Suicide and Suicide Prevention Awareness in Korea During the COVID-19 Pandemic
Article information

Abstract
Objective
Owing to prolonged social distancing and the resultant isolation, the prevalence of depression and suicidality has increased during the COVID-19 pandemic. This study aimed to investigate the severity of depression and suicidality in Korean community populations and examine their awareness of suicide and suicide prevention during the pandemic.
Methods
This study surveyed a community population in 2020 and 2021, involving 668 participants. We evaluated the severity of depression and suicidality using the Patient Health Questionnaire-9 and Beck Scale for Suicidal Ideation as well as questions about awareness of suicide. We performed a correlation analysis to confirm the association between variables, and compared participants’ suicide awareness according to the severity of depression.
Results
The severity of depression and suicidality in the community population decreased in 2021 compared to 2020. Awareness of the importance of suicide prevention increased in 2021, but the percentage reporting that it is possible decreased slightly. The group with higher depressive symptoms reported a lower possibility of suicide prevention.
Conclusion
Increasing social interest in suicide, as well as awareness of suicide prevention, is important for reducing suicide rates. Suicide prevention campaigns, education, and social policies are needed, particularly during the pandemic.
INTRODUCTION
Suicide is a worldwide public health issue, with approximately 800,000 people dying of suicide each year [1]. Approximately 13.7 per 100,000 men and 7.5 per 100,000 women die from suicide, and these numbers may be lower than the actual number of deaths by suicide due to cultural factors and variations in monitoring methods [2]. South Korea has the highest suicide rate among all OECD countries, and according to a report by Statistics Korea, 13,195 people died by suicide in 2020 (men: 35.5 per 100,000, women: 15.9 per 100,000) [3]. The same report added that suicide is the fifth leading cause of all deaths, the first leading cause among people aged 10–40 years, and the second leading cause among those in their 40s and 50s. Suicidal behavior not only negatively affects individuals but also the people around them. The family, friends, and coworkers of a deceased person may also experience major emotional difficulties [4-6]. Although many efforts to prevent suicide are being made in Korea, the high suicide rate remains an unresolved social problem.
The risk of suicide is related to a variety of factors, including demographic, psychopathological, and environmental ones [7-11]. Women are more likely to have suicidal thoughts and attempts than men; however, suicide mortality is higher in men than in women [10,12]. Mental disorders, such as depressive disorder, bipolar disorder, and schizophrenia, increase the risk of suicide, and the risk is higher in untreated patients [7,13-15]. Some environmental factors may increase the risk of suicide. In Korea, there is a stigma toward suicide and depression, which discourage high-risk patients from visiting psychiatric clinics [11]. Changes in an individual’s environment, such as social isolation, economic difficulties, and job loss, may also negatively affect depressive disorders and increase the risk of suicide [9].
The COVID-19 pandemic has significantly affected the living environment of millions of people worldwide [16,17]. Social distancing, working from home, and school closures were implemented suddenly, leading to a monumental increase in the number of people who lost their jobs due to work disruption [18]. Compared to the period before the pandemic, the time spent indoors increased, and the number of social meetings decreased worldwide, including in South Korea. In February 2020, with the spread of COVID-19, school closures were implemented and employees had to change their work patterns to work from home. The number of socially isolated people has increased, and they have been emotionally exhausted by the prolonged pandemic. Social anxiety caused by the infection of family and acquaintances and the risk of mental health problems has increased [18]. Furthermore, stressful experiences such as social isolation, depression, anxiety, and economic uncertainty during the pandemic have increased suicidal risk. To counter this threat, awareness campaigns and educational programs have been suggested as universal interventions to prevent suicide in the general population. [18,19]. Raising awareness of the risk and protective factors of suicide as well as providing information on where to receive help is effective in preventing suicide.
This study aimed to assess the public’s views on suicide and suicide prevention during the COVID-19 pandemic. A survey was conducted on a community population in 2020 and 2021 during the pandemic period. This study investigated the awareness of suicide, the possibility and importance of suicide prevention, and suicide prevention methods in the community. The study hypotheses were as follows: 1) the severity of depressive symptoms and suicide risk in the general population have increased during the pandemic; 2) people with depressive symptoms perceive that suicide prevention is less likely; and 3) the frequency of contact with acquaintances is related to the severity of depression. In addition, this study examined the methods suggested by the local community population to prevent suicide and identified robust measures for suicide prevention within the community.
