Attachment Insecurity and Stigma as Predictors of Depression and Anxiety in People Living With HIV
Article information

Abstract
Objective
The purpose of this study was to examine whether attachment insecurity, stigma, and certain demographic and medical factors predict depression and anxiety in people living with HIV (PLWH).
Methods
Participants were 147 PLWH who visited the outpatient infection clinic in Kyungpook National University Hospital (KNUH; Daegu, South Korea) between June 2020 and January 2021. We measured HIV-related stigma, attachment anxiety and avoidance, depressive symptoms, and anxiety symptoms.
Results
Logistic regression analysis showed that unemployment, longer time receiving antiretroviral therapy, higher attachment avoidance, and higher attachment anxiety were significant predictors of depression. Results also showed that longer time receiving antiretroviral therapy, higher attachment anxiety, and concern with public attitudes were significant predictors of anxiety.
Conclusion
In addition to education to reduce public stigma, interventions to reduce PLWH’s self-stigma should continue. We suggest attachment-based psychotherapy as an effective intervention to improve PLWH’s mental health.
INTRODUCTION
The introduction of combination antiretroviral therapy (ART) has changed the concept of HIV infection from a life-threatening terminal disease to a controllable chronic disease [1]. There has been a considerable amount of research estimating the life expectancy of people living with HIV (PLWH) is approaching that of the general population [2-4]. With prolonged life expectancies, many recent studies have focused on the various mental health aspects of PLWH.
The projections of mortality and burden of disease to 2030 were initiated by the World Health Organization and it is estimated that along with AIDS and ischemic heart disease, unipolar depression will be one of the three diseases of most significant burden worldwide [5]. Depression is the most common neuropsychiatric complication among PLWH and have reported a two to four times higher prevalence than in general population [6]. Anxiety disorders are also prevalent among PLWH. Depression and anxiety are associated with sexual risk behaviors, nonadherence to HIV medications, progression to AIDS, higher mortality rates and low quality of life (QOL) [7-9]. These psychiatric disorders can subsequently lead to a more complicated clinical course in adapting to HIV care.
Several demographic and clinical factors are known as risk factors for depression and anxiety in people with HIV infection. A review paper that studied depression in PLWH stated that the depression prevalence was high when the infected person is female, in their 50s or older, when there is no residence, unemployment, and lower income. Increased level of HIV-RNA is also known as risk factor for depression [6]. Another study identified that sexual orientation and emergency of HIV-related symptoms as predictors of depression and anxiety in PLWH [10].
Many studies have noted that the stigma related to HIV could be a considerable barrier to HIV prevention and treatment. Some recent studies have attempted to examine the mechanisms of HIV-related stigma at an individual level. Earnshaw and colleagues [11,12] suggested the HIV Stigma Framework (HSF) for PLWH, to explore how the stigma of HIV elicits a series of stigma mechanisms and leads to deleterious outcomes including affective, behavioral, and physical health and well-being. Studies have been conducted around African, Western, and some Asian countries to reduce HIV-related stigma and have been shown to be effective in reducing stigma at an individual or social levels [13]. However, HIV-related stigma is still prevalent around the world, affecting patients’ emotional and physical well-being.
Being able to connect and rely emotionally on others helps prevent and reduce mental and medical problems in many diseases. In this context, attachment security is becoming more important in medical settings. Several studies have shown that attachment security in patients with chronic diseases such as diabetes, systemic lupus erythematosus, and cancer affects patients’ QOL, disease management, and disease adaptation [14-16].
