A Latent Class Analysis of Suicidal Behaviors in Adolescents
Article information

Abstract
Objective
The purpose of the present study was to identify adolescents’ suicide subgroups using five indicators (depression, anxiety, suicide ideation, and planned and attempted suicide), and explore the distinctive features of each subgroup.
Methods
This study included 2,258 teenagers from four schools. Both adolescents and their parents, who voluntarily agreed to participate in the study, completed a series of self-reported questionnaires on depression, anxiety, suicide, self-harm, self-esteem, impulsivity, childhood maltreatment, and deviant behaviors. The data were analyzed using latent class analysis, a person-centered method.
Results
Four classes were detected: “high risk for suicide without distress,” “high risk for suicide with distress,” “low risk for suicide with distress,” and “healthy.” The “high risk for suicide with distress” class was the most severe on all evaluated psychosocial risk factors, namely, impulsivity, low self-esteem, self-harming behaviours, deviant behaviour problems, and childhood maltreatment, followed by “high risk for suicide without distress.”
Conclusion
This study identified two high risk subgroups for adolescent’ suicidality, “high risk for suicide with or without distress.” Both high risk subgroups for suicide showed higher scores for all psychosocial risk factors than low risk subgroups for suicide. Our findings suggest that special attention needs to be paid to the latent class “high risk for suicide without distress,” as this group’s “cry for help” might be relatively difficult to detect. Specific interventions for each group (e.g., distress safety plans for “suicidal potential with or without emotional distress”) need to be developed and implemented.
INTRODUCTION
Teenage suicide is a growing public health concern; it is the second and third leading cause of death for females and males, respectively [1], and the first in South Korea (Korean National Statistics, 2019). Suicide ideation, planning, and attempts are immediate precursors of “death by suicide” and increase dramatically in teenage years [2,3]. Particularly, suicide ideation is significantly associated with future attempted suicide, and previous attempted suicide is a strong predictor of future death by suicide [4,5]. Other important indicators closely related to suicidal behaviour in adolescents are depression and anxiety.
We use the terminology of suicide and suicide behaviours based on the definition by the previous work [6-9]. Suicide is defined as the act of intentionally ending one’s life. The terminology of suicidal behaviours is used and classified into three categories: suicidal ideation, suicide plan, and suicide attempt. Depressive and anxious mood are known to be significant predictors of suicide behaviours [10-13]. However, not all individuals with depression and/or anxiety are at high risk for suicidality. As Lewinsohn, Rohde and Seeley suggested [14], there might be adolescents with low severity of depression or anxiety. Although aforementioned variables are well-known predictors of suicidal behaviour, most previous studies have mainly conducted variable-centered research, which is unable to identify specific features of individuals at increased suicidal risk. With latent class analysis (LCA), different types of individuals presenting suicidal behaviour can be detected, which can help to develop individually tailored preventive strategies and interventions.
On the other hand, previous research has identified crucial risk factors of suicidal behaviours in adolescents. For example, as an individual’s behaviour trait, impulsivity appeared to be higher in both suicide ideators and attempters than in nonsuicidal individuals in a study with adults [15], and similar results have been reported in adolescents [16,17]. Another individual characteristic related to suicidal behaviour in adolescents is self-esteem; low self-esteem in adolescents was significantly associated with suicidal ideation and attempts [18]. In particular, Chatard et al. [19] noted that suicide rates were higher in nations characterized by lower self-esteem among individuals (i.e., Asia) than in those where citizens have higher self-esteem. Adolescents’ deviant behaviour problems such as violence, peer victimization, bullying, and alcohol and substance use have been identified as significant proximal risk factors for suicidal behaviours [20-23]. Non-suicidal self-injury, known to be the strongest proximal risk factor predicting suicidality, is most common in adolescents [24,25]. Childhood adversity, such as physical and sexual abuse or neglect, is also a critical distal factor of suicidal behaviours in adolescents [22,26-28].