METHODS
Participants
A survey was conducted on the adult community population aged 19 years or older living in Ansan-si, a satellite city in Seoul, in 2020 and 2021. The survey was conducted both online and offline by the Ansan Suicide Prevention Center through a questionnaire prepared using Google Forms. An offline survey was conducted among those who participated in suicide prevention education and publicity campaigns for the general population held at universities and public places. After receiving an explanation on how to fill out the questionnaire on-site, the participants were directly connected using a QR code to answer the questionnaire. The online survey was advertised via posters placed in public places, such as hospitals, libraries, universities, large bookstores, and online advertisements using social network services. The participants received sufficient explanation, including the purpose and methods of the study, before answering the questionnaire, and those who agreed to participate were included in the study. A total of 353 participants from the first survey (June 26 to November 22, 2020) and 315 participants from the second survey (March 5 to October 16, 2021) were included in this study. Participants who did not complete the questionnaire were excluded, and 637 participants were included in the analyses.
Clinical measures
Demographics and awareness of suicide
Sociodemographic information, such as age, sex, employment status, and personal relationships, was collected. Participants completed questionnaires related to suicide and suicide prevention, which comprised five multiple-choice questions. The suicide awareness questionnaire used in the survey was prepared by the Ansan Suicide Prevention Center based on the contents of the suicide awareness and attitude survey questionnaires used in previous studies in Korea [20,21]. This study investigated the general population’s awareness of the importance and possibility of suicide prevention, groups that should make an effort to prevent suicide, the level of contact with acquaintances, and the effect of contact with acquaintances on suicide prevention. The importance of suicide prevention was investigated using the question “Do you think your own suicide or that of those around you must be prevented?” and participants’ responses were classified as follows: “agree,” “unsure,” “disagree,” and “indifferent.” Unlike previous studies, we included an “indifferent” response item to identify the percentage of people who were indifferent to suicide itself. The question on the groups that should make an effort to prevent suicide consisted of eight items: psychiatrist, counselor, family, friends, police, 119 rescue teams, general population, and others. Detailed information regarding the questions used in the survey is presented in Table 1.

Questionnaire related to suicide and suicide prevention
Depressive mood and suicidality
The Patient Health Questionnaire-9 (PHQ-9) and Beck Scale for Suicidal Ideation (SSI) were used to evaluate participants’ degree of depressive mood and suicidal ideation. Han et al. [22] translated and validated the Korean version of the PHQ-9, which consists of nine items measured on a four-point Likert scale. Han et al. [22] suggested 5 points as a screening score for depressive disorder, and scores above 5 were classified as follows: 5–9, mild depression; 10–19, moderate depression; and 20–27, severe depression. A cutoff score of 10 (total score of PHQ-9) was suggested to differentiate the major depressive disorder (MDD) group from the non-MDD group [23]. Beck et al. [24] developed the SSI to measure suicidal ideation and severity. The SSI is a 19-item self-report inventory with each item on a three-point scale ranging from 0 to 2. The total score ranges from 0 to 38; the higher the score, the higher the severity of suicidal ideation. Lee and Kwon [25] validated the Korean version of the SSI using a Korean sample, and identified two primary factors: “active suicidal ideation” and “ambivalent attitude toward suicide. In his study, Cronbach’s alpha for the SSI was 0.74.
Statistical analysis
Pearson’s chi-square test and Student’s t-tests were used to compare socioeconomic information (e.g., sex, age, and job), the severity of depressive mood and suicidal ideation, and awareness of suicide prevention among the participants in 2020 and 2021. We also compared the variables according to the perception of the possibility of suicide prevention and investigated the correlation between age, depressive mood (PHQ-9), suicidal ideation (SSI), and awareness of suicide prevention using a correlation test. Spearman’s correlation test was used because the variables did not follow a normal distribution and contained nominal variables. We compared the awareness of suicide prevention according to depressive symptoms (MDD group and non-MDD group) and sex using Pearson’s chi-square test and Student’s t-test. All statistical analyses were performed using the Statistical Package for the Social Sciences 26.0 (IBM Co., Armonk, NY, USA).
Ethics statement
The study protocol was approved by the Institutional Review Board of Korea University Medical Center, Ansan Hospital, Gyeonggi-do, Korea (No. 2020AS0138). All participants provided informed consent for online or offline participation.
