Relationship Between Social Withdrawal (Hikikomori), Personality, and Coping in an Adult Population
Article information

Abstract
Objective
The aim of this study was to investigate the relationships between personality dimensions, coping strategies, and Hikikomori while controlling for the presence of depression and anxiety.
Methods
Two groups, recruited on social networks, were compared: the control group (n=101, mean age±standard deviation [SD]= 36.2±12.8 years) and the Hikikomori group (n=28, mean age±SD=30.1±9.1 years). Participants of both groups completed the Big Five Inventory, the Brief Coping Orientation to Problems Experienced, and the Hospital Anxiety and Depression Scale.
Results
The Hikikomori group had higher depression, anxiety, neuroticism, and dysfunctional coping dimension (self-blame and behavioral disengagement) scores than the control group. Being alone and depression were positively associated with Hikikomori while extraversion and instrumental support were negatively associated with Hikikomori.
Conclusion
These findings contribute to a better understanding of the psychological functioning of Hikikomori as well as to treatment elaboration and confirm that some psychological characteristics are transcultural.
INTRODUCTION
The Japanese term Hikikomori was used for the first time by Saito in 1998 [1]. This term designates the extreme, voluntary, and prolonged (6 months or more) withdrawal of adolescents and young adults to their home, avoiding social contacts, school, or professional activities [1,2]. In the literature, this term is usually translated as “social withdrawal” but also as “youth social withdrawal,” “housebound syndrome,” or “claustration syndrome.” In Japan, the term Hikikomori refers to both the phenomenon and the person affected by this withdrawal. Currently, the term Hikikomori is applied to individuals who do not leave their rooms or homes, and to individuals who are able to go out locally or for their hobbies but most often stay home [3]. In the lit-Print ISSN 1738-3684 / On-line ISSN 1976-3026 OPEN ACCESS erature, there is a distinction between “primary Hikikomori,” which presents no comorbidity, a “pure” form of social withdrawal, and “secondary Hikikomori,” which occurs due to a known mental disorder [4].
The first prevalence study was performed in Japan, where, in 2006, lifetime prevalence was estimated at 1.2% [5]. Hikikomori has now been identified in many other countries, such as Hong Kong, Spain, France, India, Korea, Ukraine, and the United States [6-10], and can be conceptualized as a “culturally boundless syndrome of modern society [11].” Despite heterogeneous results across studies, there are several common Hikikomori characteristics: onset around the age of 20 years with a largely male predominance [5,12], urban area living [6], and mostly occuring in high-income, developed countries, with a strong maternal presence [12-14]. Previous studies have reported that most Hikikomori who seek treatment in a health care centers have also suffered from a psychiatric disorder during their lifetime [5,15-17]. Nevertheless, whether it is the psychiatric disorders that generate the social withdrawal or whether the social withdrawal is the cause of the psychiatric disorders remains unclear [18].
Beyond psychiatric comorbidities, several studies have investigated the psychological functioning of individuals with Hikikomori, especially looking at personality. Some studies that evaluated personality disorders found a strong relationship between Hikikomori and avoidant personality disorder [19] or passive-aggressive personality disorder [20]. Other studies that focused on personality traits found difficulties in identifying and verbalizing emotions among individuals with Hikikomori [10,21]. Indeed, people with Hikikomori are more likely to express emotions indirectly and expect others to implicitly understand their feelings and thoughts [20]. More recently, Amendola et al. [22] found a strong relationship between Hikikomori and overall personality dysfunction. Nevertheless, only a few studies have investigated personality traits and none have done so according to the most dominant framework for measuring them: the Big Five personality traits. Indeed, the Big Five Inventory is one of the tools most widely used internationally to assess dimensions of personality.
Family relationships and their involvement in social withdrawal have been a subject of high interest in research on Hikikomori. However, the results have been heterogeneous regarding the presence or not of dysfunctional family functioning as a cause or consequence of Hikikomori [12,23]. Insecure attachments, especially avoidant and ambivalent attachment, have been associated with Hikikomori [24], highlighting vulnerability to situations of rejection. Indeed, social withdrawal often comes as a consequence of difficult socializing experiences, perceived as failures and avoided thereafter. Social withdrawal can also be linked to rejection of social success ideals [25] or to traumatic experiences such as school bullying or sexual abuse [26], thus instilling fear and distrust of the outside world amongst these individuals.
