Influence of Optimism, Social Support, and Spirituality on COVID-19 Stress in Christian Church Community
Article information

Abstract
Objective
Optimism, social support, and spirituality can be important factors related to coronavirus disease-2019 (COVID-19) stress. However, studies investigating the influence and interplay of optimism, social support, and spirituality on COVID-19 simultaneously are still few. This study is aimed to explore the influence of optimism, social support, and spirituality on COVID-19 stress in the Christian church community.
Methods
A total 350 participants were included in this study. This study was cross-sectionally conducted by using an online survey on optimism, social support, spirituality, and COVID-19 stress that were measured by the Life Orientation Test-Revised (LOT-R), Multidimensional Scale of Perceived Social Support Scale (MSPSS), Spiritual Well-Being Scale (SWBS), and COVID-19 Stress Scale for Korean People (CSSK). The prediction models for COVID-19 stress were analyzed by using univariate and multiple linear regression.
Results
Based on the results of univariate linear regression, subjective feelings on income (p<0.001) and health status (p<0.001), LOTR (p<0.001), MSPSS (p=0.025), and SWBS (p<0.001) scores were significantly associated with COVID-19 stress. The multiple linear regression model with subjective feelings on income and health status and SWSB score was significant (p<0.001) and explained 17.7% of the variance (R2=0.177).
Conclusion
This study showed that subjective feeling on low income, those who had poor health status, lower optimism, lower perceived social support, and lower spirituality were significantly affected with COVID-19 stress. Especially, the model with subjective feelings on income and health status, and spirituality showed highly significant effects, despite the interaction with associated factors. To cope with unpredictable stressful situations like the COVID-19 pandemic, integrated interventions on psycho-socio-spiritual aspect are warranted.
INTRODUCTION
The coronavirus disease-2019 (COVID-19) pandemic situation tremendously changed human daily life around the world. The negative impact of the COVID-19 infection on health lead to fearful worry [1]. Furthermore, the quarantine and social distancing for prevention of the COVID-19 spreading provoked psychosocial distress [1]. A systematic review and meta-analysis reported that student populations showed a high prevalence of depressive, anxiety symptoms as well as stress and fear symptoms during the COVID-19 pandemic stressful situation [2]. Longitudinal cohort studies also showed an overall aggravation in mental health symptoms during COVID-19 pandemic period compared to the pre-pandemic outbreak [3]. Meanwhile, after the pandemic crisis was alleviated, these symptoms of mental health were recovered to prepandemic levels [3].
To manage COVID-19 stress for prevention of mental problems and illness, it will be important to explore factors associated with COVID-19 stress. Optimism can be a protective factor to be closely considered as an associated factor with COVID-19 stress in the pandemic situation [4-6]. A study of university students during the COVID-19 pandemic situation reported that optimism had a positive effect on the regulation of stress, anxiety, and depression [7]. Social support was also known as one of the protective factors on mental health. A meta-analysis study confirmed the positive effect of social support on mental health [8]. The positive effect of social support was similarly observed not only in the general population, but also in special groups of people such as pregnant women, adolescents, or immigrants [9-11]. Considering these positive effects of social support, even in the COVID-19 pandemic situation, social support can act as a protective factor for mental health [12,13]. Furthermore, spirituality can positively affect COVID-19 stress and mental health [14,15]. Spirituality has been reported as a factor inducing positive changes on mental health in people on special circumstance, such as pregnant women and immigrants, and in patients with severe disease, such as Crohn’s disease, cancer, and autism [6,16-19]. A study conducted in Malaysia found that spirituality reduced fear and helped maintain mental health during COVID-19 pandemic situation [20]. In addition, a study in Italy reported that spirituality was a protective factor in the onset of mental illness, and religious activity had a beneficial effect on mental health [21].
As noted previously, optimism, social support, and spirituality can be important factors related to COVID-19 stress. Although there would be more associated factors with COVID-19 stress, these factors could be represented in terms of psychological, social, and spiritual aspects, respectively. However, studies investigating the influence and interplay of optimism, social support, and spirituality on COVID-19 simultaneously are still few, especially, those that would examine the effect of spirituality. Research into religious groups seeking spirituality need to be performed. Thus, this study aimed to explore the influence of optimism, social support, and spirituality on COVID-19 stress in Christian church community.