RESULTS
Sociodemographic characteristics
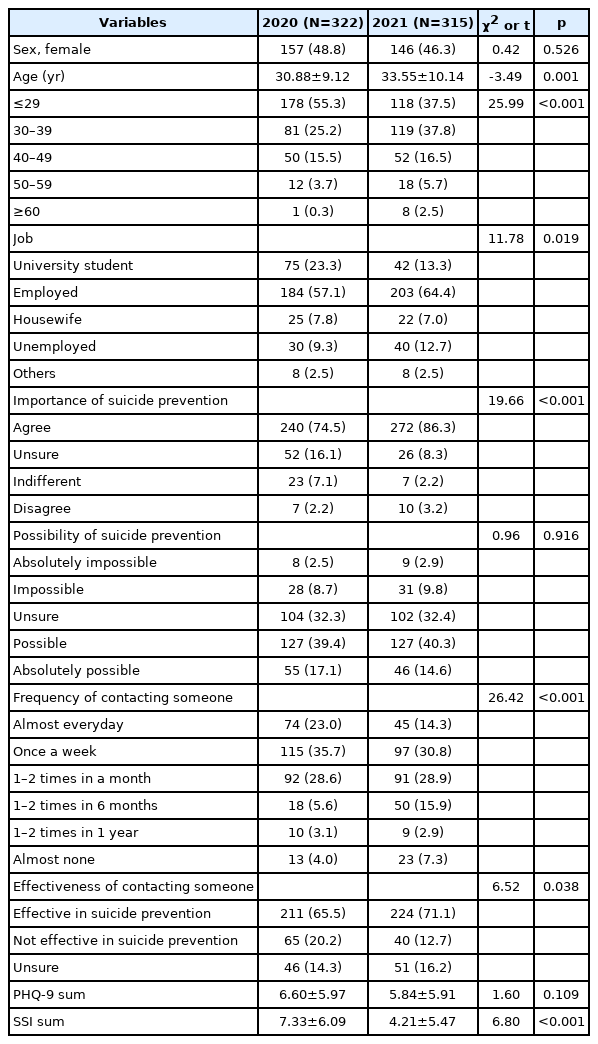
Although more males than females participated in both 2020 and 2021, the difference was not statistically significant. Mean ages were 30.88±9.12 years in 2020 and 33.55±10.14 years in 2021, respectively, and the mean age of participants in 2021 was significantly higher. Job status was in the order of employed, university students, and unemployed; however, there was a significant difference in the percentage of job status between 2020 and 2021. Regarding awareness of suicide, the proportion of those who thought that suicide should be prevented increased from 74.8% in 2020 to 86.3% in 2021, but the ratio of those who responded that suicide prevention was (absolutely) possible slightly decreased from 56.5% to 54.9%. The sum of the PHQ-9 scores decreased, and the ratio of participants who reported the presence of depressive symptoms increased (58.4% in 2020 and 49.8% in 2021), but the difference was not statistically significant. The total SSI scores decreased significantly in 2021 compared with those in 2020. The proportion of participants who responded that suicide should be prevented was significantly higher among females than males (males: 77.2%, females: 83.8%). The response rate for reporting that suicide prevention was (absolutely) possible was also higher among females, but this difference was not statistically significant (males: 53.9%, females: 57.8%). The number of participants who reported contacting their acquaintances once a month was the largest in both 2020 and 2021, and the rate of reporting that contacting someone was effective in preventing suicide significantly increased from 65.5% to 71.1% (n=211 in 2020 and n=224 in 2021) (Tables 2 and 3).