According to attachment theory, based on previous support experiences with other people affected the development of internal working models of close relationships. These models can affect an individual’s perceptions of others’ availability in a stressful situation and how to handle stressors [17,18]. Although early life relationship models have an impact on life as a whole, they are likely to evolve as individuals develop new relationships or experiences [19]. Close relationships can increase emotional control, which can also reduce attachment insecurity, such as attachment anxiety, by reducing negative emotions [20]. It can also be assumed that negative relationships or experiences are likely to increase attachment insecurity. A review of post-traumatic stress disorder found that patients treated after HIV diagnosis had more prevalent trauma symptoms than other chronic diseases, similar to those treated in intensive care units [21]. Previous studies have shown that the degree of trauma symptoms is closely related to attachment security [22]. The frequency of trauma symptoms in PLWH may be attributed to frequent exposure to traumatic life events before they were diagnosed with HIV, or to experiences resulting from the HIV diagnosis itself. In any case, a series of traumatic experiences or relationships may have affected the attachment security of individuals who were diagnosed with HIV and may have affected changes in the attachment system. Therefore, it can be assumed that PLWH have differences in attachment security compared to the general population or other chronic diseases [23].
Few studies have focused on the link between attachment security and emotional or psychical well-being among PLWH. In previous studies, researchers have shown that individuals coping with HIV were significantly associated with less secure and more anxious attachment styles. A study with the degree of adjustment of PLWH also suggested that secure attachment is highly related to experiencing positive disease adaptation [24,25]. There was another suggestion that attachment insecurity, especially attachment anxiety can act as a buffer between perceived and internalized stigma and can indirectly change mental health and behavior of PLWH [26]. Through these studies, it can be assumed that not only stigma but also patients’ attachment security would be a factor affecting PLWH’s physical and mental health.
Although some of the studies have noted the correlation of attachment security and HIV-related stigma that affects the mental health of PLWH, there is still a lack of research in this area. For this reason, our study has focused on HIV-related stigma and attachment insecurity as psychosocial factors that can affect depression and anxiety in PLWH. This study was conducted to determine whether HIV-related stigma, attachment insecurity, and other demographic and clinical factors of PLWH serve as factors for predicting depression and anxiety.
METHODS
Participants
Participants were 147 PLWH who visited the outpatient infection clinic in Kyungpook National University Hospital (KNUH; Daegu, South Korea) between June 2020 and January 2021. Patients were eligible to participate if they met the following criteria: 1) had been diagnosed with HIV infection, 2) were currently on an ART regimen, 3) were age 20 years or older, 4) were able to give written informed consent, and 5) were able to read and write in Korean. All participants provided written informed consent (in Korean) after we had explained the study. This study was approved by the Institutional Review Board of Kyungpook National University Hospital (KNUH IRB file no. 2020-03-034).
Sociodemographic and clinical data
Participants reported their demographic information, HIV transmission route, experience with AIDS-related diseases, ART start date, and ART adherence. To measure ART adherence, participants answered the question “How often have you missed your medication in the last four weeks?” We dichotomized responses as “very good” if the answer was “not more than once” and “not very good” if the answer was “more than once.” We extracted clinical data from the patients’ medical records, including total CD4 T-cell counts (cell/μL) and HIV quantitative real time polymerase chain reaction (RT PCR) (copies/mL).
Measures
HIV-related stigma
We used the revised HIV Stigma Scale (HSS-R) [27,28] in this study to measure HIV-related stigma. The HSS-R is an abbreviated version (32 items) of the original 40-item scale and contains four subscales. Enacted stigma is related to the personal experience of rejection. Disclosure concerns are HIV-positive individuals’ need to keep their HIV diagnosis concealed. Negative self-image provides information about PLWH’s feelings of inferiority and shame. Concern with public attitudes addresses what PLWH believe that other individuals might think about them. Participants rated items for each subscale using a 4-point Likert scale ranging from 1 (“strongly agree”) to 4 (“strongly disagree”). The Cronbach’s alpha for the 32-item Korean version of the HSS-R were measured based on the data collected under the present study, and it was 0.897 for the total scale, indicating good internal consistency. All subscales demonstrated similarly strong internal consistency (enacted stigma: 0.933; disclosure concerns: 0.785; negative self-image: 0.822; concerns with public attitudes: 0.834). However, as 57 of the 147 participants (38.8%) in our study had no experience informing other individuals about their HIV/AIDS status, enacted stigma was difficult to measure.
