Psychosocial Factors Influencing Quality of Life Among Medical Students
Article information

Abstract
Objective
This study investigated the influence of psychosocial factors on medical students’ quality of life (QOL).
Methods
A total of 408 medical students participated in this study. We collected data on participants’ sociodemographic details, symptoms of depression and Internet addiction, self-esteem, social support, and QOL. QOL was assessed using the World Health Organization Quality of Life-Abbreviated form, which has four domains (physical health, psychological health, social relationships, and environment). A stepwise multiple linear regression model was constructed to identify factors’ independent impact on QOL.
Results
Higher levels of depression and Internet addiction were associated with lower scores in all domains of QOL, whereas higher levels of self-esteem and social support were associated with higher scores. Being in third-year versus first-year was associated with higher scores in the physical health and environment domains. Living alone or in dormitories, low or middle socioeconomic status, and insufficient or moderate pocket money were associated with lower scores in the environment domain. Additionally, female students displayed significantly lower scores for physical health, psychological health, and environment than male students, but not for social relationships. There were significant differences in certain domains of QOL due to sociodemographic factors.
Conclusion
This study demonstrates the psychosocial factors influencing medical students’ QOL. Educational strategies focusing on strengthening self-esteem and social support as well as preventing depression and Internet addiction may contribute to improving medical students’ QOL.
INTRODUCTION
The medical education course is considerably long and demanding and seems to harm medical students’ mental health [1]. Although medical students are inclined to experience less stress regarding future opportunities and employment than their non-medical peers, they suffer from academic stress due to a heavy workload, fear of failing, extreme competition, sleep deprivation, and exposure to patient deaths [2]. Due to these stressors, medical students are at a higher risk of experiencing psychological distress or mental health problems than the general population and/or age-matched peers [2]. It has been reported that a substantial amount of medical students experience depression, burnout, anxiety, Internet addiction (IA), and suicidal ideation [3,4]. These psychological problems, along with socioeconomic factors such as financial difficulties, may negatively affect medical students’ quality of life (QOL).
QOL is an individual’s perception of their position in life in the context of their culture and value systems in relation to their goals, expectations, standards, and concerns [5]. As a multidimensional construct, QOL can be viewed through subjective domains, such as life satisfaction, and objective domains encompassing physical, material, emotional, and social wellbeing as well as development and activity [6]. Assessing medical students’ QOL can provide comprehensive information on their overall health, including physical, psychological, and social well-being. Lower levels of QOL in medical students is associated with adverse events, including academic failure, mental health problems, and other negative effects on their future professional development and health [7,8]. Thus, it is important to elucidate the factors influencing medical students’ QOL.
Among the various psychological symptoms, depression and IA have been the focus of research for medical students, as they are more prevalent in this population than in the general population [2,4]. Medical students with depression or IA had significantly lower academic performance compared to peers who did not have these disorders [9]. Particularly, depression was a major risk factor for suicidal ideation and behavior and a significant predictor of lower QOL in medical students [10]. Furthermore, a significant negative association between medical students’ IA and QOL has been found [11]. Sex and specific factors related to medical education, such as the year of study, have been reported to significantly predict medical students’ health-related QOL [12].
Self-esteem is the direction of self-attitude, a favorable or unfavorable opinion of oneself, and an important factor closely associated with various psychopathologies. Low self-esteem has been shown to increase the risk of experiencing depressive symptoms, whereas high self-esteem has been shown to protect against depressive moods [13]. Furthermore, self-esteem is a powerful predictor of life satisfaction [14]. A recent study revealed a strong association between QOL, self-esteem, and self-efficacy in adolescents, implying the critical role of psychosocial factors in QOL [15].
Social support has been shown to have beneficial effects on physical and mental health [16]. Social support is derived from a network of family, friends, and community. In a study among university students, it was found that social support from family and friends played a significant role in increasing psychological QOL [17]. In contrast, low social support is significantly associated with mental health problems among college students [18].
