Association of Social Support and Postpartum Depression According to the Time After Childbirth in South Korea
Article information

Abstract
Objective
This study examined the association between social support and postpartum depression (PPD) according to the time after childbirth within 12 months in South Korea.
Methods
Data were collected from 1,481 women in Chungnam Province, South Korea from September 21 to 30, 2022. Multivariate logistic regression models were used to examine the association between social support and PPD. Subgroup analysis of the associations of support from family, friends, and significant others with PPD according to the time after childbirth was undertaken using crude and adjusted models.
Results
Of the participants, 39.91% had PPD. The prevalence of PPD was 36.05% at <3 months, 37.50% at 3≤ to <6 months, and 44.41% at 6≤ to <12 months. A 1-point increase in the social support score was associated with an increase in the adjusted odds ratio of PPD of 0.91 (95% confidence interval=0.90–0.93). Social support from family was significantly associated with PPD regardless of the time after childbirth. Support from significant others was significantly associated with PPD after 6≤ to <12 months.
Conclusion
Family support should be provided consistently to women after birth; social connections with significant others can prevent PPD.
INTRODUCTION
Postpartum depression (PPD) is the most common mental health problem among women after childbirth [1,2]. PPD is a mental disorder related to childbearing characterized by depressed mood, frequent crying, insomnia, fatigue, loss of appetite, feelings of worthlessness, and suicidal thoughts [3,4]. Women commonly experience PPD within 6 weeks following childbirth and recover within 6 months. However, it may persist for up to two years postpartum [2,5].
In Western countries, the prevalence of PPD varies from 10% to 15% [6]. Studies of PPD from China have found a prevalence of PPD was 19.8% [7]. In South Korea, the prevalence of PPD was 24.3% [8,9]; however, previous studies have found a higher prevalence of PPD. Differences in relation to the prevalence rates of pervious studies may be due to differences, in culture, reporting practices, and perceptions of mental health problems in the study population.
The prevalence of PPD differs over time after childbirth [10]. Community studies have shown that the prevalence of PPD is 27%–48% at 3–4 months postpartum, 30%–62% at 6 months, 25%–31% at 9 months, and 6%–39% at 12 months [11]. A prospective cohort study reported that the prevalence rates of PPD were 32.8%, 24.6%, and 22.4% at 2, 6, and 12 weeks postpartum, respectively [8]. The period prevalence rates of PPD were 15.1% within the first month, 11.6% in 1–3 months, 11.5% in 3–6 months, and 11.5% in 6–12 months after birth in Japan [12].
PPD risk may depend on sensitivity to hormonal fluctuations. The biological changes underlying postpartum blues may be modulated by genetic factors, childcare-related stress, lack of social support, low socioeconomic status, poor body image, and lack of employment [3,4,13,14].
Social support refers to the emotional, psychological, or physical support provided by another person. Family members, friends, neighbors, and relatives are important sources of social support for mothers during the period after childbirth [15]. Social support is effective in helping women cope with PPD [16-18].
Previous studies have investigated the relationship between PPD and social support. However, there was relatively little consideration for time after childbirth. Therefore, we investigated the prevalence of PPD in South Korean women and the association between social support and PPD according to the time after childbirth.
METHODS
Study design
Women in South Korea register for the Maternal and Child Health Service from 40 days before the scheduled date of childbirth to 30 days after the date of childbirth to obtain access to reproductive health, delivery, and parenting services. Our study population included 5,234 mothers registered for the Maternal and Child Health Service in Chungnam Province in 2022. Of these, 1,490 mothers agreed to participate in the web-based survey and completed the questionnaire (response rate: 28.5%). Informed consent was obtained from all the eligible participants. After excluding respondents with missing data, 1,481 women were included in the analysis. We conducted a web-based, cross-sectional survey between September 21 and September 30, 2022. This study was approved by the Institutional Review Board (IRB) of the College of Medicine, the Catholic University of Korea (approval number: MC22ZISI0095).