Demographic data and awareness of suicide
Comparison of variables according to the possibility of suicide prevention
Comparison of variables according to the possibility of suicide prevention
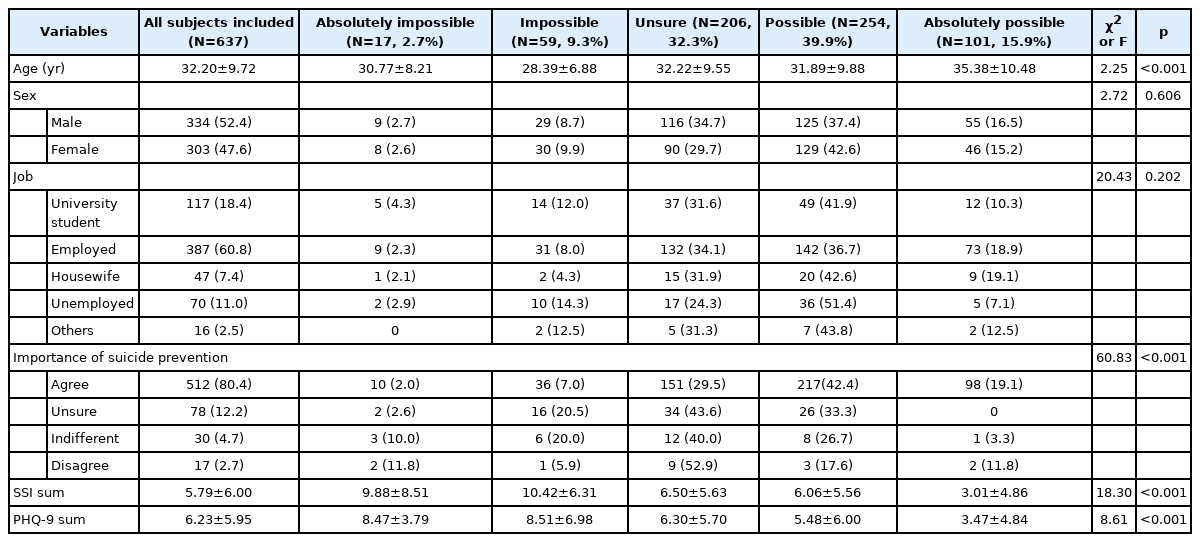
The participants were divided into five groups as follows: “absolutely impossible,” “impossible,” “unsure,” “possible,” and “absolutely possible.” Of the participants, 55.8% answered that suicide prevention was (absolutely) possible, and 12.0% answered that it was (absolutely) impossible. One-third of the participants reported that they were unsure about the possibility of suicide prevention. The mean age of the group that answered that suicide prevention was absolutely possible was the highest, and the group without employment had the highest rate of reporting that suicide prevention was impossible. The total SSI and PHQ-9 scores were higher in the group that reported that suicide prevention was (absolutely) impossible (Table 3).
Awareness of suicide prevention by severity of depressive symptoms
We compared the two groups by dividing them into MDD and non-MDD groups based on the PHQ-9’s cut-off point of 10. The non-MDD group was 488 (76.6%) and the MDD group was 149 (23.4%). There was a significant difference in the awareness of suicide between the two groups. The non-MDD group tended to report that suicide should be prevented, and the rate of reporting that suicide prevention was (absolutely) possible was higher than that of the MDD group (60.3% vs. 40.9%). The total score of SSI was also significantly higher in the MDD group (12.30±7.14) than in the non-MDD group (3.80±3.81). The non-MDD group reported a higher rate of contact more than once per week (54.1% vs. 45.0%). In the MDD group, 36 participants reported no contact with people around them (12.8%).
A similar tendency was also observed when the participants were divided into four groups based on the sum of their PHQ-9 scores: no depressive mood (n=292, 45.8%), mild depression (n=196, 30.8%), moderate depression (n=127, 19.9%), and severe depression (n=22, 3.5%). In all, 89.0% of the group without depressive symptoms reported that suicide should be prevented, whereas only 54.5% of the group with severe depressive symptoms reported that suicide should be prevented. Regarding the possibility of suicide prevention, the results confirmed that the higher the depressive symptoms, the lower the possibility of suicide prevention. The results of the comparison between the groups according to the severity of depressive symptoms are presented in Table 4 and Supplementary Table 1 (in the online-only Data Supplement).

Demographic data and awareness between MDD group and non-MDD group
Correlations among awareness of suicide, depressive mood, and suicidality
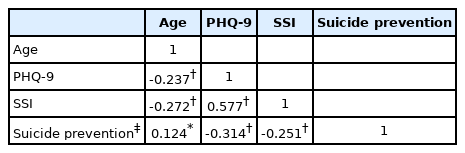
The results indicated that the severity of depressive mood and suicidality decreased with increasing age and that there was a correlation between age and the possibility of suicide prevention. In contrast, the possibility of suicide prevention and the severity of depressive mood were negatively correlated. The more depressed the participants, the more they recognized that suicide could not be prevented. Similarly, the possibility of suicide prevention and the sum of the SSI scores showed a negative correlation. The results of the correlation analysis were statistically significant (Table 5).