Previous studies on medical students’ QOL have mainly investigated the impact of sociodemographic and academic factors, with limited studies examining the association between QOL and psychological symptoms, self-esteem, and social support. Moreover, there have only been a few studies on the predictors and associated factors of medical students’ QOL in Korea. Thus, the present study aimed to examine the impact of sociodemographic and psychosocial factors (depression, IA, self-esteem, and social support) on medical students’ QOL.
METHODS
This cross-sectional study was conducted among medical students at Chosun University. The curriculum of Chosun Medical School is six years long with the first two years comprising pre-medical education. The participants were selected using the convenience sampling method. Written informed consent was obtained after the purpose and procedures of the study had been explained by a researcher with no relationship of the medical students. The data collection procedures are described in Seo et al. [19] 2021. Participants completed a selfreport questionnaire comprising of items on their sociodemographic characteristics, depression, IA, self-esteem, social support, and QOL. This study was approved by the Institutional Review Board at Chosun University (IRB No. 2-1041055-AB-N-01-2019-23).
Sociodemographic data
Data on participants’ age, sex, school year, residence type, socioeconomic status, and perception of their pocket money were obtained. Analyses applied to the following categories: sex (male and female), school year (first–fourth year), residence type (living alone, in a dormitory, or with family), perceived socioeconomic status (low, middle, or high), and perceived level of pocket money (insufficient, moderate, or sufficient).
QOL: World Health Organization Quality of Life-Abbreviated form
QOL was assessed using the World Health Organization Quality of Life-Abbreviated form (WHOQOL-BREF), a 26-item questionnaire in which each item is rated on a 5-point Likert (1–5) scale, with higher scores indicating better QOL. WHOQOL-BREF evaluates the four major QOL domains defined by the WHO; physical health, psychological health, social relationships, and environment. The raw scores of each domain are converted to a 0 to 100 scale to facilitate comparisons with other data. The Korean version of the WHOQOL-BREF was found to be both valid and reliable among the Korean population [20].
Psychosocial factors
The severity of depression was evaluated using the Beck Depression Inventory (BDI), which consists of 21 items [21]. Each item of the BDI is rated on a 4-point (0–3) scale, and the total score ranges from 0–63 with a higher score indicating more severe depression. The Korean version of the BDI was standardized by Rhee and colleagues [22,23]. The internal consistency of the Korean BDI has been reported to range from 0.85 to 0.87 [22,23]. The severity of IA symptoms was assessed using the Internet Addiction Test (IAT), which is a 20-item scale [24]. Each item is rated on a 6-point (0–5) scale with a higher score indicating more severe IA. The validity and reliability of the Korean version of the IAT have been confirmed [25]. The Korean version of the IAT has good internal consistency, with a Cronbach’s α of 0.91 [25]. Self-esteem was assessed using the Rosenberg Self-Esteem scale (RSES) [26]. The RSES consists of five positive and five negative questions reflecting high and low self-esteem, respectively. Each item is rated from 1 (strongly disagree) to 4 (strongly agree); however, negative items are inversely rated. The RSES total score ranges from 10 to 40, with a higher score indicating higher self-esteem. The Korean version of the RSES showed sound reliability and validity, with a Cronbach’s α of 0.90 [27]. The Duke-University of North Carolina Functional Social Support Questionnaire (Duke-UNC FSSQ) was used to evaluate social support. The eight items of the Duke-UNC FSSQ, consisting of two subscales (confidant and affective support), were used to calculate the mean social support score [28]. Responses to each item are rated on a 5-point (1–5) scale, with higher scores indicating a higher level of overall social support. The Korean version of the Duke-UNC FSSQ is reported to have high reliability and moderate validity, with a Cronbach’s α of 0.89 [29].
Statistical analysis
Continuous variables were checked for normal distribution using the Kolmogorov-Smirnov test. Since all continuous data were non-normally distributed, nonparametric tests were applied for analysis. Comparisons for differences between each domain of WHOQOL-BREF based on sociodemographic factors were performed using the Mann-Whitney U test or Kruskal-Wallis test. A Spearman’s rank correlation test was conducted to identify the correlation between psychosocial factors and each domain of WHOQOL-BREF. Further, factors significantly related to each WHOQOL-BREF domain per the univariate analyses were entered into multivariate regression models as independent variables. Multiple linear regression analyses using stepwise variable selection were performed to assess the relative contributions of individual sociodemographic and psychosocial factors to each domain of WHOQOL-BREF. Significance was set at p<0.05 (two-tailed) and Bonferroni correction was performed when necessary. All statistical analyses were performed using IBM SPSS version 27.0 for Windows (IBM Corp., Armonk, NY, USA).