Attachment insecurity
We used the Modified Experiences in Close Relationships Scale (ECR-M16) to measure participants’ experiences in close romantic and nonromantic relationships across two domains: attachment anxiety and attachment avoidance [29,30]. This is a shortened version of the ECR-M36, and existing research has found the ECR-M36 to be a useful tool for understanding attachments to close family, friends, and medical staff during the course of serious illness [31,32]. The ECR-M16 contains 16 items scored on a 7-point Likert scale ranging from 1 (“disagree”) to 7 (“agree”), with total scores ranging from 8 to 56 on each subscale. High scores on each subscale indicate high attachment insecurity. The full scale’s Cronbach’s alpha of 0.816 demonstrated the Korean version of the ECR-M16’s good internal consistency based on the data collected in this study. The eight-item attachment anxiety subscale also demonstrated good internal consistency (Cronbach’s alpha=0.880), and the eight-item attachment avoidance subscale’s internal consistency was acceptable (Cronbach’s alpha=0.649).
Depression
We measured depressive symptoms using the Korean version of the Patient Health Questionnaire-9 (PHQ-9) [33]. The PHQ-9 assesses nine criteria on which the DSM-IV diagnosis of major depressive disorder is based. The nine items utilize a 4-point Likert scale from 0 (“not at all”) to 3 (“nearly every day”). Total scores range from 0 to 27. Currently, the recommended single screening cutoff score for major depressive disorder diagnosis is 10 or greater [34,35], which we also used in our study.
Anxiety
We measured anxiety symptoms using the Korean version of the Generalized Anxiety Disorder-7 (GAD-7) [36,37]. On a 4-point Likert scale ranging from 0 (“not at all”) to 3 (“nearly every day”), participants rated how often they have experienced feelings of nervousness, worry, or restlessness in the past two weeks. Total scores range from 0 to 21. In the Korean version, a score of 8 or greater represents an optimal cutoff value for identifying cases of generalized anxiety disorder, which we applied in our study to indicate the presence or absence of anxiety.
Statistical analysis
First, preliminary analyses were performed to identify significant group differences within the sample. Chi-square tests were conducted using categorical variables: gender, marriage, employment, education, monthly income, religion, HIV transmission route, experience with AIDS-related diseases, and ART adherence. Fisher’s exact test was applied when more than 20% of cells had expected frequencies lower than 5. Cutoff levels for PHQ-9 were 10 points or more, GAD-7 were 8 points or more. Also, Pearson correlation analyses were conducted for continuous variables: ART period from start, total CD4 T-cell count, HIV quantitative RT PCR, attachment anxiety, attachment avoidance, disclosure concerns, negative self-image, concern with public attitudes, PHQ-9, and GAD-7.
Second, the backward stepwise binary logistic regression analysis using log-likelihood ratio statistic was performed to determine the predictors for depression and anxiety. All the sociodemographic, medical, and psychological variables investigated in this study were included in the analysis to determine potential explanatory variables. We used SPSS version 21 for Windows (IBM Corp., Armonk, NY, USA) for all analyses.
RESULTS
Participants’ sociodemographic, clinical, and psychiatric characteristics
The mean age of participants was 42.7 (standard deviation [SD]=12.5) years, and the majority were male (n=142, 96.6%). Most participants were single (68.0%), employed (65.3%), had a monthly income of 3 million KRW or less (66.7%), had no religion (65.3%), had not experienced AIDS-related diseases (68.7%), and had very good ART adherence (89.8%). The proportion of groups that continued their education after high school and those who did not were similar. Almost half the participants reported their HIV transmission route via homosexual or bisexual behavior (45.6%). The mean ART period was 71.3 (SD=58.6) months, the mean CD4 T-cell count (cells/μL) was 610.3 (SD=428.7), and the mean HIV quantity based on RT PCR analysis (copies/mL) was 8,544.9 (SD=87,642.9) (Table 1). After the survey for demographics, researchers tried to minimize missing data thorough question and answer with the participants, but if the participant did not wish to answer the question, it was processed as missing data, some data showed that the total number did not satisfy 147.