Experiences of failure, loneliness, and worthlessness are currently known suicide motives in Hikikomori [27]. Hikikomori can be seen as an expression of contemporary suffering on entering adulthood due to social and family pressures on youth in which the requirements for success are high [14]. Thus, some investigators have proposed that Hikikomori may be a (maladaptive) strategy to cope with the stress caused by social judgment [18]. Although the behavioral repertoire of families who cope with individuals with Hikikomori have been investigated [28], only one study has evaluated the different adjustment strategies used by the Hikikomori themselves. Thus, Nonaka and Sakai [29] found that Hikikomori was associated with the use of instrumental support and behavioral disengagement coping strategies. As highlighted by the authors, these findings need to be replicated in cultures outside of Japan to clarify whether there are cultural specificities in the psychological functioning of Hikikomori.
Thus, the aim of the present study was to explore the relationships between personality dimensions, coping strategies, and social withdrawal while controlling for the presence of depression and anxiety. Given that social withdrawal may be a sign of depression itself and may be seen as a marker of anxiety, and that the period during which the current study took place during the coronavirus disease-2019 (COVID-19) pandemic was associated with an increase in anxiety and depression due in part to isolation from others [30], it was important to control for the possible effect of psychological distress.
METHODS
Participants
Individuals (male and female) who were 18 years or older were included in this study conducted between January and September 2021. Participants were recruited from several general social network groups and one private group dedicated to Hikikomori: “Hikikomori France. Communauté francophone des Hikikomori et reclus sociaux” (all French speaking). After asking the administrators for their permission, we posted a message explaining the aim, duration, and anonymity of the study, as well as a link to the questionnaire (with a full explanatory note containing the ethical requirements). Participants who agreed to participate in the study had to provide their informed consent before accessing the questionnaires (for minors, one of the parents also had to give consent). For the Hikikomori social network group, the questionnaire was distributed by the group’s creator, known by the pseudonym Ael, himself being Hikikomori for the past 13 years.
All participants received information regarding the survey and all participants provided written informed consent to participate. Participants were excluded if they presented with a possible comorbid psychotic disorder (based on the L module of the Mini International Neuropsychiatric Interview [31]). The two groups (control group and Hikikomori group) were formed on the basis of the following measures: 1) their score on the 25-item Hikikomori Questionnaire (HQ-25) and 2) their answers to questions created for the study. These additional questions were asked for three reasons: 1) the high rate of false-positives on the HQ-25 [32]; 2) the restrictions linked to the COVID-19 pandemic situation when recruitment took place (during certain periods, a curfew had been imposed); and 3) the recent proposition by Kato and colleagues [18,33] to use “marked and continuous social isolation” (i.e., frequency of going out) as Hikikomori criteria, rather than avoidance of social interaction or staying at home as the main criteria. Thus, the additional questions were: 1) Outside of the current restrictions linked to COVID-19, how often do you go out alone or with friends for shopping, sports, or socializing? (once a week, several times a week, every day, once a month, less than once a month, almost never, and never); 2) Outside of the current restrictions linked to the COVID-19, do you only go outside for vital needs (food or medical appointment)? (yes, no); and 3) Does the current pandemic context have an impact on what you usually want to do in terms of outings, leisure, or any other activity outside your home? (yes, no, and not at all).
On this basis, individuals were included in the Hikikomori if they reached the HQ-25 cutoff score (≥42) and if they had the following specific answers to the 3 additional questions: “almost never” or “never” to the first question, “no” to the second question, and “no” or “not at all” to the third one.
The control group was composed of 101 participants (30 males, 70 females, 1 other; mean age±standard deviation [SD]=36.2±12.8 years). Most participants were either single (39.6%) or married or in a relationship (50.5%). The majority were employed (65.3%) and had less than a high school graduate education (84.2%). They either lived alone (44.0%) or with a partner (36.0%). Most had parents who lived together (45.5%).