Taken together, previous research findings suggest that suicide ideation, planning, and attempts along with depressive and anxious mood are crucial indicators of suicidal behaviours. While we note that there are a handful of studies investigating subtypes of adolescents with suicidal behaviours using LCA, most of them did not include suicide indicators (e.g., suicide ideation, and planned and attempted suicide) and mood indicators (e.g., sad and anxious mood) together. Two studies so far have considered sad or anxious mood as risk indicators when identifying subtypes of adolescents’ suicidality [29,30]. However, Jiang et al. [30] did not include anxious mood in the analysis and Ginley and Bagge [29] analysed psychiatric patterns including depressed and anxious mood among only recent suicide attempters, not suicide ideators or planners. As noted in previous studies showing the strong association of adolescents’ suicidality with both depressed and anxious mood, and given that suicide ideation, plans, and attempts are also significantly related to each other, it is of great importance to consider and analyse both mood and suicidal indicators together to categorise adolescents’ suicidality. Furthermore, in clinical observations it is often observed that sudden suicide may occur without any emotional precursor such as depression or anxiety. Therefore, it is important to investigate whether or not such individuals exist as a latent group with high risk of suicidality. As such, using LCA, the present study aimed to categorise adolescent suicidal behaviour using five indicators: suicide ideation, planned suicide, attempted suicide, and depressive and anxious mood. Additionally, we aimed to investigate which groups are more likely to have severe risk features, thus requiring active intervention. The main questions of the present study were as follows: 1) how many different classes of adolescent suicide-related behaviour exist? and 2) how do the identified classes differ in terms of suicide risk factors (impulsiveness, self-esteem, deviant behaviour problems, childhood maltreatment, and self-harm)?
METHODS
Participants and procedure
The design of the present study was cross-sectional research. A total of 2,753 adolescents from four schools in two big cities, Seoul and Gyeonggi-do, were provided detailed information about the study, and 2,258 adolescents and their parents voluntarily agreed to participate and provided informed written consent. Participants were then asked to complete a packet of a paper and pencil version of the self-reported questionnaires at school. The average duration to complete the survey was 15 min. The Institutional Review Board of Catholic University of Korea reviewed and approved the study protocol (IRB No. UC15QISI0073).
Measures
Suicide risk indicators
The following six self-report items were used: 1) During the past 12 months, did you ever seriously think of attempting suicide (suicide ideation)?; 2) During the past 12 months, did you make a specific plan about how you would attempt suicide (planned suicide)?; 3) During the past 12 months, did you actually attempt suicide (attempted suicide)?; 4) During the past 12 months, did you feel so depressed almost every day for 2 weeks or more in a row that you stopped doing some usual activities (depressed mood)?; 5) During the past 12 months, did you feel a markedly diminished interest or pleasure in everything or almost everything (anhedonia)?; and 6) During the past 12 months, did you feel excessive anxiety or worry occurring for 1 month or more (anxiety)? Participants answered “yes” or “no” to the questions about suicide ideation, planned suicide, depression, and anxiety. The question about attempted suicide used a 4 point-scale to assess frequency (0 times, 1 time, 2 or 3 times, and 4 or more times). The items used in the present study were taken from the Youth Risk Behaviour Survey (YRBS) by the Center for Disease Control and Prevention and from the Suicidal Behaviour Module of the World Health Organization Composite International Diagnostic Interview [31]. Previous studies reported good reliability, and convergent and discriminant validity [32-34].
Suicide risk factors
Impulsivity was measured using 3 items from the Barratt Impulsivity Scale originally developed by Barratt [35] and vali dated by Lee et al. [36]. For the current sample, Cronbach’s alpha was 0.73.
Self-esteem was measured using five positively worded items from the Rosenberg Self-esteem Scale [37]. This scale has shown good reliability [38]. In the current sample, Cronbach’s alpha was 0.87.
Childhood maltreatment was measured using eight items originally developed by Pennebaker and Susman [39]. Items are rated on a 4-point Likert scale. Cronbach’s alpha in the current sample was 0.76.
Deliberate self-harm was measured using three items (cutting, burning, and head banging) included in the Inventory of Statements About Self-injury [40]. Participants were asked to indicate how many times they had intentionally engaged without lethal intent in each of the behaviours listed during the past 12 months. The scale has shown good internal consistency and construct validity [40,41].