Sociodemographic and clinical data of the study participants
The mean score on the PHQ-9 was 5.9 (SD=6.3) and on the GAD-7 was 4.4 (SD=4.8). Participants with depression (PHQ-9 score ≥10) comprised 21.8% (n=32) of the sample, and those with anxiety (GAD-7 score ≥8) accounted for 23.1% (n=34). The mean score on the ECR-M16 attachment anxiety subscale was 24.7 (SD=10.8) and on the attachment avoidance subscale was 30.3 (SD=8.2). As for the HSS-R, the mean score on the disclosure concerns subscale was 25.2 (SD=5.1). The mean negative self-image score was 17.8 (SD=4.9), and that for the concern with public attitudes subscale was 19.0 (SD=4.2) (Table 2).
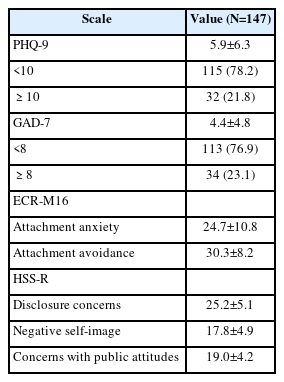
Psychiatric measures of the study participants
Comparing groups with or without depression or anxiety
The results of the chi-square test showed that the proportion of depressed participants was significantly higher in the unemployed group than in the employed group (p=0.009). The mean values for the ART period (p=0.018), GAD-7 (p<0.001), attachment anxiety (p<0.001), attachment avoidance (p<0.001), negative self-image (p=0.012), and concerns with public attitudes (p<0.001) were statistically significantly higher for depressed participants than for those without depression (Table 3).

Results of analyses comparing two groups with or without depression
Like depression, anxiety was significantly more frequent when HIV-positive individuals were unemployed (p=0.037). The mean values for the PHQ-9 (p<0.001), attachment anxiety (p<0.001), attachment avoidance (p<0.001), disclosure concerns (p=0.046), negative self-image (p<0.001), and concerns with public attitudes (p<0.001) were statistically significantly higher for anxious participants than for those without anxiety (Table 4).

Results of analyses comparing two groups with or without anxiety
Correlation analysis for continuous variables
Participants’ age was positively correlated with ART period (r=0.366) but negatively correlated with attachment anxiety (r=-0.216). Depression (r=0.240) and anxiety symptoms (r=0.173) were positively correlated with ART period. Depression was positively correlated with all measured psychosocial factors: anxiety (r=0.850), attachment avoidance (r=0.333), attachment anxiety (r=0.512), disclosure concerns (r=0.169), negative self-image (r=0.281), and concern with public attitudes (r=0.310). Anxiety also was positively correlated with attachment avoidance (r=0.326), attachment anxiety (r=0.552), disclosure concerns (r=0.182), negative self-image (r=0.299), and concern with public attitudes (r=0.317) (Table 5).
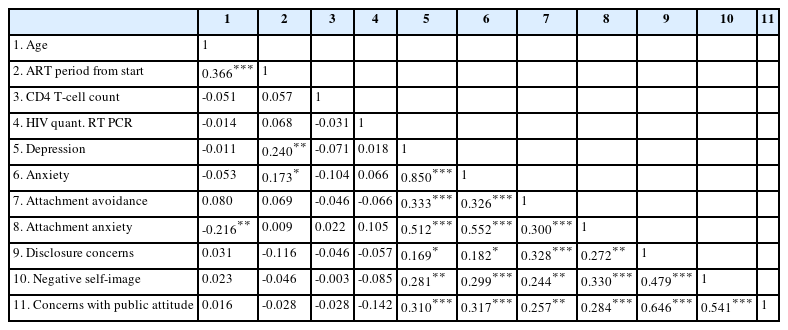
Results of Pearson correlation test for continuous variable
Logistic regression predicting depression and anxiety in PLWH
The variables shown in Tables 6 and 7 are the variables included in the equation in the last step through backward elimination. The analysis indicated that unemployment (odd ratio [OR]=3.068, p=0.048), longer ART period (OR=1.016, p=0.002), higher attachment avoidance (OR=1.076, p=0.049), and higher attachment anxiety (OR=1.130, p<0.001) were significant predictors of depression (Table 6). Further, longer ART period (OR= 1.012, p=0.005), higher attachment anxiety (OR=1.132, p< 0.001), and greater concern with public attitudes (OR=1.203, p=0.022) were significant predictors of anxiety (Table 7).
