Patient’s Perspective on Psychiatric Drugs: A Multicenter Survey-Based Study
Article information

Abstract
Objective
We aimed to identify the expectations and preferences for medication and medical decision-making in patients with major psychiatric disorders.
Methods
A survey was conducted among patients with major psychiatric disorders who visited psychiatric outpatient clinics at 15 hospitals between 2016 and 2018 in Korea. The survey consisted of 12 questions about demographic variables and opinions on their expectations for medication, important medical decision-makers, and preferred drug type. The most preferred value in each category in the total population was identified, and differences in the preference ratio of each item among the disease groups were compared.
Results
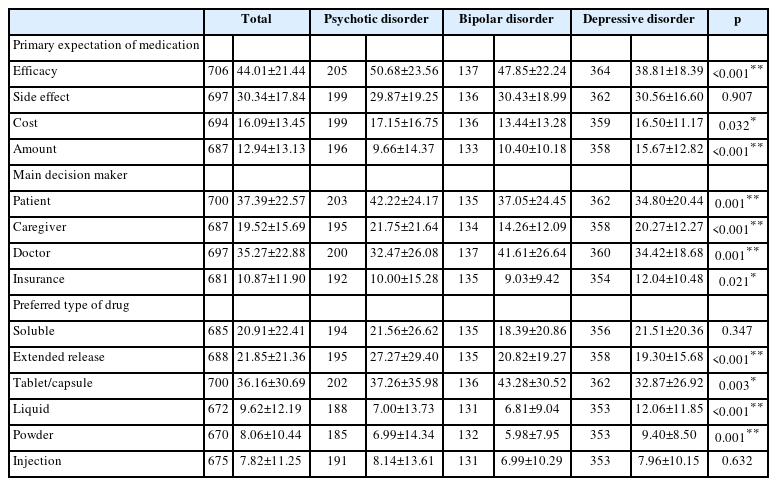
A total of 707 participants were surveyed. In the total population, patients reported high efficacy (44.01%±21.44%) as the main wish for medication, themselves (37.39%±22.57%) and a doctor (35.27%±22.88%) as the main decision makers, and tablet/capsule (36.16%±30.69%) as the preferred type of drug. In the depressive disorders group, the preference ratio of high efficacy was significantly lower, and the preference ratio of a small amount was significantly higher than that of the psychotic disorder and bipolar disorder groups. The preference ratio of a doctor as an important decision maker in the bipolar disorder group was higher compared to the other groups.
Conclusion
This study revealed the preference for medications and showed differences among patients with psychiatric disorders. Providing personalized medicine that considers a patient’s preference for the drug may contribute to the improvement of drug compliance and outcomes.
INTRODUCTION
According to the Global Burden of Disease Study (GBD) 2019, mental disorders remain one of the top 10 leading causes of disease burden worldwide. In the study using these results to report trends in the burden of diseases, injuries, and risk factors, depression, bipolar disorder, and schizophrenia were among the top 25 in the Years Lived with Disability (YLDs) ranking [1]. This shows that these major mental disorders cause a significant burden, and medication plays an important role in their treatment as it affects the prognosis and course of these diseases [2]. Therefore, medication adherence, which is defined as “the degree to which the patient acts according to the prescribed set interval and dosage of the drug,” [3] is an essential issue. However patients with mental disorders tend to avoid taking drugs compared to other patients with physical disorders [4]. As poor adherence may lead to disease recurrence, repeated and long-term hospitalization, loss of productivity, increased mortality, extended treatment period, and national economic losses, drug compliance is an important issue from both the quality of life and health economics perspectives [5].
Numerous studies have identified a variety of factors that influence medication adherence in psychiatric patients [6] as well as factors associated with adherence/nonadherence within specific disease groups. In the study of patients with schizophrenia, negative attitudes or subjective response to medication, previous nonadherence, and poor therapeutic alliance were associated with nonadherence [7]. Drug side effects were most commonly reported reason for treatment discontinuation in patients with depression [8,9] and other motivating factors for adherence included trust in medical staff, one’s will to treat disease, convenience in taking the drug formulation (method, frequency, simplicity of operation, etc.), and the appearance of the drug (perceptual aspects such as size, number, color, etc.) [8]. In patients with bipolar disorder, poor drug adherence was associated with considerably higher risks of relapse, recurrence, hospitalization, and suicide attempts, as well as lower chances of achieving remission and recovery [10,11]. Also side effects, complicated drug regimens, unfavorable attitudes toward medicine, lack of insight, and poor therapeutic relationships were contributing factors [9].