Deviant behaviour problems included leaving home without notice, truancy at school, violence, peer victimization, bullying (including cyberbullying), and alcohol and substance problems experienced during the past 12 months, and were measured using 15 items developed by the National Youth Policy Institute [42]. All items were rated on a 5-point scale (never, 1 time, 2–3 times, 1–2 per week, every day). Cronbach’s alpha for the current sample was 0.79.
Data analysis
LCA was conducted using Mplus 8 [43]. To determine the best number of latent classes, Akaike’s information criterion (AIC) [44], Bayesian information criterion (BIC) [45], and sample-size adjusted BIC (saBIC) [46] were included as information criteria indices. Likelihood ratio tests were judged using the Lo-Mendell-Rubin likelihood ratio (LMR LR) Lo et al. [47] and bootstrapping likelihood ratio test (BLRT). Relative entropy-based normalization was used to assess the precision of latent class assignment [48]. Smaller values of AIC, BIC, and saBIC indicate better fitting of a model. Entropy values of 0.80 or higher indicate clear classification. Statistical significance of LMR LR and BLRT tests (e.g., p<0.05) are desirable. Subjects were classified into latent classes based on posterior probabilities derived from LCA parameters with the modal assignment rule, in which each case is assigned to the latent class with the highest posterior membership probability. The Kruskal-Wallis H test was performed followed by Dwass, Steel, Critchlow-Fligner (DSCF) multiple comparisons to compare psychosocial risk factors among the classified participants. This method is considered as a nonparametric alternative to the one-way ANOVA under the condition that the assumption of normality is violated for the given data.
RESULTS
Participant characteristics
Of 2,258 teenagers, 55.0% (n=1,242) were male, 44.8% (n=1,012) female, and 0.2% (n=4) did not respond. Mean of age was 16.47. All the participants were of Korean nationality. The descriptive statistics for the democratic and study variables were given in Table 1.
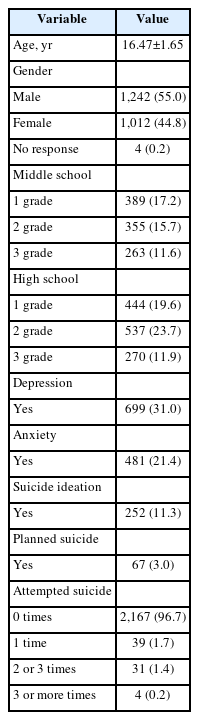
Sample characteristics (N=2,258)
Number of latent classes
Indicators in the LCA were depressed mood, anxious mood, suicide ideation, planned suicide, and attempted suicide. The fit indices of the latent classes are presented in Table 2. All values for AIC, BIC, and saBIC in the three-class model were lower than those in the two-class model. The four-class model had a lower AIC value and higher BIC and saBIC values than the three-class model, and the LMR LR and BLRT p-values were still significant, with a higher value of entropy. The five-to seven-class models showed increasingly higher values of AIC, BIC, and saBIC, with non-significant LMR LR p-values. The four-class model yielded the two classes including less than 5% of the respondents, suggesting the possibility of spurious classes. However, considering the low rate of suicidal behaviors, it is natural to have such small classes in the model. Otherwise, it can possibly oversimplify the heterogeneity in a population. Consequently, we chose a four-class model as the optimal model for the present study based on the statistical criteria and interpretability of the model.
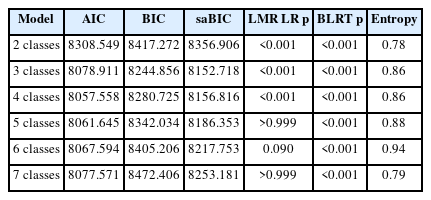
Fit indices of latent class models
The first latent class (LC1) included 33 students (1.6%) with the highest probability of suicide ideation and planned and attempted suicide, but low probability of depressed and anxious mood. This class was named “high risk for suicide without distress.” The second latent class (LC2) included 60 students (3.4%) with the highest probability of depressed and anxious mood among all latent classes and high probability of suicidal ideation and planned and attempted suicide that were slightly lower than the first class. This class was labelled “high risk for suicide with distress.” The third class (LC3) contained 382 students (20.8%), who showed the second-highest probability of depressive and anxious mood. However, the third class showed a relatively lower probability of suicidal ideation and planned and attempted suicide than the first and second classes. Hence, the third latent class was defined as “low risk for suicide with distress.” The last class (LC4) included 1,783 students (74.1%) and was defined as “healthy,” showing the lowest probability of all five suicide risk indicators. Table 3 and Figure 1 present detailed information of the model.