METHODS
Subjects
The participants of this study were recruited through an online survey was conducted using Google Forms from July 30, 2021 to August 23, 2021. Inclusion criteria were defined as 1) more than age 18, 2) people attending Christian church, and 3) people who consent to the online survey for research. The people who wanted to participate in this study and have difficulties in adequate response to online survey due to things such as illiteracy and intelligence problems were excluded. Considering the gender ratio of attendees in Korean Christian churches, the participants in this study maintained 1:2.5 (male:female) gender ratio. After recruiting 100 male and 250 female subjects, an online survey was closed. A total 350 male and female subjects were finally included in this study. This study was approved by Institutional Review Board at Pusan National University Hospital (PNUH IRB: No. 2206-017-116).
Design
This study was cross-sectionally conducted by using the results of a questionnaire survey on optimism, social support, and spirituality. Demographic variables such as age, gender, marital status, education level, and subjective feelings on income and health status were investigated. Subjective feeling on income was measured by the 5-point Likert scale such as very low (1), low (2), middle (3), high (4), and very high (5). Subjective feeling on health status was measured by the 5-point Likert scale such as very bad (1), bad (2), middle (3), good (4), and very good (5). Optimism was evaluated through the Life Orientation Test-Revised (LOT-R), and social support was evaluated through the Multidimensional Scale of Perceived Social Support Scale (MSPSS). Spirituality was evaluated using the Spiritual Well-Being Scale (SWBS). COVID-19 stress was evaluated by the COVID-19 Stress Scale for Korean People (CSSK).
Measurements
LOT-R
To measure optimism, the LOT-R was used in this study [22]. The LOT-R consisted of 10 items, consisting of 3 generalized positive expectations, 3 negative expectations, and 4 ambiguous questions. Ambiguous questions were inserted to prevent the examination’s intention from being understood. Negative expectation items were reversely scored, and ambiguous items were excluded from scoring. Each item was rated on a 5-point scale (1=not at all, 5=very much), and a higher score indicated higher optimism. The Korean version used in this study showed acceptable reliability with Cronbach’s alpha 0.75 in the previous study [23].
MSPSS
The MSPSS was a self-report questionnaire that measures social support functions developed by Zimet et al. [24]. The MSPSS was a 5-point Likert scale composed of 12 items [24]. The possible score range was between 12 and 84. A higher score reflected higher perceived social support. Three factor models on family, friends, and significant others demonstrated good psychometric properties in previous studies [24-26]. The Korean version used in this study also showed good internal consistency with Cronbach’s alpha 0.89 [27].
SWBS
The SWBS was developed by Paloutzian and Ellison [28]. This scale consisted of a total of 20 items with two factors such as religious well-being and existential well-being. Each item was rated on a 6-point scale (1=not at all, 6=strongly agree), and a higher score indicated a higher level of spiritual well-being. The Korean version in this study showed good reliability (Cronbach’s alpha: total scale 0.91; religious well-being 0.90; existential well-being 0.87) [29].
CSSK
To measure COVID-19 stress, the CSSK developed by Kim et al. [30] was developed. This scale has a total of 21 items and consists of three factors: fear of infection, difficulty due to social distancing, and anger towards others. Each question was rated on a 5-point scale (1=not at all, 5=very much), and a higher score meant more stress from COVID-19. Examples of questions are “I am anxious because I do not know when and where I will be infected with coronavirus,” “It is difficult because I cannot meet my family and friends often because of coronavirus,” etc. This scale showed good internal consistency (Cronbach’s alpha: total scale 0.91; fear of infection 0.93; difficulty of social distancing 0.81; anger toward others 0.89) and good construct validity [30].
Statistical analysis
Socio-demographic and clinical variables were expressed as mean±standard deviation or number (%) according to characteristics of variables. To explore influences of associated factors on COVID-19 stress, univariate linear regression was performed on each variable. Subjective feelings on income and health status were used as a dependent variable in univariate linear regression. To analyze the impact and interplay with significant factors simultaneously, multiple linear regression analysis was performed by using backward elimination (p<0.10 for retention, p<0.05 for significance). Multicollinearity was evaluated by variance inflation factor (VIF) and tolerance. Statistical significance was defined as p<0.05. A statistical analysis was performed using the SPSS 22.0 statistical program (IBM Corp., Armonk, NY, USA).