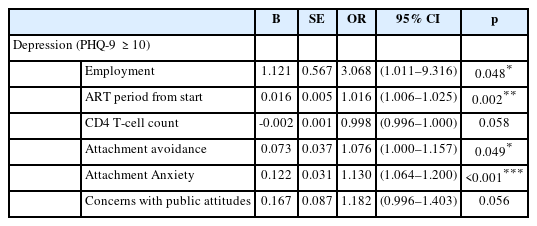
Results of logistic regression analysis for factors predicting depression (PHQ-9 ≥10)
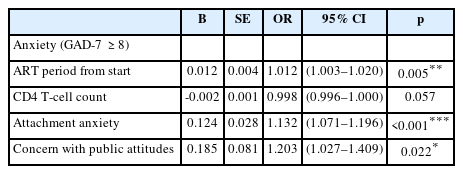
Results of logistic regression analysis for factors predicting anxiety (GAD-7 ≥8)
DISCUSSION
Sociodemographic and clinical factors associated with depression and anxiety
The gender and age distributions shown in the results were similar to the Korea HIV/AIDS cohort study which investigated the enrollment of PLWH between 2006 and 2016 [38]. And also, for depression and anxiety prevalence, results were similar to past one-month mood disorder diagnosis prevalence shown in a previous US study [39]. In the South Korean cohort study, each severe depressive and anxiety symptom was reported 17.6% and 13.2% at the baseline [38].
The chi-square test and logistic regression analysis results indicate unemployment state and ART period are significantly correlated with depression or anxiety among participants. Unemployment and job loss have been reported to be associated with impaired mental health for a long time. A meta-analysis with 237 cross-sectional and 87 longitudinal studies revealed significant differences in several indicators including distress, depression, anxiety, psychosomatic symptoms, subjective well-being, and self-esteem depending on the employment status [40]. In this context, our findings have similar results to a number of existing studies.
In most previous studies, a long period from the start of ART was not suggested as a predictor for psychological well-being. However, it has been suggested that in those with long-term HIV infection, the persistent activation of immune cells by the virus likely increases the susceptibility of these patients to inflammatory diseases [41]. This reaction can increase the likelihood of other chronic diseases associated with inflammatory reactions in PLWH, and as age increases, its effects can also affect an individual’s psychological well-being [42]. Nevertheless, more research is needed to relate it to mental health over time on ART.
HIV-related stigma as a predictor for depression and anxiety
In our study, the mean score of three subscales of HSS-R is shown to be higher than a previous study conducted in the US, and above all, concern with public attitudes revealed the largest difference in mean score compared with the previous study [27] (Table 2). The stigma associated with this subscale is related to the overall social perception of the disease. Globally, social stigma and discrimination against PLWH are still known as unresolved problems, but in Korea, such problems are found to be much more serious than in Western countries. In a survey released in 2019 by the Korea Center for Disease and Prevention, 52.4% of the 1,000 responders from the general population, said they could not eat a meal with a HIV-infected person [43]. This shows a significant difference from the results of the report for stigmatizing attitudes toward PLWH conducted in the Center for Disease Control and Prevention in the United States, that 17.5% of adults responded that they were afraid of casual contact with HIV-infected persons [44]. Prejudice against PLWH in Korea can be defined as serious in society when to compared with Western societies, it can be predicted that the stigma that patients perceive will also be high [43]. And it has been suggested that negative perceptions of disease affect not only concerns about social attitudes but also the possibility of anticipatory stigma and internalized stigma. This explains why the overall stigma of patients in our study is higher than in the previous study [45].