Endorsement of depression, anxiety, suicide ideation, planned suicide and attempted suicide by class
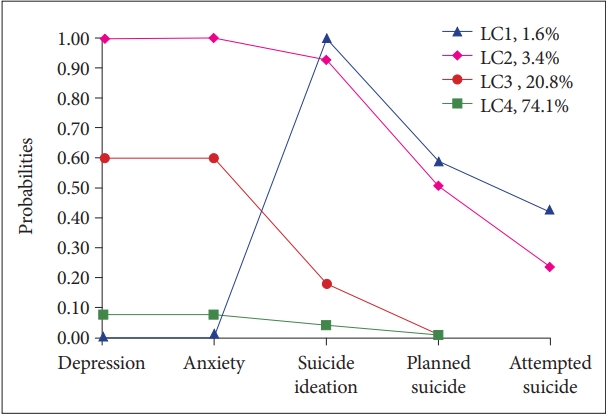
Line graph of conditional response probabilities comparing latent class profiles on depression, anxiety, suicide ideation, planned suicide, and attempted suicide. LC, latent class.
Differences in psychosocial risk factors by class
Preliminary analysis revealed that psychosocial risk factors were heavily skewed to the right, with z-scores for skewness ranging from 1.6 to 32.8. Given this nonnormality of data, class differences in psychosocial risk factors were examined using the Kruskal-Wallis H test, which is the nonparametric alternative to one-way ANOVA. Additionally, multiple DSCF comparisons were performed to identify specific class differences for multiple tests.
As shown in Table 4, each class was significantly different from each other in all risk factors, namely, deviant behaviour problems, childhood maltreatment, self-harm, self-esteem, and impulsivity (all p<0.001). LC2, high risk for suicide with distress, appeared to be the most distinguishing on all measures compared with the remaining three groups. More specifically, individuals in this class reported the highest levels of deviant behaviour problems and self-harm, followed by LC1. LC3 and LC4 did not differ between each other in levels of deviant behaviour problems or self-harm. Childhood maltreatment in LC2 was higher than in LC1, and LC3 was higher than in LC4. LC4 showed the highest self-esteem among all latent classes, followed by LC1 and LC3, whereas LC2 presented the lowest self-esteem. The results also revealed that LC2’s impulsivity was relatively higher than that of LC1. Similarly, the impulsivity level of LC3 was higher than that of LC4, but no difference was found between LC1 and LC3. Table 4 presents the results in detail.

Class differences in psychosocial risk factors
DISCUSSION
Identifying distinctive subgroups of adolescents’ suicidality and exploring differential characteristics of each high-risk subgroup is of great importance for preventive interventions. In this sense, the present study, as an exploratory research, sought to categorize adolescents’ suicidality using the LCA and investigate group differences on a series of risk factors, namely, impulsivity, self-esteem, childhood maltreatment, self-harm, and deviant behaviour problems. Key findings were as follows. Firstly, an LCA identified four subgroups: high risk for suicide without distress, high risk for suicide with distress, low risk for suicide with distress, and healthy. Secondly, two subgroups, high risk for suicide without distress and high risk for suicide with distress typified the highest risk of adolescent’s suicidality. Thirdly, these two subgroups differed significantly in terms of all psychosocial risk factors (impulsivity, self-esteem, childhood maltreatment, self-harm and deviant behaviour problems); the high risk for suicide with distress subgroup showed higher scores on all the psychosocial variables than did the high risk for suicide without distress subgroup.