From these results, we can suspect that the factors affecting adherence reflect patients’ expectations, attitudes, and values about medication and that there are some differences between disease groups. It is now more important than ever to understand what patients’ value because of the recent rise of patientcentered care, where treatment decision-makings are made by everyone, not just doctors. Also, if people with different psychiatric disorders differ in the degree to which they value certain values related to adherence, then incorporating these factors into treatment may increase adherence and potentially lead to better treatment outcomes. However, few studies have compared differences between disease groups, and multicenter studies are even rarer.
Therefore, we conducted a multicenter survey-based study which was designed to examine the expectations for medication among patients who were diagnosed with depressive disorder, bipolar disorder, or psychotic disorder and the results will help us understand their expectations and preferences for medication and determine if there are differences between conditions.
METHODS
Participants and procedure
This study was performed using a nationwide survey of 15 Korean hospitals, which consisted of 11 university hospitals (The Catholic University of Korea Yeouido St. Mary’s Hospital, Jeju National University Hospital, SoonChunHyang University Cheonan Hospital, Inje University Haeundae Paik Hospital, Jeonbuk National University Hospital, Chung-Ang University Hospital, Konkuk University Chungju Hospital, Kyungpook National University Hospital, Dongguk University Gyeongju Hospital, Wonkwang University Hospital, and Daegu Catholic University Medical Center), one general hospital (Kangbuk Samsung Hospital), and three mental hospitals (National Center for Mental Health, Naju National Hospital, and Keyo Hospital). This study was conducted between January 2016 and December 2018. The study protocol was approved by the Office of Human Research Protection of the Catholic University of Korea, Yeouido St. Mary’s Hospital (IRB no. SCMC08MT095). The survey was performed with the approval of the institutional review board at each site.
Patients who were 18 years of age or older and visited the outpatient clinics were asked to participate in the survey. Patients who understood the purpose and contents of the study and agreed to participate signed the written consent form. Patients who refused to participate in the survey or did not complete the survey were excluded.
Measures
The survey was developed to understand patients’ expectation and preferences for treatment, and the questions were constructed through meetings and discussions among the research group of board-certified psychiatrists. The final survey consisted of demographic variables (age, sex, marital status, education, and economic status) and 12 questions: two questions to write psychiatric diagnosis, weight, and height; four questions to check medical history (hypertension, diabetes, and hyperlipidemia) and smoking status; three Likert questions asking how long you have been taking the drug, how long you have to take it in the future, and how satisfied you are with the drug treatment; and three constant sum questions asking about the wish for the drug, main treatment decision maker, and preferred formulation.
First, participants were asked about their age, sex (male/female), and marital status (married/not married). The education level (elementary school, middle school, high school, university, graduate school) was checked, and based on high school graduation (12 years), it was classified as <12 years or >12 years. Socioeconomic status was classified by annual income (<20 million KRW, 20–50 million KRW, >50 million KRW).
Patients were asked to write the names of the diseases that they were being treated for or were going to be treated for (Question 1, Q1) and their weight and height (Q2). They were asked to answer questions about their medical conditions, such as whether they had been diagnosed with diabetes (Q3), hypertension (Q4), or hyperlipidemia (Q5) and whether they were currently smoking (Q6).
The next three Likert scale questions asked the following: how long they had been taking medication in the past (0–1, 1–6, 6–12, 12–24, 24–60, >60 months) (Q7), how long they thought they should be taking medication in the future (0–1, 1–6, 6–12, 12–24, 24–60, >60 months) (Q8), and how satisfied they were from taking medication (completely dissatisfied, mostly dissatisfied, somewhat dissatisfied, neither satisfied nor dissatisfied, somewhat satisfied, mostly satisfied, completely satisfied) (Q9).
The following three constant sum questions were about various aspects of drugs that patients would consider important during their treatment: main wish for drugs (high efficacy, low side effects, low costs, lesser number of drugs) (Q10); main decision maker (patient, caregiver, doctor, health authority); and the preferred form of medications (soluble, extended-release, tablet, capsule, liquid, powder, injection) (Q12). They were asked to write the percentage of how much they valued each option, and the total should add up to 100.