Sociodemopraphic characteristics
The sociodemographic characteristics of interest of the participants included age, education level, current employment status, and household income. We categorized age as 20–29, 30–39, or 40–49 years; education level as high school graduation or college or higher; current employment status as employed (full or part-time), employed (maternity leave), or unemployed; and monthly household income level as <3,000,000, 3,000,000–5,000,000, or ≥5,000,000 KRW.
Health-related variables
Maternal health-related factors included parity, period after birth, type of pregnancy, type of delivery, and planned pregnancy. Parity was categorized as 1 or ≥2. The time after birth was categorized as <3, 3≤ to <6, or 6≤ to <12 months. The type of pregnancy was categorized as spontaneous pregnancy or artificial insemination/test-tube. The type of delivery was categorized as vaginal delivery or cesarean section. Planned pregnancy was classified as yes or no.
General health-related factors included quality of sleep and past depressive disorder. Regarding the quality of sleep, the responses to the question “How is your current quality of sleep?” ranged from 1 (very satisfied) to 5 (very dissatisfied). We categorized the responses as high (very satisfied or satisfied), moderate (average), or low (unsatisfied or very dissatisfied). Past depressive disorder was classified based on the response (yes or no) to the question “Have you ever been diagnosed with depressive disorder by a doctor?”.
PPD
The Korean version of the Edinburgh Postnatal Depression Scale (K-EPDS) was used to evaluate depressive symptoms in women during the time after childbirth. The K-EPDS is a reliable and valid instrument that can be used for measuring PPD in the Korean population [19]. This assessment includes 10 items scored from 0–3 points (total score=0–30), with higher scores indicating more severe depression [20]. A cutoff score of ≥10 points was used to identify PPD [2].
Social support
The Multidimensional Scale of Perceived Social Support (MSPSS) was specifically designed to focus on perceived or subjective evaluation of social support adequacy from 3 particular sources: family, friends, and significant others. The inclusion of significant others is unique to the MSPSS. The support of significant others was associated with depression because the concept of a special person implies an especially close relationship. The significant others subscale is a strong supplement to the family and the friend subscales because it evaluates a different support source. Significant others were considered to be those who were considered significant by the participants, excluding family and friends in our study.
The MSPSS is a 12-item questionnaire, with each item rated on a 5-point Likert scale [2]. The subscale scores range from 4 to 20 points, and the total score ranges from 12 to 60 points. Higher scores indicate a higher level of perceived social support. The Korean version of the MSPSS is a reliable and valid tool for the assessment of perceived social support in the Korean population [21].
Statistical analysis
Descriptive analysis was performed to compare general characteristics of the participants according to PPD. Means and standard deviations (SD) were regarded as continuous variables, and frequencies and percentages were considered categorical variables [22]. The chi-square test and t-test were used for comparisons.
Multivariate logistic regression was used to identify the association between social support and PPD. The odds ratio (OR) and 95% confidence interval (95% CI) of PPD were estimated. In subgroup analyses, we investigated the relationships between social support from family, friends, and significant others and PPD according to the time postpartum. We constructed unadjusted and adjusted models of the associations between the social support subscales and PPD according to the time postpartum. The adjusted model included sociodemographic and health-related factors. A p<0.05 were considered statistically significant. The statistical analyses were done using SAS software (ver. 9.4; SAS Institute, Cary, NC, USA).