The Hikikomori group was composed of 28 participants (13 males, 15 females; mean age±SD=30.1±9.1 years). Most were single (67.9%), unemployed (60.7%), and had less than a high school graduate education (75.0%). They either lived alone (39.3%) or with one parent (39.3%). Most had divorced parents (42.9%).
Measures
Participants’ characteristics were evaluated, including age, sex, education, and marital and professional status.
The HQ-25 [32] was used to assess the severity of Hikikomori symptoms during the preceding 6 months. This self-administered instrument composed of 25 items evaluates the psychological features and behavioral patterns of typical Hikikomori syndrome, such as lack of social connectedness, active social isolation or withdrawal behavior, avoidance of social contact, and a sense of alienation from society. All items of the HQ-25 were rated on a scale ranging from 0 (strongly disagree) to 4 (strongly agree). Authors of the HQ-25 proposed a cutoff score of 42 (out of 100), which was associated with a sensitivity of 94% and a specificity of 61% in their clinical study. In our study, the scale showed high internal consistency, with a Cronbach’s α of 0.92.
The French version of the Big Five Inventory (BFI-Fr) [34] is a 45-item self-report questionnaire that assesses five personality domains with two facets per domain: neuroticism (anxiety and emotional volatility), agreeableness (compassion and respectfulness), conscientiousness (organization and responsibility), extraversion (anxiety and emotional volatility), and openness (aesthetic sensitivity and creative imagination). All items of each dimension were rated on a scale from 1 (strongly disapprove) to 5 (strongly approve), for a total score ranging from 5 to 25 in each dimension. Each domain demonstrated high reliability and a clear factor structure. In the current study, the BFI-Fr yielded adequate internal consistencies for neuroticism (Cronbach’s α=0.83), agreeableness (Cronbach’s α=0.80), conscientiousness (Cronbach’s α=0.85), extraversion (Cronbach’s α=0.88), and openness (Cronbach’s α=0.80).
The Brief Coping Orientation to Problems Experienced (Brief-COPE), French version [35], was used to assess various coping styles. The scale consists of 28 questions, including 14 subscales (two questions per subscale) in a Likert scale format (0 to 4 points). These subscales, or coping styles, include active coping, instrumental support, planning, acceptance, emotional support, humor, positive reframing, religion, behavioral disengagement, denial, self-distraction, self-blame, substance use, and venting. In this study, the scale showed good internal consistency, with a Cronbach’s α of 0.70. The problem-focused coping dimension included active coping, planning, and instrumental support. The emotion-focused coping dimension included emotional support, religion, positive reframing, acceptance, humor, and venting. The dysfunctional coping dimension included self-blame, denial, self-distraction, behavioral disengagement, and substance use [35].
The French version of the Hospital Anxiety and Depression Scale (HADS [36]) is a14-item self-report scale that was used to screen participants for anxiety (seven items) and depression (seven items). This tool has good psychometric properties and is quick to administer and thus suitable for field research. Cutoff scores for the depression and anxiety subscales are as follows: 7 or 8 indicates “possible presence,” 10 or 11 suggests “probable presence,” and 14 or 15 refers to “severe presence.” In this study, the two subscales showed good internal consistency, with a Cronbach’s α of 0.80 for depression and 0.74 for anxiety.
Data analysis
All statistical analyses were performed with IBM SPSS software (version 20; IBM Corp., Armonk, NY, USA). For sociodemographic, personality, and coping characteristics, we used ttests or chi-squared tests for group differences (control group vs. Hikikomori group), with Cohen’s d or Cramer’s V for effect size for continuous or categorical variables, respectively. We considered d >0.5 as a medium effect size and d >0.8 as a large effect size [37]. To test group differences and because some cells had very small numbers (<5), we pooled some data: for sex, we eliminated “other,” and for marital status, we grouped together “single” and “divorced” and created a new variable called living situation (alone vs. not alone). Employment status was rephrased as “social participation” with two categories: “participation” (employment and enrolled in education) vs. “nonparticipation” (out of school and unemployed). Finally, education was included in tests with the categories “low” (less than high school diploma) vs. “high” (high school diploma and higher).