Lastly, the attending psychiatrist examined the primary diagnosis and according to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) [12] diagnostic criteria and clinical judgment, the patient was classified into three groups; psychotic disorder (which includes schizophrenia, schizoaffective disorder, and other psychotic disorders), bipolar disorder (which includes bipolar disorder, manic episode, depressive episode, mixed features, remission or partial remission state), and depressive disorder (major depressive disorder, remission or partial remission, persistent depressive disorder, and other depressive disorders). Then, the psychiatrist measured the Clinical Global Impression-Severity (CGIS) and Improvement (CGI-I) scores on 7-point Likert scale and the level of insight on a 6-point Likert scale.
Statistical analysis
The analysis of variance test was performed to compare between groups according to the diagnosis made by one’s psychiatrist. When there was a significant difference across the disease groups (p<0.05), Tukey’s test was used to identify the disease diagnoses that showed the difference.
RESULTS
Demographic data
A total of 707 patients (mean age=44.3±13.6 years, 355 [50.2%] females, 206 [29.1%] with psychotic disorders, 137 [19.4%] with bipolar disorders, and 364 [51.5%] with depressive disorders) were recruited. More than half of the patients who had been taking psychiatric medications for >2 years (444, 62.8%), were expected to take medications for >2 years (387, 54.7%), and were satisfied with their medications (447, 63.2%). Most patients had better than moderate levels of CGI-S (669, 94.6%) and showed improvement in CGI-I (627, 88.7%) (Table 1).

Demographic and clinical characteristics of the subjects
In the psychotic disorders group, the mean age of patients was 46.5±15.4 years, and 110 (42.3%) of them were females. Less than half of the patients had been taking psychiatric medications for >2 years (87, 42.2%), but more than half of the patients with psychotic disorders were expected to take medications for >1 year (132, 64.1%), and were satisfied with their medications (121, 58.7%). In addition, most patients had better than moderate levels of CGI-S (198, 96.1%) and showed improvement in CGI-I (193, 93.7%).
In the bipolar disorders group, the mean age of patients was 42.3±13.8 years, and 77 (56.2%) of them were females. More than half of the patients who had been taking psychiatric medications for >2 years (82, 59.9%), were expected to take medications for >1 year (93, 67.9%), and were satisfied with their medications (99, 72.3%). Most patients had better than moderate levels of CGI-S (133, 97.1%) and showed improvement in CGI-I (132, 96.4%).
In the depressive disorders group, the mean age of patients was 43.8±12.3 years, and 168 (46.2%) of them were females. Most of them had been taking psychiatric medications for >2 years (275, 75.5%) and more than half of the patients were expected to take medications for >1 year (254, 69.8%), but less than half of them were satisfied with their medications (162, 44.5%). In addition, most patients had better than moderate levels of CGI-S (338, 92.9%) and showed improvement in CGI-I (302, 83.0%).
Primary outcomes
Primary expectation of medication
In the total population, the major choice about the wish for the drug was high efficacy (44.01%±21.44%), followed by low side effects (30.34%±17.84%), low cost (16.09%±13.45%), and small amount (12.94%±13.13%) (Table 2).
Patient’s expectation and preference for medication
The sequence was the same among the psychotic disorders, bipolar disorders, and depressive disorders groups, however, the proportion of “efficacy” was significantly less in patients with depressive disorders (38.81%±18.39%) compared with that in patients with psychotic disorders (50.68%±23.56%) and those with bipolar disorders (47.85%±22.24%). The proportion of “efficacy” of each disease group was significantly different from each other (p<0.001). The proportion of “cost” was significantly less in patients with bipolar disorders (13.44%±13.28%) compared with that in patients with psychotic disorders (17.15%±16.75%) and those with depressive disorders (16.50%±11.17%). The proportion of “cost” of each disease group was significantly different from each other (p<0.05). The proportion of “amount” was significantly high in patients with depressive disorders (15.67%±12.82%) compared with that in patients with psychotic disorders (9.66%±14.37%) and those with bipolar disorders (10.40%±10.18%). The proportion of “amount” of each disease group was significantly different from each other (p<0.001) (Figure 1).