Internalized stigma, represented by negative self-image in our study, has been argued to have a close connection to mental health in several previous studies as well as the HSF [11,12,45]. In this study, negative self-image was not shown as a predictor in either depression or anxiety. Instead, concern with public attitudes was shown as a predictor of anxiety, which was not significant in depression, but was close to statistical significance. In the correlation study, each stigma subscale including negative self-image has shown to be associated with depression and anxiety, but concerns with public attitudes established a higher degree of correlation. These results can be attributed to the increasingly problematic social stigma in Korea compared to the West. Given its’ high association with mood symptoms, ongoing efforts are necessary to reduce the associated stigma. In South Korea, education continues at the national level to reduce the stigma of HIV and promote related knowledge. As part of such efforts, surveys conducted in 2019, showed a reduction in personal-level stigma and increased knowledge levels, but the social stigma remained problematic [43]. Efforts should continue across the country, communities, and health care institutions to reduce the overall social stigma.
Given the same degree of prediction of mental illness in stigma and attachment security, the stigma did not act as a predictor of depression. Concern with public attitudes is shown to have less statistical significance for predicting anxiety than attachment anxiety. Stigma itself can act as a factor related to depression and anxiety, but its importance as a predictor is less when placed on the same line as attachment anxiety.
Attachment insecurity as a predictor for depression and anxiety
Since the ECR-M16 measure used in our study was not used in other studies with PLWH, simple comparison of mean score was difficult. In an Australian study of attachment security of parents with young children with ECR-M16, both attachment anxiety and attachment avoidance averaged around 16 points, which is significantly lower than our study [46]. Other study with advanced cancer patients, participants showed similar degree of attachment anxiety to our study, but a much lower degree of attachment avoidance [47]. Comparing the two dimensions within the participants to each other also shows attachment avoidance (30.3±8.2) has a much higher mean score compared to attachment anxiety (24.7±10.8). This result shows contrary to several previous studies of HIV positive participants’ attachment insecurity conducted in the United States, in which participants scored slightly higher mean scores in attachment anxiety than attachment avoidance [48-50]. Although there is now a general consensus that the attachment behavioral system is applicable to all humans, there is still a growing body of research devoted to cross-cultural aspects of the attachment system [51]. In other words, cultural differences in each country can affect the attachment security in adulthood and it can change the quality of attachment during lifetime. As mentioned above, prejudice against PLWH in Korea can be serious in society when compared to Western countries, and it can also be considered that such cultural differences may have affected patients’ attachment behavior. This sociocultural influence may have strengthened the aspect of avoiding and suppressing problems rather than facing them and solving them through relationships with others.
Results from both correlation analysis and logistic regression showed a significant correlation between affective symptoms with attachment insecurity. The Pearson correlation test (Table 5) demonstrated that both attachment anxiety and attachment avoidance had a high degree of correlation with depressive and anxiety symptoms. As a result of logistic regression analysis (Tables 6 and 7), attachment anxiety is a predictor of both depression and anxiety. However, attachment avoidance was suggested to be a predictor of depression, but not anxiety. In addition, the result suggests that anxious attachments are more strongly predictive of depression than attachment avoidance, given their odds ratio and statistical significance.
In a meta-analysis published in 2020, authors examined the strength of correlations between two attachment dimensions with depressive symptoms. As a result, attachment anxiety was indicated to be more strongly related to depressive symptoms than attachment avoidance [52]. The authors explained that both attachment dimensions are related to maladaptive emotional regulations, but the different use of strategies had led to this result. Individuals with high attachment anxiety tend to adopt hyperactivating strategies such as focusing on their distress to gain support from others. They usually use emotion focused coping, and this strategy does not relieve painful emotions. However, individuals with high attachment avoidance, usually emphasize self-reliance and often use deactivating strategies like suppressing their negative emotions in stressful situations [53]. This strategy may not bring about a fundamental release of emotions, but in the short term, it may have the effect of preventing distress. In this way, the difference in the effects of two attachment dimensions on depression might be explained, and our research can also be said to have this context.