Secondly, multivariate analyses were conducted (logistic regressions). Pearson’s correlations were used to evaluate the relationships between variables. In order to test for the unique contributions of sociodemographic data (only age, social participation, and living situation were significant), depression and anxiety, personality (the 5 domains) and coping, a fourstep multiple regression analysis was performed. Odds ratios (ORs) and 95% confidence intervals were generated by using logistic regressions.
Ethical considerations
In France, it is not mandatory to seek an ethics committee when the population studied is not a clinical population and when the study does not investigate sensitive date. We adhered to basic ethical principles of research. This study was conducted in accordance with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. All participants received information regarding the survey and all participants provided written informed consent. When the participants agreed to participate in the study, they had to sign the informed consent before accessing the questionnaires. The study was carried out anonymously.
RESULTS
Descriptive data for the whole sample are presented in Table 1. The proportion of females and males in our two samples was equivalent, but the Hikikomori group was significantly younger than the control group (F(1)=5.44, p=0.021, d=0.54). Participants of the Hikikomori group were significantly more alone than those in the control group (φc=0.24, p=0.005) and less involved in social participation (φc=0.41, p<0.001).
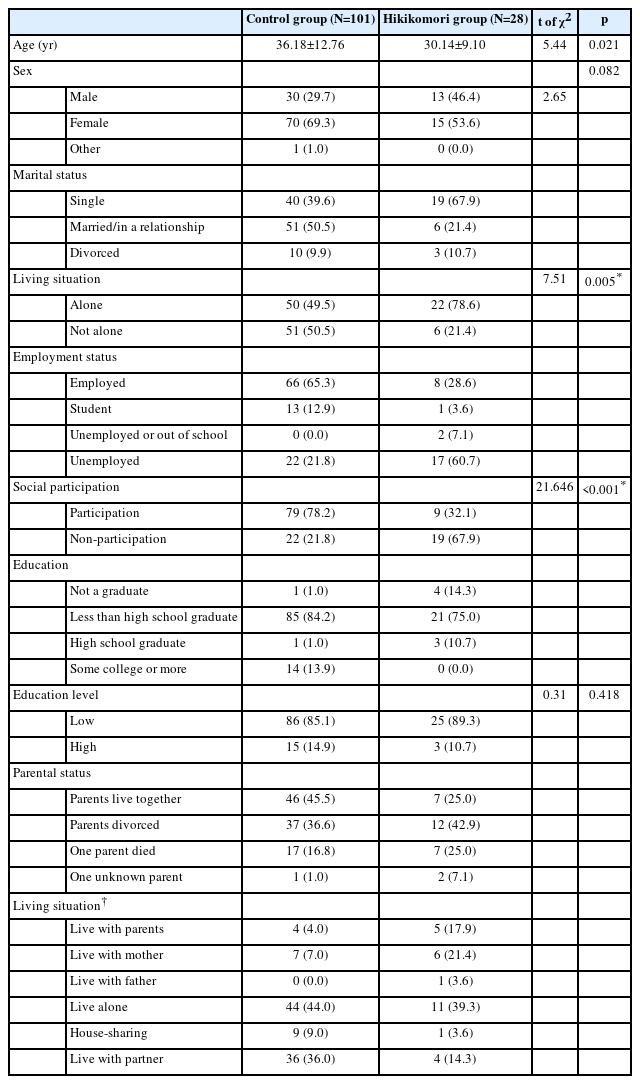
Sociodemographic characteristics of the social withdrawal (Hikikomori) and control groups
The Hikikomori group had higher depression and anxiety scores than the control group did, with a large effect size (F(1)=54.74, p<0.001, d=1.10 and F(1)=53.08, p<0.001, d=1.14, respectively). None of the control group had a score of probable or severe depression or anxiety (Table 2).