RESULTS
Socio-demographic characteristics
Socio-demographic characteristics were shown in Table 1. The mean age of participants was a 46.2±11.8 years, ranged from 20 to 75. The marital status of the participants was 67.7% married, divorced/separated 30.9%, and unmarried 1.4%. The mean education year was 16.0±2.1. As for the subjective feeling on income, the case responding as middle was mostly 49.4%, and the case of responding as low or very low was 34.0%. The subjective feeling on health status of the participants was examined that 49.1% of the respondents answered as middle, and 14.5% answered as bad or very bad.
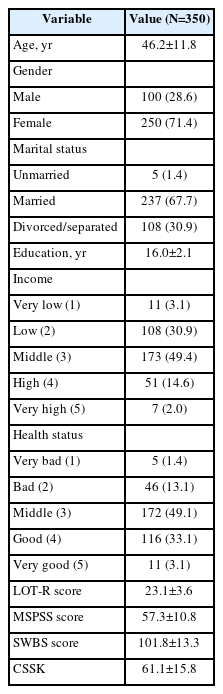
Socio-demographic characteristics
Results of univariate linear regression
Based on the results of univariate linear regression in Table 2, the age, education, and gender were not significantly associated with COVID-19 stress. Subjective feelings on income and health status were significantly associated with COVID-19 stress (income: B=-4.136, p<0.001; health status: B=-4.175, p<0.001). Optimism measured by LOT-R was significantly associated with COVID-19 stress (B=-1.193, p<0.001). Perceived social support measured by MSPSS was also significantly associated with COVID-19 stress (B=-0.175, p=0.025). Furthermore, spirituality measured by SWBS was significantly associated with COVID-19 stress (B=-0.451, p<0.001).
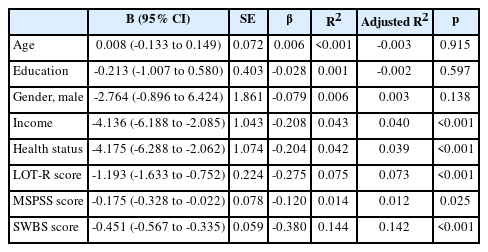
Associated factors with COVID-19 stress based on univariate linear regression
Results of multiple linear regression
As shown in Table 3, multiple linear regression analysis with backward elimination were performed. The Model 1 was composed of associated factors with COVID-19 in univariate linear regression. In Model 1, the LOT-R score was removed because the p-value was biggest 0.538. The Model 2 included the variables except the LOT-R score. In the Model 2, the MSPSS score was removed because the p-value was more than 0.10 as 0.144. Finally, the Model 3 with subjective feelings on income and health status and SWBS, showed a score that was significant (p<0.001). The final Model 3 explained 17.7% of the variance (R2=0.177). The VIFs and tolerances in linear regression models ranged from 1.043 to 1.850 and from 0.540 to 0.958, respectively. Based on the VIFs and tolerance, multicollinearity was within an acceptable range in linear regression models.

Regression model associated with COVID-19 stress using multiple linear regression with backward elimination
DISCUSSION
This study investigated the factors associated with COVID-19 stress. Low income and poor health status, lower optimism, lower perceived social support, and lower spirituality were significantly related to COVID-19 stress. The COVID-19 pandemic situation unexpectedly led to an economic crisis due to the shrinkage of usual consumption. Personal economic condition that are usually not good would have inevitably intensified COVID-19 stress. Individual health status was likely to be related to COVID-19 stress. People with chronic conditions can be negatively influenced by COVID-19 infections [31,32]. When personal medical condition was not good, the stress and fear about the risk of being infected by COVID-19 would be much greater. Optimism was also an important protective factor for COVID-19 stress [7]. Concerns about vague and unpredictable situations, such as the possibility of infection or complications from vaccine side effects or treatment complications, can exacerbate COVID-19 stress. Optimism can be the strength to endure these uncertain situations [4,7]. In addition, social support can be the strength to endure isolated stressful situations [12,33]. Although social distancing was mandatory to prevent the spread of infection during the COVID-19 pandemic, a quarantine system that does not undermine the social support system would be better in aspects of mental health management. Considering that stress can disturb the immune system and reduce resistance to virus, policies to maintain good mental health are required to form herd immunity well.