RESULTS
The study population consisted of 1,481 women, 591 (39.91%) and 890 (60.09%) of whom did and did not have PPD, respectively. The prevalence of PPD was 36.05% (n=159) within 3 months after childbirth, 37.50% (n=162) within 3≤ to <6 months after birth, and 44.41% (n=270) ≥6 months after birth. The sociodemographic and health-related characteristics of the PPD group are summarized in Table 1. The mean total social support score was 43.30 (SD=9.74) in women who had PPD and 51.23 (SD=7.98) in those who did not. The mean scores of support from family, friends, and significant others were 14.80 (SD=3.61), 13.66 (SD=4.02), and 14.84 (SD=3.52) in women who had PPD, respectively. The mean scores of support from family, friends, and significant others were 17.58 (SD=2.66), 16.16 (SD=3.62), and 17.50 (SD=2.75) in women without PPD. There were significant differences between the total and subscale scores between the women who had and did not have PPD (all p<0.001).

General characteristics of the participants
Multiple logistic regression was performed to investigate the association between social support and PPD after adjusting for age, current job, education level, household income, quality of sleep, past depressive disorder, parity, time after childbirth, type of pregnancy, type of delivery, and planned pregnancy (Table 2). A 1-point higher social support score was associated with a 9% lower likelihood of PPD (OR=0.91, 95% CI=0.90–0.93). The relationship between the time after childbirth and PPD was not significant. Women with low-quality sleep, a past depressive disorder, or unplanned pregnancy had a higher adjusted OR for PPD.
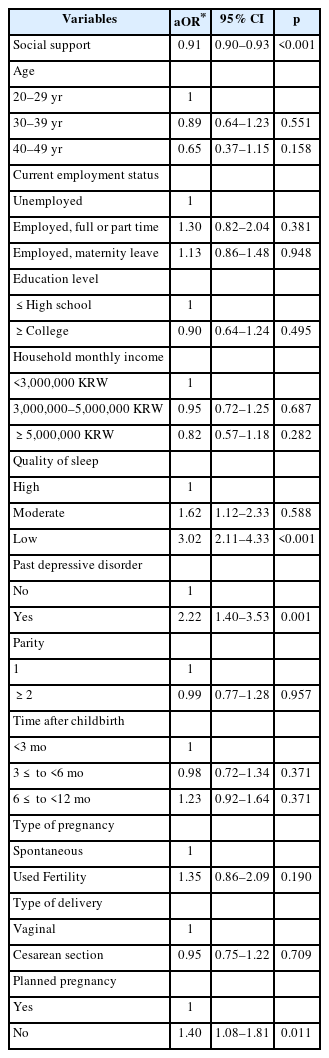
Multivariable logistic regression analysis of social support and postpartum depression
Table 3 and Figure 1 show the crude and adjusted ORs of PPD stratified by time after childbirth. Regardless of the time postpartum, total and family social support scores were negatively associated with PPD. Within 3 months after childbirth, the prevalence of PPD was 0.79 times lower with a 1-point increase in the family support score (95% CI=0.67–0.93). For women less than 6 months after birth, the prevalence of PPD was 0.80 times lower with a 1-point increase in the family support score (95% CI=0.71–0.91). After 6 months, the prevalence of PPD was 0.90 times lower with a 1-point increase in the family support score (95% CI=0.82–0.99). The support of friends was not significantly associated with PPD at any time point after birth. The support of significant others had an adjusted OR of 0.82 (95% CI=0.74–0.91) ≥6 months after birth.