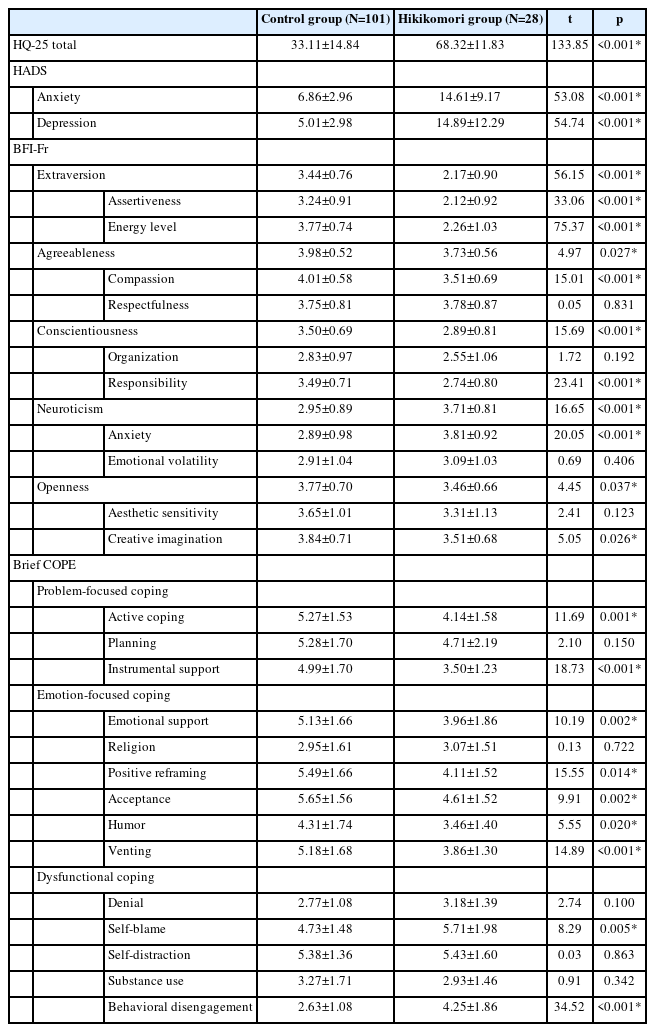
Psychopathological characteristics of the social withdrawal (Hikikomori) and control groups
Regarding personality dimensions, participants from the control group had significantly higher extraversion (F(1)=56.15; p<0.001; d=1.52), assertiveness (F(1)=33.06; p<0.001; d=1.24), energy level (F(1)=75.37; p<0.001; d=1.68), agreeableness (F(1)=4.97; p=0.027; d=0.46), compassion (F(1)=15.01; p< 0.001; d=0.78), conscientiousness (F(1)=15.69; p<0.001; d=0.81), responsibility (F(1)=23.41; p<0.001; d=0.99), openness (F(1)=4.45; p=0.037; d=0.46), and creative imagination (F(1)=5.05; p=0.026; d=0.47) scores than did those from the Hikikomori group, with effect size ranging from medium to large. In contrast, participants from the Hikikomori group had higher neuroticism (F(1)=16.65; p<0.001; d=0.89) and anxiety (F(1)=20.05; p<0.001; d=1.41) scores than did those from the control group, with a large effect size.
Regarding coping, participants from the Hikikomori group had significantly lower scores on the problem-focused coping dimensions, especially active coping (F(1)=11.69; p=0.001; d=0.73) and instrumental support (F(1)=18.73; p<0.001; d=1.00). They also had significantly lower scores on some emotion-focused coping dimensions: emotional support (F(1)=10.19; p=0.002; d=0.66), positive reframing (F(1)=15.55; p=0.014; d=0.87), acceptance (F(1)=9.91; p=0.002; d=0.67), humor (F(1)=5.55; p=0.020; d=0.54), and venting (F(1)=14.89; p<0.001; d=0.88). Finally, regarding the dysfunctional coping dimension, participants from the Hikikomori group had higher scores on self-blame (F(1)=8.29; p=0.005; d=0.56) and behavioral disengagement (F(1)=34.52; p<0.001; d=1.06) than did those from the control group.
Two factors were positively associated with Hikikomori (Table 3), being alone (OR=14.75, p=0.047) and depression (OR=1.94, p=0.030), respectively. In contrast, Hikikomori was negatively associated with extraversion (OR=0.04, p=0.013) and instrumental support (OR=0.11, p=0.011).