RESULTS
Sociodemographic and psychosocial characteristics
A total of 418 medical students participated in this study. Excluding 10 invalid questionnaires (those with >25% questions of unanswered), 408 completed self-report questionnaires were analyzed. Descriptive data on sociodemographic and psychosocial characteristics are presented in Table 1. The mean± standard deviation (range) scores of the four WHOQOL-BREF domains were as follows: physical health, 64.8±17.6 (0–100); psychological health, 61.2±19.4 (0–100); social relationships, 62.8±17.5 (0–100); environment, 65.9±16.7 (6–100).
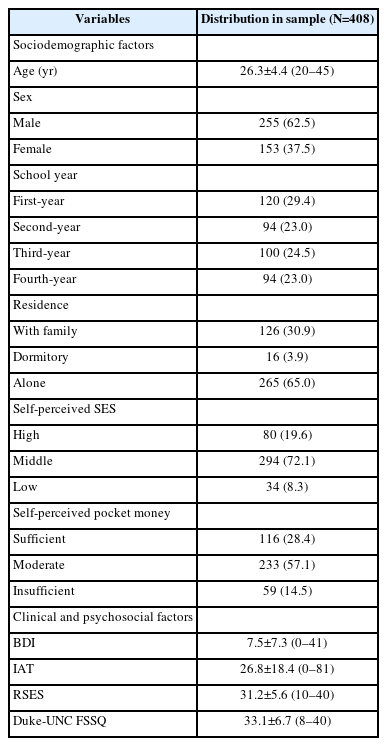
Participants’ sociodemographic and psychosocial characteristics
Comparisons of QOL based on sociodemographic factors
Female students showed significantly lower scores than male students in the physical health, psychological health, and environment domains of QOL. There were significant differences in physical health, social relationships, and environment domains regarding school year. In post-hoc analyses, first-year students had significantly lower scores in physical health than third-year and fourth-year students. Physical health scores were significantly lower in second-year students compared to third-year and fourth-year students. Regarding social relationships, second-year students had significantly lower scores than third-year and fourth-year students. Regarding the environment domain, first-year and second-year students showed significantly lower scores than third-year students. Comparing QOL based on sociodemographic factors, excluding sex and school year, significant differences were found only in the environment domain. Post-hoc analyses for the environment domain are as follows: students living with family showed significantly higher scores than those living in a dormitory or living alone; students living alone had significantly higher scores than those living in a dormitory. Regarding socioeconomic status, students who perceived themselves as having high socioeconomic status showed significantly higher scores than those who perceived themselves of middle or low socioeconomic status. Students who perceived themselves of middle socioeconomic status showed significantly higher scores than those who perceived themselves as having low socioeconomic status. Regarding pocket money, students who perceived that they received sufficient pocket money exhibited significantly higher scores than those who perceived that they received moderate or insufficient pocket money. Students who perceived that they received moderate pocket money showed significantly higher scores than those who perceived that they received insufficient pocket money. Comparisons of the four WHOQOL-BREF domains based on the sociodemographic factors are presented in Table 2, and the results of post-hoc comparisons are presented in Figures 1 and 2.