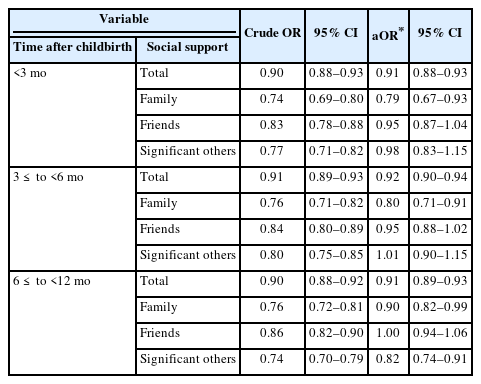
Subgroup analysis of social support and PPD according to the time after childbirth
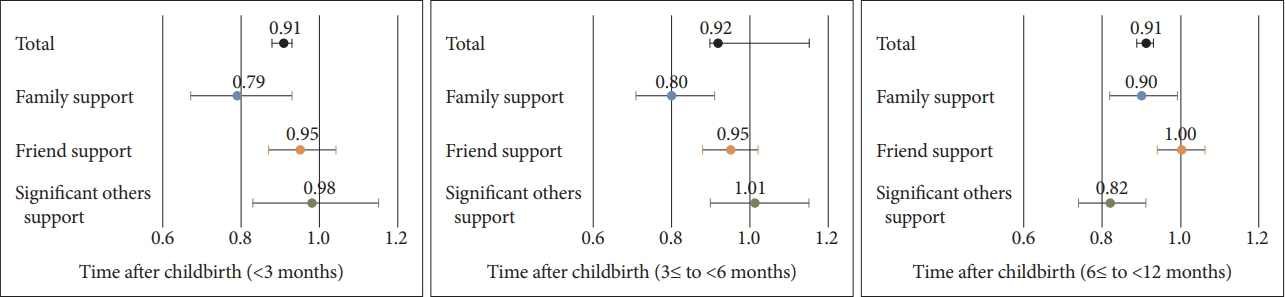
Adjusted ORs of postpartum depression according to the time after childbirth. OR, odd ratio.
DISCUSSION
This study investigated the prevalence of PPD and its association with social support up to 12 months postpartum. We found that 39.91% of the participants had PPD. The prevalence rates were 36.05%, 37.50%, and 44.41% at <3, 3≤ to <6, and 6≤ to <12 months after birth, respectively.
The self-reported prevalence of PPD varies from 1.9% to 82.1% in developing countries and from 5.2% to 74.0% in developed countries. The prevalence of PPD was 10.2% in China [23] and 14.3% in Japan. In the present study, the prevalence rates of PPD were 17.6% at 1 month, 10.0% at 2 months, and 6.1% at 3 months after childbirth in Japan [24]. A study of 122 mothers from Guangzhou, China demonstrated that the PPD rates were 23.0% at 6 weeks, 25.4% at 3 months, and 27.0% at 6 months after childbirth [25].
The prevalence of PPD was significantly higher in the present study, focused on Korea, than in other Asian countries [26]. This could be due to the use of different assessment tools to measure mental health status and the inclusion of study participants with different time intervals after childbirth. Additionally, the wide range of the prevalence may be related to different in the cutoff scores of PPD, cultural factors, or perception of mental health and its stigma [27]. The differences in the time period for PPD measurement, screening tools, and cutoff scores used to classify PPD make it difficult to compare the prevalence rates among previous studies.
Few studies have assessed depressive symptoms in women after the early postpartum period. Our study showed that PPD prevalence increased over time. As the mother’s external activities gradually increase after 6 months [28], stress may also increase, partly due to multiple, conflicting roles and responsibilities.
Previous studies have been revealed mixed results, with some showing a gradual decrease in incidence of depression during the first and second years following childbirth [8,29,30] and others showing no significant change in depressive levels after the early postpartum period [12,31]. Although higher levels of depressive symptoms decreased during the first year postpartum, minor depression symptoms increased. However, many questions regarding the course of persistent PPD, and the factors associated with persistence or remission, remain unclear. Our findings suggest that women should be evaluated for PPD beyond the early postpartum period and throughout the first year after childbirth.
Our study found that the prevalence of PPD was inversely related to the social support score; greater social support was related to higher parental self-efficacy and less severe depressive symptoms. This finding is in line with previous studies showed that perceived social support is important for coping with the effects of PPD. This is important because some women do not have access to a social network that could provide informational and instrumental support, to access psychosocial care services [32]. A study from the United Kingdom found that three brief home-based visits based on counseling techniques accelerated recovery for women with PPD [33]. Support group attendance provides mothers with a sense of hope through the realization that they are not alone. It is important to integrate mental health screening into routine primary care for pregnant and postpartum women and to follow up this screening with treatment or referral and with follow-up care [34].