Importantly, the present study identified two different highrisk groups for suicide. In particular, high risk for suicide without distress (1.6%, 33/2,258) is of great interest. This subgroup showed the highest risk of suicide ideation and planned and attempted suicide but low probability of depression and anxiety. Consistent with the results obtained by Lewinsohn et al. [14], our results point to the critical message that adolescents’ suicidality is not necessarily accompanied by depression or anxiety. Adolescents classified as having a high risk for suicide without distress did not subjectively manifest depression and anxiety, which are known warning signs of a suicide. Unless suicide measurements are used, it might be difficult for family members, school teachers, and school counselors to identify these adolescents as having the highest risk of suicidality, and timely intervention might not be offered in the absence of a “cry for help.” Also, from a psychopathology viewpoint, 1.6% of the sample assigned to this class might correspond to prevalence rates of psychotic-spectrum disorders or eating disorder in adults. Future research is warranted to check whether this subgroup is explained by the features of psychotic spectrum disorders or eating disorder.
On the other hand, high risk for suicide without distress showed some similar patterns to that of of the third latent class (LC3) identified by Jiang et al. [30] Adolescents in LC3, as shown in Jiang et al. [30], also displayed the lowest probability of feeling sad or hopeless but the highest probability of attempted suicide. However, the proportion of adolescents who considered and planned suicide was low. Some in this group were those who physically forced to have sexual intercourse and those who felt unsafe going to or being at school. Ginley and Bagge [29] also classified adult suicide attempters into three groups. Suicide attempters in the LC3 shown in this study displayed high levels of antisocial personality disorders, alcohol and substance use but lower levels of depression and anxiety. As shown in the post-hoc analyses in the present study, adolescents at high risk for suicide without distress (LC1) also reported high levels of deviant behavior problems such as alcohol and substance use, truancy at school, violence, peer victimization, and bullying (including cyberbullying). Based on these results, we presume that the LC1, high risk for suicide without distress might be a specific group with externalizing disorders who are at risk for adolescent suicidality. Another possibility to consider for this group is those with personality pathology or perhaps adolescents with poor insight into their symptoms or those who do not want to report their symptoms due to fear of stigmatization for psychiatric symptoms. Future research is warranted to include these measurements (i.e., psychotic disorder, eating disorder, antisocial personality disorder, sexual histories) to better understand the features of the LC1, high risk for suicide without distress subgroup.
Regarding the characteristics of adolescents in high risk for suicide without distress, post-hoc analyses showed high levels of impulsivity, self-harm, and deviant behaviour problems, along with childhood maltreatment experiences. Additionally, the scores of deviant behaviour problems and self-harm were mid-range for high risk for suicide with distress and low risk for suicide with distress. These results are consistent with those of prior studies indicating that deviant behaviour problems [20] and self-harm [24] are proximal risk factors of adolescents’ suicidality. Given that impulsivity was high in high risk for suicide without distress, an intervention aimed at decreasing impulsivity and problematic behaviours might be helpful to prevent suicidality in this subgroup.
High risk for suicide with distress (3.4%, 60/2,258) was the other high-risk suicidality subgroup, with the highest probability of depression, anxiety, and suicidal ideation, and a moderate probability of planned and attempted suicide. This subgroup is quite similar to the fourth latent class in the study by Jiang et al. [30] In their study, female gender, forced sexual intercourse, and smoking were the main features of that latent class. However, the gender effect was not significant within high risk for suicide with distress in the current study. In post-hoc analyses, adolescents in this class reported significantly higher scores on impulsivity, self-harming behaviours, deviant behaviour problems, and childhood maltreatment, and lower scores on self-esteem, relative to those in other classes. These results are consistent with the previous findings that childhood physical and sexual abuse [49], substance use including smoking and alcohol [22,29], impulsivity [16,17,50], self-harming behaviours [24,25], and low self-esteem [18] are significantly associated with suicidal thoughts and attempts. These findings indicate that a high risk for suicide with distress, which is characterized by both emotional distress and suicidality, should be treated with the highest priority in suicide prevention and interventions. This subgroup might benefit from risk management, such as the distress safety plan interventions suggested by Bagge et al. [51,52] A distress safety plan targets those at risk of suicidal thoughts and those who planned and attempted suicide, along with individuals suffering from emotional distress. Additionally, dialectical behavior therapy, aimed at reducing impulsivity and self-harming behaviors, might be a helpful therapeutic intervention for this subgroup see for a review [53].