Interestingly, spirituality was identified as a strong protective factor in this study. Multiple linear regression models suggest that spirituality appears to be a strong factor associated with COVID-19, pertaining to stress in a global pandemic situation when compared with interactions of optimism and social support [20,21]. Although optimism and social support are known to be a strength in overcoming adversity [7,12,33], spirituality is likely to be a more empowering factor in unpredictable and uncertain situations, like a COVID-19 pandemic. Spirituality has been seen to bring positive outcomes in extremely stressful situations such as life-threatening cancer or hospice care [34,35]. The tremendous fear which prevailed at the beginning of the COVID-19 outbreak, could bring more significant consequences than a typical, stressful situation. More intense, stressful situations may require a spiritual approach that goes beyond optimism and social support.
Considering that COVID-19 stress worsens mental health [2,36], it is necessary to modify associated factors with the COVID-19 stress. Optimism is one of the modifiable factors. Psychological interventions to increase individual happiness and optimism have been performed in various ways [37]. Meta-analyses showed that positive psychological interventions for enhancement of optimism could be effective on depressive symptoms as well as psychological well-being [38,39]. Meanwhile, spirituality programs for empowering person have been tried in several populations exposed to stressful situations [40,41]. Especially, spirituality programs were significantly effective in persons under severe stressful situations such as terminally ill patients in hospice [42] and severe psychiatric patients [43]. To efficiently overcome COVID-19 stress from economic hardship and health threatening situations, where there is the unknown of when and how it will go, the ability to view life from a spiritual level can be beneficial. For this reason, spirituality should be considered a key modifiable issue to pay attention to in improving mental health. Furthermore, it is necessary to develop an integrated intervention model that includes spiritual enhancement programs on existing psychosocial intervention for prevention of mental problems during severe stressful situations like COVID-19 pandemic.
There are some limitations. Firstly, this study was a cross-sectional study conducted in the context of the COVID-19 pandemic. Thus, a causal relationship between COVID-19 stress and associated factors cannot be confirmed. In the future, it is necessary to investigate the factors associated with the change of COVID-19 stress through cohort study. Secondly, this study was performed by using a self-report questionnaire. It needs to be investigated with rater-based assessments. However, this study can be meaningful in that it simultaneously explored factors associated with COVID-19 stress in psychological, social, and spiritual aspects. Thirdly, since the findings in this study were only investigated by interviewing those of the Christian faith, there are limitations in generalizing these results to those who represent other religions. Future studies need to be conducted to see if similar findings would be observed in people representing other religions. Fourthly, since the stress of COVID-19 and its associated factors can be differential according to age, the generalization of these findings to adolescent or elderly people was limited. In the future, COVID-19 stress, and its associated factors, needs to be explored in the adolescent and elderly population.
In conclusion, the COVID-19 pandemic situation has tremendously changed the lives of all of us and provoked several COVID-19 related stresses. Even if the COVID-19 pandemic were to end, there may be a similar global stressful situation in the future. To cope with unpredictable stressful situations like COVID-19 pandemic, psychosocial interventions to strengthen protective factors and reduce aggravating factors related to stressful situation are warranted. This study showed that psycho-socio-spiritual factors, especially spirituality, were related to COVID-19 stress. Proper interventions on psychosocio-spiritual aspects can be useful in coping with future stressful situations like COVID-19 pandemic. The spiritual aspect should not be overlooked, especially, when coping with a stressful situation such as a pandemic.
Notes
Availability of Data and Material
The datasets generated or analyzed during the study are available from the corresponding author on reasonable request.
Conflicts of Interest
The authors have no potential conflicts of interest to disclose.
Author Contributions
Conceptualization: Kyoungmi Kim, Sung Il Moon. Data curation: Kyoungmi Kim, Sung Il Moon. Formal analysis: Hyun Ju Lim, Eunsoo Moon. Investigation: Kyoungmi Kim, Sung Il Moon. Methodology: all authors. Project administration: Sung Il Moon. Resources: Kyoungmi Kim, Sung Il Moon. Software: Hyun Ju Lim, Eunsoo Moon. Supervision: Sung Il Moon. Validation: Kyoungmi Kim, Eunsoo Moon, Sung Il Moon. Visualization: Eunsoo Moon. Writing—original draft: Kyoungmi Kim, Hyun Ju Lim, Eunsoo Moon. Writing—review & editing: Eunsoo Moon, Sung Il Moon.
Funding Statement
None