptoms.
This study demonstrated that exhibiting lower self-esteem increases the likelihood of being in the COVID-19–related PTSD risk group. This study corresponds with the results of a previous study, which reported that a higher self-esteem score was an independent factor associated with lower levels of psychological distress during the COVID-19 pandemic [57]. Self-esteem was also associated with positive emotions, which protect mental health by controlling the negative effects of stress [58]. Moreover, it was found that people with high self-esteem possess many psychological resources, including tranquility, optimism, and openness [59]. Based on the protective factor model, these positive personal attributes reduce the negative influence of stress [60].
Exhibiting lower social support increases the likelihood of being in the COVID-19–related PTSD risk group. The results of this study are consistent with those of the previous study, which reported that perceived support in close relationships was negatively associated with the intensity of PTSD among general population during the COVID-19 pandemic [61]. Additionally, a cross-sectional study was conducted on healthcare worker to assess the frequency of mental health issues and their association with perceived social support [62]. The results showed that stress was the most common mental health issue and high social support positively affected this group’s mental health during the pandemic [62]. This suggests that close social support is a major factor to maintain mental well-being in the social distancing era. A possible explanation may be offered by the ‘‘stress-buffering hypothesis,’’ according to which social support received when experiencing intense stress may reduce traumatic events’ psychological impact [63]. In other words, social support helps people manage uncertainty and increase the perception of personal control over their lives during the COVID-19 pandemic [64].
These findings suggested specific and feasible approaches for primary prevention of PTSD associated with COVID-19. It is necessary to consider introducing organized lectures and curricula focused on enhancing resilience and self-esteem. Furthermore, institutional measures are needed to provide more social support to medical students.
This study has some limitations. First, we were unable to determine the definite causal relationships between psychosocial factors or psychological variables and the COVID-19– related PTSD risk group because we used a cross-sectional study design. Second, the data were obtained through self-reported questionnaires, which could lead to response bias (i.e., social desirability). Third, although our study showed a relationship between sociodemographic or psychosocial factors and the COVID-19–related PTSD risk group, the possibility of the contribution of underlying factors, including biological or genetic factors, to the COVID-19–related PTSD risk group should also be considered. To overcome these limitations, longitudinal cohort studies are required along with this crosssectional study that can help refine PTSD prediction models and contribute to the design of prevention strategies among medical students during the COVID-19 pandemic. In addition, since this study focused on students from a single medical school, we should be careful in generalizing our results. Further studies of medical students of all grades, including those attending other universities, are needed to compensate for this limitation. Nonetheless, our study exhibits the following strengths. This study was the first to investigate the prevalence of the COVID-19–related PTSD risk group and the sociodemographic and psychosocial factors associated with it among Korean medical students.
In conclusion, this study explored the sociodemographic risk factors and psychosocial protective factors of the COVID-19–related PTSD risk group. This study may provide valuable information to the relevant university and medical school authorities responsible for screening and managing of COVID-19–related PTSD risk group. It is important to find ways to provide medical students with more social support, boost their self-esteem, and help them become resilient to changes in learning style and lifestyle.
Notes
Availability of Data and Material
The datasets generated or analyzed during the study are not publicly available due to privacy or ethical issue but are available from the corresponding author on reasonable request.
Conflicts of Interest
Seung Jae Lee, a contributing editor of the Psychiatry Investigation, was not involved in the editorial evaluation or decision to publish this article. All remaining authors have declared no conflicts of interest.
Author Contributions
Conceptualization: Jimin Lee, Seung Jae Lee, Byung-Soo Kim. Data curation: Jimin Lee, Sung Man Chang, Byung-Soo Kim. Methodology: Jimin Lee, Seung Jae Lee, Seunghee Won, Jungmin Woo. Formal analysis: Jimin Lee, Sung Man Chang, Byung-Soo Kim. Investigation: Jimin Lee, Seung Jae Lee, Seunghee Won, Byung-Soo Kim. Writing—original draft: Jimin Lee. Writing—review & editing: Byung-Soo Kim.
Funding Statement
None