While many previous studies have shown a high link between attachment anxiety and anxiety disorders, the association with attachment avoidance and anxiety disorders has been somewhat controversial. Several studies have shown that both insecure attachment dimensions are positively associated with anxiety symptoms. However, other studies suggested that the anxious attachment, but not avoidant attachment are related with anxiety symptoms or disorders [54,55]. Individuals with anxiety disorder report that their worry-related cognitions are mostly focused on interpersonal domains. Furthermore, research suggests that anxiety disorder is associated with a tendency to excessively seek support and reassurance from others as a means of reducing anxiety-related pain. This tendency of anxiety disorder patients could be seen as similar in strategy to those with high attachment anxiety, which is somewhat different from those with high attachment avoidance. It is suggested that a more diversified additional approach is needed for the association between avoidance attachment and anxiety disorder, considering the various variables involved.
As mentioned in the discussion related to stigma, our findings differ from previous studies in that attachment insecurity, especially attachment anxiety has precedence over stigma as a predictor of depression and anxiety. As attachment insecurity has emerged as an important psychosocial factor in predicting mental illness in our study, a related therapeutic approach will be important. Previous studies have shown that psychotherapy is an effective way to alleviate depressive symptoms in PLWH [56-58]. We propose that attachment-based psychotherapy will be an excellent intervention to improve mental health among PLWH, as our findings have shown that attachment security has a significant impact on patient’s affective symptoms. Attachment-based psychotherapy is a therapy that attempts to create a secure enough base to explore insecurities around attachment and relationships [59]. Through this intervention, we can expect improvement in patients’ mood symptoms and improvement in overall physical and social psychological health.
In addition, services will be needed to make psychiatric intervention more accessible to patients. PLWH may be reluctant to visit psychiatric clinics due to their own high stigma and above-normal avoidance and anxiety attachment. Therefore, the introduction of integrated health service in which psychiatrists are included in care unit and begin interventions early in diagnosis, could be a way to effectively provide mental health service [58].
Limitations
Our study has several limitations that should be taken into consideration. First, there may have been a selections bias in including participants in the study. Participants in the study were handed over to the study coordinator after brief explanations and recommendations from the consulting nurse or physician in the survey, and patients who had not been cooperated before meeting the study coordinator were excluded from the study. This leaves open the possibility that those who did not cooperate with the survey may have been more reluctant to ask for help or that their physical or emotional conditions were poor. Second, the study was based on results from a single center, so further studies that include larger sample size and multiple centers are still warranted to validate our findings. Despite these limitations, this study is of great significance in that it is the first study in Korea to determine whether attachment insecurity and stigma are major factors predicting mental illness in PLWH.
Conclusion
Through this study, attachment insecurity was identified as an important factor and is highly correlated to depression and anxiety symptoms in PLWH. Attachment anxiety was presented as a predictor of depression and anxiety, and attachment avoidance was presented as a predictor of depression but not anxiety. The stigma was shown to be both related to depression anxiety symptoms. Concern with public attitudes was presented as a predictor of anxiety, but negative self-image and disclosure concerns did not appear to be a predictor of either depression or anxiety. In conclusion, continuing efforts to reduce stigma at a social level are needed. In addition, attachment-based psychotherapy may be a useful psychiatric intervention to promote PLWH’s mental health, and longitudinal studies evaluating these psychotherapy effects should be conducted in the future.
Notes
Availability of Data and Material
The datasets generated or analyzed during the study are available from the corresponding author on reasonable request.
Conflicts of Interest
The authors have no potential conflicts of interest to disclose.
Author Contributions
Conceptualization: all authors. Data curation: Kyungmin Kim, Seoyoung Jang, Shin-Woo Kim, Hyun-ha Chang. Methodology: Kyungmin Kim, Hyo-Deog Rim, Jungmin Woo. Formal analysis: Kyungmin Kim, Jungmin Woo. Investigation: Kyungmin Kim, Seoyoung Jang, Hyo-Deog Rim, Jungmin Woo. Writing—original draft: Kyungmin Kim. Writing—review & editing: Kyungmin Kim, Jungmin Woo.
Funding Statement
None