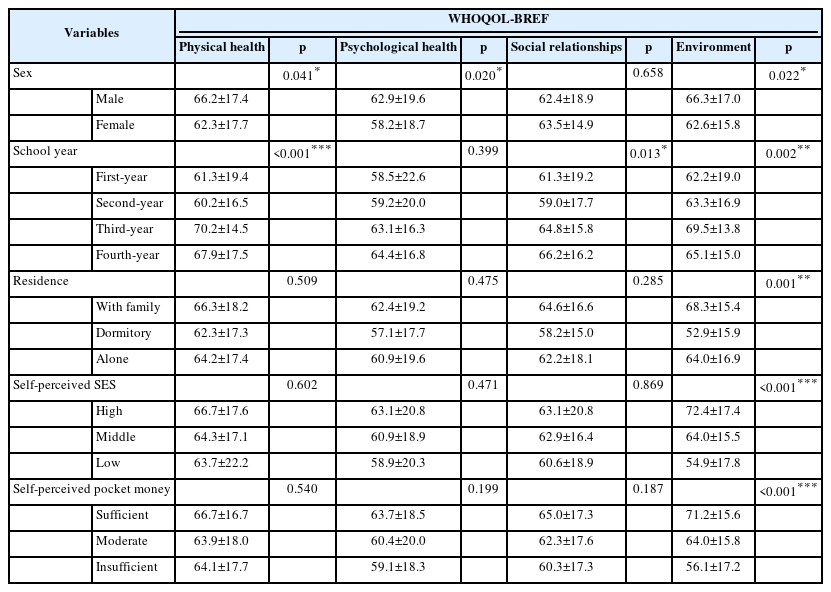
Comparison of WHOQOL-BREF according to participants’ sociodemographic factors
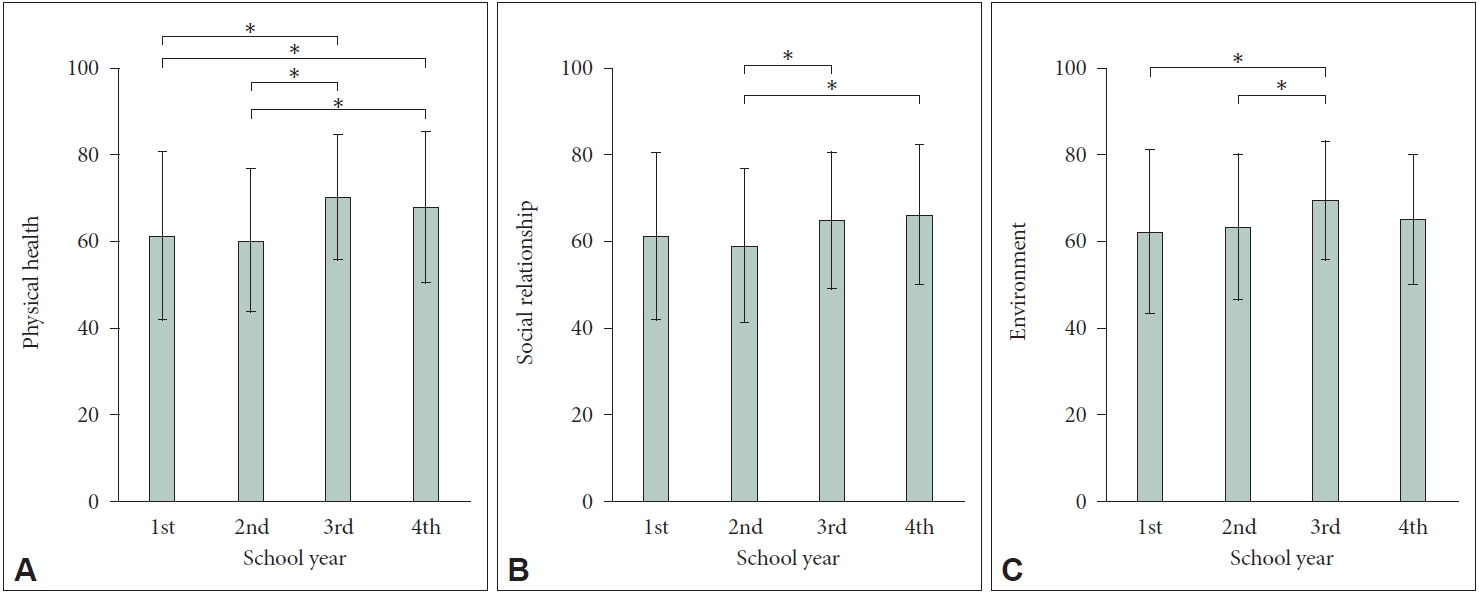
Post-hoc comparisons of the physical health (A), social relationships (B), and environment (C) domains of the WHOQOL-BREF according to school year. *p<0.008 (adjusted p-value by Bonferroni’s correction). WHOQOL-BREF, World Health Organization Quality of Life- Abbreviated form.