Factors associated with social withdrawal among the whole sample (four-step multiple logistic regressions)
DISCUSSION
To date, only a few studies have investigated the personality dimensions of Hikikomori and only one has explored coping strategies. The aim of this study was to explore the relationships between Hikikomori, personality, and coping while taking into account depression and anxiety.
Our Hikikomori sample had an equal proportion of male and female participants, in contrast to the male predominance highlighted in several previous studies [5,12]. Furthermore, our results showed that sex is not a risk factor associated with being Hikikomori, in line with a recent study that found a similar proportion of Hikikomori men and women [38]. Another interesting result was that even though individuals of the Hikikomori group were less involved in social participation than the control group, some of them did work. Thus, as in previous studies [9,10,38,39], some Hikikomori prefer to avoid social participation but are engaged in it by obligation, mostly for financial reasons.
Our results on personality dimensions showed higher neuroticism scores in the Hikikomori group, especially on the anxiety facet. This result is in line with the self-reported case study of Chong and Chan [40] that suggested that having an introverted personality plays a crucial role in a person becoming Hikikomori. Previous studies have found a relationship between neuroticism and a negative attitude toward events [41] that have interpersonal consequences. Indeed, individuals with high neuroticism scores tend to be less satisfied with their relationships overall [42-46] and have higher social deprivation [47]. Regarding relationships, intrapersonal theories [48] suggest that neurotic individuals “think in ways that lead to more negative perceptions of their interpersonal experiences, regardless of the objective quality of those experiences [49].” Personality shapes individuals’ perceptions of the world around them [50]; thus, the general tendency of neurotic individuals to experience negative emotions [51], especially in the interpersonal domain, could lead to avoidance of social situations and relationships (i.e., Hikikomori). Consequently, it is not surprising that extraversion was negatively associated with Hikikomori. Indeed, previous studies have demonstrated the influences of individuals’ personality on their environment and vice versa (individuals influence their environment and are, in return, influenced by their environment). For example, extraverted individuals may create a positive social environment through their own positive demeanor and may then be positively reinforced by their environment for their extraverted personality [52], because they are appreciated for it. Thus, in agreement with the state-effect model [53], one hypothesis is that the lack of contact with the environment (i.e., the lack of extraversion, extraversion which is negatively associated with Hikikomori in our study) may cause short-term personality changes as a result of their current Hikikomori disorder (i.e., Hikikomori have higher neuroticism scores but this personality dimension is not associated with Hikikomori). A longitudinal study is necessary to confirm this hypothesis.
Participants from the Hikikomori group also had significantly higher depression scores, and depression was positively associated with the risk of being Hikikomori. This result is similar to that of a previous study in which individuals who were reported to be lonely, isolated, or neurotic—as well as any combination thereof—were more depressed than were those who did not have these characteristics; the individuals in that study also had higher social deprivation [48]. Our results are similar to other studies that have highlighted a strong relationship between depression and both loneliness [54-56] and neuroticism [57,58]. In our study, being alone was highly associated with being Hikikomori (it increased the risk by almost 15 times).
Compared with members of the control group, Hikikomori used significantly more dysfunctional coping strategies, especially self-blame and behavioral disengagement, and less problem-focused and emotion-focused coping strategies. In the qualitative study of Yong and Kaneko [59], social withdrawal appeared to be a passive way of coping with existing problems. This coping type could be seen as a “specific adaptation to contemporary competitive social changes and the human relationships these changes produce [59].” It may be a way of creating a safe place where events are more predictable and less challenging. Taken together, our results confirm that neurotic individuals are “prone to cope more poorly than others with stress,” as posited by Costa and McCrae [51].
As in previous studies that found a relationship between ineffective coping styles and poorer mental health [60], Hikikomori tend to criticize themselves for a perceived sense of responsibility for the situation (self-blame) and tend to withdraw when faced with a stressful situation (behavioral disengagement). This is in line with a study on social anxiety in which frequent engagement in dysfunctional coping strategies was associated with higher degrees of social anxiety and related social impairment [61]. Thus, as suggested by Tran and Haaga [62] for social anxiety, Hikikomori cope with their anxiety by fleeing stressful situations. Nevertheless, in agreement with the results of Nonaka and Sakai’s study [29], only instrumental support was negatively associated with Hikikomori. According to the selfesteem and identity models, social support has an impact on self-esteem which contributes to less psychological distress [61]. Nevertheless, the inclination to use social support is linked to personality [61]. For example, individuals with poor social abilities will have difficulty accepting help without feeling inferior. Given the strong effect of self-esteem on depression [63] and the relationship between depression and Hikikomori in our study, it seems necessary to better understand the links between these variables.