Our study found that family support was important regardless of the postpartum time. Family members can help prevent the onset of mental health problems in mothers [35]. A study stated that husbands are a key source of support, and can be more helpful if they are aware of PPD and steps that can assist in recovery [36]. Women who have access to social support may feel that their family and friends are unable to be supportive due to a lack of understanding with regard to PPD, which could worsen maternal mental health or act as a barrier to treatment [32]. Family support was important during the coronavirus disease-2019 (COVID-19) pandemic because mothers spent more time at home during the COVID-19 [37].
Our study showed that mothers with higher education levels and household income were less likely to have PPD. However, the difference was statistically significant. Epidemiological evidence regarding associations of employment, income, and education with the risk of PPD is inconsistent [38]. Some studies have suggested that a low social economic status (SES) contributes to the development of PPD and that a higher SES protectes against PPD, while others report that a low SES has very little influence on the development of PPD. There were no relationships between household income or maternal educational levels with PPD in Japan [38].
We also found that a past depressive disorder, unwanted pregnancy, and low-quality sleep were related to PPD, in line with previous studies. Most mothers with PPD experience stressful events such as unplanned pregnancies [39,40]. According to one study, a past depressive disorder is a strong risk factor for PPD. Moreover, in women suffering from PPD and members of their family, there is a very strong relationship between a history of depressive or psychiatric disorder and PPD [41]. Moreover, women who did not plan their pregnancy may be unprepared and thus might implement prenatal care at a later stage [42]. Therefore, clinicians need to identify risk factors for PPD in women and implement appropriate preventive measures. Counseling services and family planning may decrease the rate of unplanned pregnancies.
This study had several limitations. First, it was a community web-based survey conducted in South Korea, which limits its generalizability. Second, it was a cross-sectional study, therefore, a causal relationship could not be established with respect to the association between social support and PPD. Third, the study used self-report measures of general and maternal health status, among other variables. However, we measured PPD using valid and reliable scales. Fourth, our findings may be subject to selection bias because participation in the study was voluntary.
In conclusion, we observed a high prevalence of PPD among women in South Korea at various time points postpartum (<3, 3≤ to <6, and 6≤ to <12 months). PPD was common and affected more than one-third of mothers, with an increase in the proportion over the months postpartum. Our data provide important insights that could aid the identification of at-risk mothers; the data also emphasize the need for long-term follow-up. The study findings indicate that family support should be provided to women after birth, and that social connections with significant others can help decrease depressive symptoms after childbirth. Therefore, support from family and significant others is crucial to reduce the risk of PPD and improve mental health.
Notes
Availability of Data and Material
The data from this study cannot be made publicly available to protect participants’ information. Inquiries about the data can be referred to the corresponding author [HY, LEE, hylee@catholic.ac.kr].
Conflicts of Interest
The authors have no potential conflicts of interest to disclose.
Author Contributions
Conceptualization: Seongju Kim, Mi-Sun Lee, Hooyeon Lee. Formal Analysis: Seongju Kim, Mi-Sun Lee, Hooyeon Lee. Investigation: all authors. Methodology: Seongju Kim, Hooyeon Lee. Project administration: Hooyeon Lee. Data curation: Seongju Kim, Dong Jun Kim. Supervision: Hooyeon Lee. Validation: Seongju Kim, Hooyeon Lee. Visualization: Seongju Kim, Dong Jun Kim. Writing—original draft: Seongju Kim. Writing—review & editing: Mi-Sun Lee, Hooyeon Lee.
Funding Statement
This study was supported by the National R&D Program for Cancer Control through the National Cancer Center (NCC) funded by the Ministry of Health & Welfare, Republic of Korea (Grant number: HA21C0225) and the Catholic Medical Center Research Foundation made in the program year of 2022 (Grant number: 5-2022-B0001-00207).