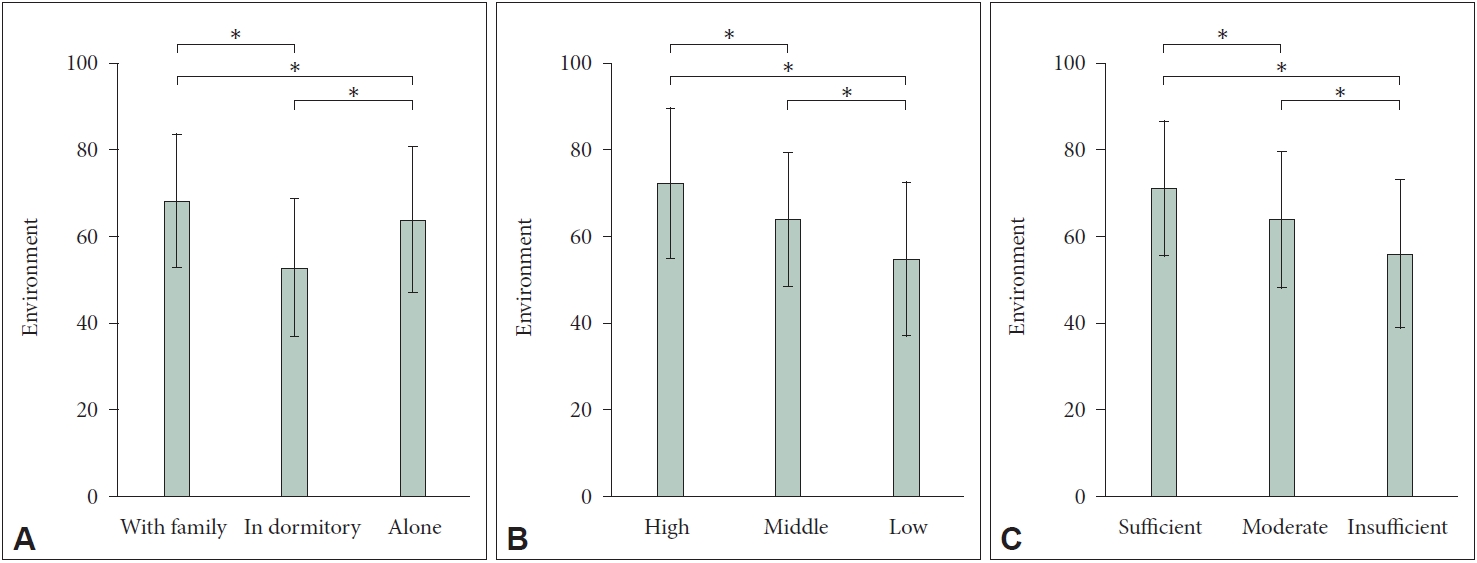
Post-hoc comparisons of environment domain of the WHOQOL-BREF according to residence (A), self-perceived SES (B), and self-perceived pocket money (C). *p<0.017 (adjusted p-value by Bonferroni’s correction). WHOQOL-BREF, World Health Organization Quality of Life-Abbreviated form; SES, socioeconomic status.
Correlations between psychosocial factors and QOL
The total scores for the BDI and IAT showed a significant negative correlation with the scores of the four domains of the WHOQOL-BREF. Contrastingly, the total scores for the RSES and Duke-UNC FSSQ showed a significant positive correlation with the four domains of the WHOQOL-BREF. Spearman’s ρ for the WHOQOL-BREF domains regarding depression, IA, self-esteem, and social support are presented in Table 3.