Limitations and clinical implications
This study has several limitations. First, the cross-sectional nature of the study hinders the possibility of making any causality statements. Second, our sample is relatively small (n=129). As suggested by some authors, a small sample increases the risk that the relevance of specific factors remains undiscovered [64]. Despite our sample being relatively small, however, it included a significant proportion of Hikikomori (n=28). Nonetheless, our results should be replicated in a larger group of participants. Third, the small number of females did not allow us to investigate sex differences even if the Hikikomori group has a similar proportion of male and female. Because characteristics of Hikikomori manifest differently depending on sex [39], greater attention must be paid to sex differences in order to determine whether there are specificities of psychological functioning and, in particular, psychological processes involved in the occurrence of Hikikomori. Therefore, it seems important in future to include larger samples with a greater proportion of females to confirm our results in order to adapt treatment to gender specificities if relevant. Finally, as in a previous study on problematic internet use [65], collecting data during the French fourth wave of the COVID-19 pandemic allowed us to determine to what extent anxiety and depression had an impact on the occurrence of social withdrawal. Nevertheless, we cannot determine the effect of the COVID-19 pandemic on the development or aggravation of Hikikomori.
Despite these limitations, this study showed a strong positive relationship between living alone, depression, and Hikikomori on the one hand, and a strong negative relationship between extraversion, instrumental support, and Hikikomori on the other hand. Depression refers to the psychiatric level that is generally used to identify standardized treatment that targets specific syndromes [66]. Nevertheless, according to psychological models, psychiatric symptoms are a consequence of impaired or disturbed psychological processes [67]. Thus, it is important to further investigate and understand the specific psychological processes implicated in the occurrence of Hikikomori and its comorbidities (depression in our study). Our study is one of the first to have contributed to this understanding.
As evidence-based psychological interventions typically target psychological processes (e.g., dysfunctional emotional regulation processes, cognitive impairment) and not risk factors per se (e.g., personality dimensions), it is crucial to proceed with a process-based analysis when designing treatment [68-70]. An understanding of the specific psychological processes implicated in the onset and maintenance of the Hikikomori disorder will help tailor treatment depending on the specific psychological processes implicated [66]. Given the dysfunctional coping strategies identified in this study, Hikikomori would benefit from an intervention that specifically targets coping strategies. Nevertheless, given the relationship between depression and Hikikomori, they would also benefit from an intervention that targets the psychological processes implicated in the onset and maintenance of depression. Further studies need to clarify on the one hand the relationship between depression and Hikikomori (is one the consequence of the other, or are these two disorders independent); and on the other hand to determine if the psychological processes implicated in both Hikikomori and depression are similar. For example, self-blame is a core emotion in major depressive disorder [71] and self-blame was also higher in the Hikikomori of our study; thus, targeting this process would undoubtedly be useful for both social withdrawal and depression.
Notes
Availability of Data and Material
The datasets generated or analyzed during the study are available from the corresponding author on reasonable request.
Conflicts of Interest
The authors have no potential conflicts of interest to disclose.
Author Contributions
Conceptualization: Céline Bonnaire, Zoé Roignot. Data curation: Céline Bonnaire, Zoé Roignot. Investigation: Zoé Roignot. Methodology: Céline Bonnaire, Zoé Roignot. Project administration: Céline Bonnaire, Zoé Roignot. Supervision: Céline Bonnaire. Validation: Céline Bonnaire. Writing—original draft: Céline Bonnaire. Writing—review & editing: Céline Bonnaire, Zoé Roignot.
Funding Statement
None
Acknowledgements
We are grateful to all the individuals who participated in this study and we would particularly like to thank Ael without whom we would not have had access to his community. We would also like to thank Barbara Every for English language editing.