Correlation coefficients between age and PHQ-9 scores, SSI scores, and the possibility of Suicide prevention
DISCUSSION
The present study aimed to identify the severity of depressive mood, suicide ideation, and awareness of suicide prevention in a community in Korea using community surveys during the COVID-19 pandemic. We hypothesized that the severity of depressive mood and the risk of suicide would increase due to the worsening of the COVID-19 pandemic in 2021 compared to 2020 in Korea; however, contradictory results were found, and there was a statistically significant decrease in the sum of the PHQ-9 and SSI scores in 2021 compared to 2020. These results possibly reflect the adaptation to lifestyle changes as the COVID-19 pandemic progressed. With the onset of the COVID-19 pandemic in 2020, major changes occurred in the daily lives of individuals. Social distancing was enforced, and opportunities for outdoor activities were reduced. School, college, and university schedules were also delayed or classes were conducted online to reduce the risk of infection. Overall, increased indoor activity time has led to high levels of stress in the population [17,26]. As the pandemic raged, anxiety and depression in the general population increased, and a new term “corona blue,” a compound word of “coronavirus” and “blue,” appeared in Korea in 2020. According to data provided by Statistics Korea, the number of confirmed COVID-19 cases has increased significantly in 2021 compared to 2020 [27]. However, with time, people began to adapt to this new lifestyle, which may have improved their emotional states. In a longitudinal observational study of adults conducted in England, Fancourt et al. [28] examined the trajectory of anxiety and depressive symptoms during the pandemic. They suggested that the highest levels of depression and anxiety occurred in the early stages of the pandemic, and depressive and anxiety-related symptoms tended to decrease over time, possibly because individuals adapted slowly to their circumstances. Additionally, a changed lifestyle may have had a positive effect on the emotional status of individuals. In a qualitative study that conducted a thematic analysis of seven study participants in Korea, the positive and negative effects of working from home during the COVID-19 pandemic on family life experiences were evaluated [29]. In this study, Cho and Kim [29] suggested positive aspects such as increased free time due to a decrease in commuting time, increased emotional intimacy due to spending more time with family members, increased time spent between husband and wife, and an increase in understanding between family members. The low proportion of unemployed participants in 2020 and 2021 may have influenced our findings. In previous studies, emotional difficulties have increased because of health concerns and the risk of infection during the pandemic, and job insecurity has also negatively affected the severity of depression and anxiety [30,31]. In a study of 18–26-year-old young adults in the United States, more than 50% of the participants experienced employment loss either directly or indirectly, which was associated with poor mental health [31]. However, in our study, the proportion of unemployed people was similar in 2020 and 2021, and factors related to job instability may not have been reflected in the results.
In the correlation analyses of awareness and other variables, awareness of suicide prevention was inversely correlated with depressive symptoms and suicide risks. The group without depressive symptoms had a higher rate of reporting that suicide prevention should be prevented and that suicide prevention is possible compared with the group with depressive symptoms. Depressive symptoms can also affect individuals’ acceptance of suicide and vice versa. Therefore, more awareness campaigns and education on suicide prevention are needed for populations with depressive symptoms. For those with suicidal thoughts or intentions, not only the treatment of mental illness but also the attention of people around them and social interests are very important. Therefore, suicide prevention education for the general public is necessary. In a German study, van der Burgt et al. [32] reported that those who had attended a suicide prevention campaign were more familiar with suicide prevention and were more open to seeking professional psychological help. In the same study, campaign exposure was more pronounced in the group under 25 years of age [32]. It may take time to create a social atmosphere for suicide prevention; however, education on the importance and methods of suicide prevention and eliminating social prejudice against mental illness and suicide may help reduce suicide rates in the community. Wasserman et al. [19] suggested increased availability of telemedicine and digital tools as factors for suicide prevention at the social level during the pandemic. In Korea, mental health management centers, including suicide prevention centers, conduct telephone counseling for isolated individuals to prevent suicide. In this context, lifestyle management at the individual level is also important, and a campaign to promote proper diet, sleep, and exercise during a pandemic is needed.