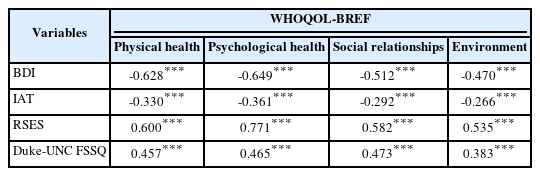
Spearman’s rank correlation of WHOQOL-BREF with psychosocial factors
Impact of sociodemographic and psychosocial factors on QOL
Being in third-year versus first-year was independently associated with higher scores in the physical health and environment domains. Living alone and living in a dormitory versus living with family were independently associated with lower scores in the environment domain. Self-perceived middle and low socioeconomic status as compared to self-perceived high socioeconomic status were independently associated with lower scores in the environment domain. Self-perceived moderate and insufficient pocket money versus self-perceived sufficient pocket money were independently associated with lower scores in the environment domain. Higher BDI and IAT scores were independently associated with lower scores in the four WHOQOL-BREF domains. Meanwhile, higher RSES and Duke-UNC FSSQ scores were independently associated with higher scores in the four WHOQOL-BREF domains. Associations between the four WHOQOL-BREF domain scores and significant independent variables are summarized in Table 4.

Multivariate associations of WHOQOL-BREF with sociodemographic and psychosocial factors
DISCUSSION
The main findings of our study were as follows: 1) symptoms of depression and IA were negatively associated with all QOL domains; 2) self-esteem and social support were positively associated with all QOL domains; 3) being in third-year versus first-year was associated with higher scores in the physical health and environment domains; 4) residence type, self-perceived socioeconomic status, and pocket money were only associated with the environment domain; and 5) there were significant differences in the level of specific domains of QOL based on medical students’ sex, school year, residence type, and self-perceived socioeconomic status and pocket money.
Our study demonstrated a significant negative association between symptoms of depression and IA levels and all domains of QOL. Additionally, the severity of depression and IA were negatively correlated with all domains of QOL. These results are in concordance with the results of previous studies [11,12]. The strong correlation between QOL and depressive symptoms has been well researched [30]. In one clinical sample, depression was found to severely worsen QOL, even when controlling for age [31]. In a study among college students, IA was negatively related to all domains of QOL, and various manifestations of IA were differentially associated with different domains of QOL [32]. However, few studies have examined the impact of depression and IA on medical students’ QOL. Our findings suggest that both depression and IA are associated with poor QOL among medical students. Moreover, symptoms of depression and IA can interact with each other, further worsening both [33]. Considering the substantial prevalence of depression and IA [3,4], our results underscore the need to address these issues and improve medical students’ overall QOL.
Contrary to symptoms of depression and IA, self-esteem and social support were positively correlated with QOL. Further, multiple linear regression indicated that medical students who had higher levels of self-esteem and social support scored higher on all domains of QOL. These findings were in line with prior studies regarding the effect of self-esteem and social support on QOL [15,17]. Particularly, we found that self-esteem was the strongest predictor of better QOL. People with low self-esteem tend to dwell on their weaknesses or defects rather than their strengths, which may be associated with depression and poor QOL. Meanwhile, high self-esteem has been shown to play a protective role against IA in medical students [34]. To our knowledge, this is the first study to examine the impact of self-esteem on various QOL domains in a sample of medical students. Our findings suggest that self-esteem plays a key role in improving QOL and buffering psychological symptoms. Social support was also found to have a positive association with QOL. A social network and social interactions are important factors for psychological well-being [35]. Social engagement was found to be an important factor in medical students’ psychological QOL [36] and medical students reported that meaningful relationships with family, friends, or teachers increased their QOL [37]. Our results support the viewpoint that social support is a valuable resource for medical students and that it improves their QOL across all domains. Taken together, educational strategies aimed at enhancing self-esteem and social support from peers and educators could contribute to the improvement of medical students’ well-being.