Several limitations to this study require consideration. Firstly, as the nature of the data was cross-sectional, casual relationships between suicidal indicators could not be inferred. Longitudinal or experimental designs in future studies are warranted to overcome this limitation of the current study. Secondly, self-report measures raise concerns regarding reliability. There is a possibility that adolescents in the present study may over- or under-report their suffering. Interview methods should be used in future research. Thirdly, because the participants in the present study were adolescents in Korea, the sample may not reflect the full aspects of the general population, and thus researchers should interpret the results with caution and not overgeneralize the findings, especially when the small latent classes are of interest. For instance, a researcher may want to investigate the small latent classes whether high risk for suicide without distress, is also identified as one of the latent classes in Western countries.
As Western cultures are known to be more open regarding the expression of thoughts and emotion than are East-Asia countries, if undetected in Western countries, LC1 might be specific to East-Asia adolescents’ suicidality. Future research is warranted to answer questions raised by the present study. The YRBS is a dichotomous measure that engenders several disadvantages in dealing with the results such as loss of information about individual differences, loss of effect size and power, or the risk of overlooking nonlinear effects [54]. Therefore, future studies should include multi-item measurements to avoid the problems mentioned above when dichotomous measurements are used. Age definitions for adolescents or youth, defined as between adulthoods and childhood, vary from law to law and country to country. According to “Basic Youth Act” adolescents are between the ages of 9 to 24 years. The UN considers youth or adolescents as those aged 15 to 24 years. Therefore, the YRBS might not correctly reflect the deviant behaviours of some participants in the present study. Finally, the present study used an abbreviated version of the questionnaire because of time pressure to complete the survey in the school, which raises concerns about the reliability and validity of the measurement itself. Indeed, the internal consistency of the self-harm inventory measured by Cronbach’s alpha was modest (0.40). The reasons for such low alpha coefficients are as follows: 1) there are only a small number of indicators per scale; 2) the scale contains substantially more zeros than the specified distribution such as normal distribution; and 3) the fact that items were chosen to represent the conceptual breadth within a complete construct. Future research is warranted to develop a reliable and validated short version questionnaire packet to be completed within a short time when conducting a large-scale mental health survey [55,56].
Despite these limitations, the present study is the first to identify the latent classes of adolescents’ suicidal behaviours, such as suicidal thoughts and planned and attempted suicide, along with emotional distress, i.e., depression and anxiety, using a person-centered approach. As the suicidal indicators used in the present study do not operate in isolation and given the complex and multifaceted nature of the factors of suicidality, the findings of the present study contribute to a better understanding of each specific risk subgroup and can help to develop interventions tailored to individuals. Future research matching the characteristics of the high risk for suicide without distress and high risk for suicide with distress in the present study to the psychiatric heterogeneity of suicide attempters observed by Ginley and Bagge [29] may offer useful and rich information for high-risk groups in a crisis. Finally, using LCA, an individual-centered approach, it is possible to identify a high-risk individual who belongs to a specific subgroup and to offer individualized intervention. Thus, researchers and clinicians need to develop a more flexible intervention program in which each module can be separated and integrated as needed. In addition, with early detection research on adolescent suicide, it is necessary to seek an efficient strategy to promote adolescents’ help-seeking behavior; digital phenotyping research and intervention might be a good way to approach adolescents with suicidality.
Notes
Availability of Data and Material
The datasets and Mplus codes used for this study are available upon request.
Conflicts of Interest
The authors have no potential conflicts of interest to disclose.
Author Contributions
Conceptualization: Jong-Sun Lee, Hoin Kwon, Hyun Ju Hong, Yong-Sil Kweon. Data curation: Hoin Kwon, Hyun Ju Hong, Yong-Sil Kweon. Formal statistical analysis: Jong-Sun Lee, Jungkyu Park. Funding acquisition: Yong-Sil Kweon. Investigation: Hoin Kwon, Yong-Sil Kweon. Methodology: Jong-Sun Lee, Hoin Kwon, Jungkyu Park, Hyun Ju Hong, Yong-Sil Kweon. Project administration: Hoin Kwon, Yong-Sil Kweon. Visualization: Jong-Sun Lee, Jungkyu Park. Writing—original draft: Jong-Sun Lee. Writing—review & editing: all authors.
Funding Statement
This work was supported by the Ministry of Education of the Republic of Korea and the National Research Foundation of Korea (NRF-2018S1A5B8A02081988).