The COVID-19 pandemic has led to the emergence of several risk factors for suicide, including a decline in mental health, depression, loneliness, domestic violence, anxiety, and fear. The occurrence and/or aggravation of depression during the pandemic has increased the risk of suicide [33]. Previous studies have reported that the suicide rate has increased among the general population and medical staff during the pandemic, with an increase in the risk of self-harm [34,35]. Depressive disorder is a risk factor for suicide, and more severe depressive symptoms increase the risk of suicide [34,35]. Although refractory and/or untreated depression increases the risk of suicide, many patients refuse psychiatric treatment because of social prejudice against mental illness [7,8]. Some socially isolated people may be unaware of depression and may have experienced worsening symptoms because opportunities for contact with others decreased during the pandemic. Social support, a sense of belonging, and stable employment have been identified as protective factors for preventing suicide [36]; however, these factors were threatened during the pandemic. In contrast, risk factors for suicide, such as sudden environmental changes, mental health problems, and isolation, have increased [9,36]. Social distancing and restriction of outside activities can cause profound loneliness, depression, and suicidality, especially in older adults. Social awareness campaigns can induce positive changes in attitudes toward depression and help-seeking behavior [37], which can help individuals at risk for suicide receive appropriate professional treatment. Similar to our results, a previous study reported that suicidal ideation was associated with negative attitudes toward help-seeking behavior, and lower depressive symptoms, older age, and female gender were associated with positive attitudes toward help-seeking intentions and behaviors [38]. Implementing mental health and suicide prevention education for the general population with and without depressive symptoms is important to lower the suicide rate. In particular, patients with depression or suicidal thoughts may refuse professional treatment; therefore, active intervention from those around them is necessary. The lack of existing suicide prevention education may have contributed to the increase in suicide rates during this pandemic. In the future, a pandemic may occur owing to the spread of certain infectious diseases, and efforts such as education and campaigns are needed to improve awareness of suicide prevention as a preventive measure.
Although the present study reveals important findings, it has some methodological limitations that should be considered. First, online self-report measures might have led to reporting bias, such as desirability bias. Second, participant bias may have occurred because those who participated in the study or the campaign and education conducted by the Ansan Suicide Prevention Center or were interested in suicide prevention might have been included. In addition, the fact that the average age of the participants in 2021 was relatively higher than that of the participants in 2020 may have influenced the results. Older people tend to have a relatively more positive attitude towards suicide prevention [38]. Caution is needed in interpretation because of the biases mentioned above [37,38] Third, questions about the direct impact of COVID-19 and some variables related to suicide risk were not examined. Factors such as a history of mental illness, change in economic status and relationships with family members may impact mental health and suicide awareness, especially in the context of the COVID-19 pandemic [33]. Although employment status was investigated in this study, detailed information, including the type of employment and job, duration, and salary, could not be confirmed. Fourth, a standardized tool was not used to investigate the awareness of suicide prevention. Fifth, this cross-sectional study was conducted in 2020 and 2021, targeting the population of a single city. Our results may not be representative of Korean society, and a causal relationship cannot be drawn.
Nevertheless, this study has strengths in that it identified the changes in depression and suicide risk in the general population during the COVID-19 pandemic and evaluated their impact on suicide awareness. Although social interest is recognized as important for suicide prevention, comprehensive studies on the general public’s awareness of suicide prevention are lacking in South Korea. Future research should include diverse variables that may influence suicide, such as educational level, nationality, income, job, and personality.
In conclusion, the present study identified the awareness of suicide prevention in a community population in Korea during the COVID-19 pandemic. Suicide is both a personal and social problem. To prevent suicide, appropriate treatment of mental illness and management of daily life are required at the individual level, and efforts to reduce social prejudice against suicide and mental illness are necessary at the social level. Along with suicide prevention campaigns and education, social policies should aim to prepare and enable individuals to recognize the risk of suicide in those around them and provide appropriate help. Social interest in suicide and increased social awareness can lead to reduced suicide rates. The results of this study confirmed that the role of people around an individual is important for suicide prevention, and education and campaigns around the same need to be encouraged.
Supplementary Materials
The online-only Data Supplement is available with this article at https://doi.org/10.30773/pi.2022.0108.
Awareness of suicide according to the severity of depressive symptoms
Notes
Availability of Data and Material
The datasets generated or analyzed during the study are available from the corresponding author on reasonable request.
Conflicts of Interest
The authors have no potential conflicts of interest to disclose.
Author Contributions
Conceptualization: Jongha Lee, Rayoung Han, Ho-Kyoung Yoon. Data curation: Jongha Lee, Rayoung Han, Nayoung Chae. Formal analysis: Jongha Lee, Cheolmin Shin, Nayoung Chae. Funding acquisition: Ho-Kyoung Yoon. Methodology: Jongha Lee, Cheolmin Shin, Young-Hoon Ko, Ho-Kyoung Yoon. Supervision: Ho-Kyoung Yoon. Writing—original draft: Jongha Lee, Ho-Kyoung Yoon. Writing—review & editing: Jongha Lee, Young-Hoon Ko, Ho-Kyoung.
Funding Statement
This study was supported by the National Research Foundation (NRF2020R1A2C1008072) of the Republic of Korea and a Korea University Ansan Hospital Grant (O2207191). The funders had no role in the design and conduct of the study or the decision to submit the article for publication.