In our study, being in third-year compared to being in first-year was independently associated with higher QOL in the physical health and environment domains. Moreover, post-hoc analyses revealed that students in lower years of study (first-or second-year) compared to those in higher years (third- or fourth-year) reported poorer QOL in the physical health, social relationships, and environment domains. These results are somewhat contradictory to previous studies in Brazil [12] and China [38] in which students in third-year showed greater impairment in QOL than those in first-year. In Brazilian and Chinese medical schools, third-year students have a greater academic load as they transition to clinical training. Meanwhile, in Korean medical schools, the amount of learning and testing in pre-medical courses is considerably less than that in medical education. The first year of medical education is a transitional period in which students develop self-control to manage the abrupt increase in their academic load. In fact, the majority of failures tend to occur in the first-year in Korean medical schools. Thus, the academic stress resulting from failing may result in poorer QOL. The differing curricula and related issues may partly account for the differences regarding the association between school year and QOL. Regardless of such differences, our findings indicate that special attention is needed to improve the well-being of Korean medical students during their preclinical years of study.
Previous studies have reported that living in a dormitory versus living with family and lower economic class are associated with poorer QOL in all domains [36,39]. Meanwhile, this study demonstrates that type of residence and financial status are predictors of poorer QOL only in the environmental domain. In addition, significant differences were observed solely in the environmental domain in post-hoc comparisons of QOL according to residence type and economic level. This may result from a potential gap in support for the dormitory system or the high tuition rates of medical schools across countries. Even though real financial problems were not evaluated, our findings suggest that the impact of residence type and self-perceived economic status on Korean medical students’ well-being may be relatively limited to the environmental aspect.
Although sex was not a significant predictor of QOL, female students scored significantly lower compared to male students in physical and psychological health as well as environment domains. This is comparable to results from the study by Zhang et al. [38], 2012. Poorer QOL in the physical and psychological domains may reflect female students’ vulnerability toward the stressful nature of medical education, suggesting that more attention toward their physical and psychological well-being is needed. However, this susceptibility was not found in social relationships. A previous study showed that women are more focused on relationships than men [40]. Sex differences regarding investment in relationships may explain female students’ higher scores in the social relationship domain.
Despite the meaningful implications of the present study, some limitations and future directions need to be discussed. First, since the design of our study was cross-sectional, it is difficult to make causal inferences. A prospective study is needed to establish the causal relationship between sociodemographic and psychosocial factors and medical students’ QOL. Second, since the participants were attending the same medical school, the data may not be generalizable to other medical schools. Third, there is the potential for sampling bias as the selection of participants was conducted through convenience sampling. Fourth, although the WHOQOL-BREF allowed a multidimensional assessment of QOL, the present study did not evaluate some relevant key issues of medical education, including satisfaction with medical training and career choice, which may affect students’ QOL. Additionally, the relationship between other factors, such as academic workload, hierarchical culture of medicine, and QOL requires further investigation. Finally, our findings should be carefully interpreted due to the reliance of self-report measures.
In conclusion, the present study demonstrated the significant psychosocial factors influencing medical students’ QOL. Although the association between a variety of variables and medical students’ well-being is not yet sufficiently investigated, our results suggest that educational strategies focusing on enhancing self-esteem and social support as well as preventing depression and IA could contribute to improving medical students’ overall QOL. These findings underline the importance of systematic prevention approaches for mental health problems and active support from educators for medical students’ well-being.
Notes
Availability of Data and Material
Hyung-Jun Yoon had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Conflicts of Interest
The authors have no potential conflicts of interest to disclose.
Author Contributions
Conceptualization: Eun Hyun Seo, Hyung-Jun Yoon. Data curation: Eun Hyun Seo, Hyung-Jun Yoon. Formal analysis: Seung-Gon Kim, Jae-Hon Lee, Hyung-Jun Yoon. Funding acquisition: Hyung-Jun Yoon. Investigation: Eun Hyun Seo, Seung-Gon Kim, Jae-Hon Lee, Chandlee C. Dickey, Hyung-Jun Yoon. Methodology: Mella Y. Kim, Ravneet Kaur Ghumman. Project administration: Hyung-Jun Yoon. Writing—original draft: Eun Hyun Seo, Hyung-Jun Yoon. Writing—review & editing: Jae-Hon Lee, Chandlee C. Dickey, Mella Y. Kim, Ravneet Kaur Ghumman.
Funding Statement
This study was supported by research fund from Chosun University(2022).