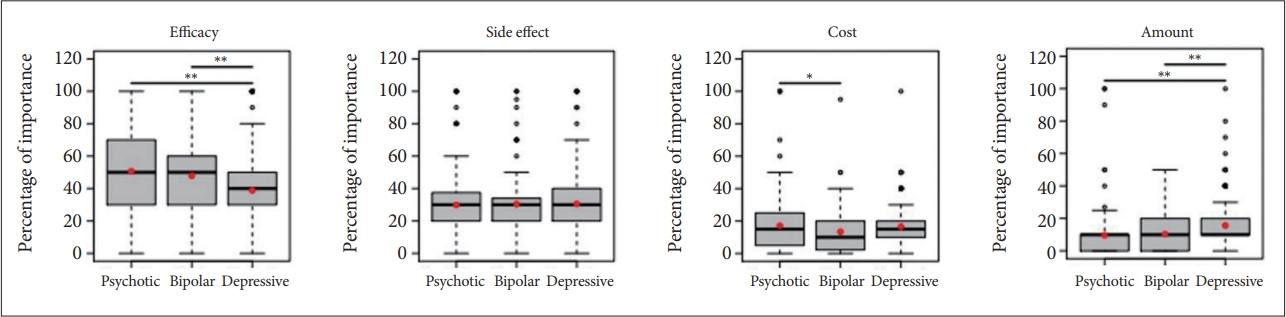
Patients’ primary expectation of medication based on the diagnosis (high efficacy, low side effect, low cost, small amount). *p≤0.05; **p≤0.01.
Main decision maker on deciding drug
In the total population, the major choices of the main decision maker was “patient” (37.39%±22.57%) and “doctor” (35.27%±22.88%), followed by “caregiver” (19.52%±15.69%) and “insurance” (10.87%±11.90%) (Table 2).
This tendency was the same in patients with psychotic disorders and those with depressive disorders; however, patients with bipolar disorders chose “doctor” as their main decisionmaker, and the proportion of “doctor” was relatively high in patients with bipolar disorders (41.61%±26.64%). Each proportion of each choice differed among the three groups (all p<0.05) (Figure 2).
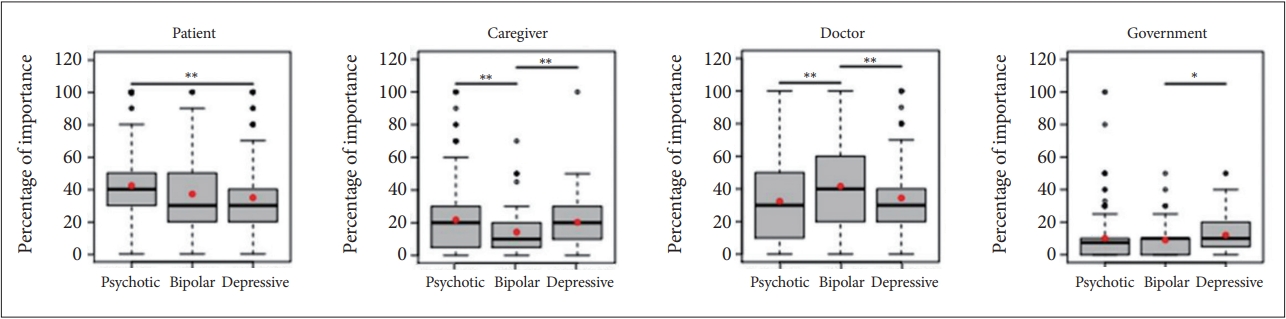
Main decision maker on deciding drug based on the diagnosis (patient, caregiver, doctor, government). *p≤0.05; **p≤0.01.
Preferred type of drug
In the total population, the most preferred type of drug was tablet/capsule (36.16%±30.69%). The second preferred types were extended-release (21.85%±21.36%) and soluble forms (20.91%±22.41%) followed by liquid (9.62%±12.19%), powder (8.06%±10.44%), and injection (7.82%±11.25%) (Table 2).
In all three groups general tablet/capsule was most favorite type of drug. Patients with psychotic disorders (27.27%±29.40%) significantly favored the extended-release form more than patients with bipolar disorders (20.82%±19.27%) and those with depressive disorders (19.30%±15.68%) did. The proportion of “extended-release” of each disease group was significantly different from each other (p<0.001). Surprisingly, proportion of favoring injection was relatively high in the patients with psychotic disorder (8.14%±13.61%) compared with the patients with bipolar disorder (6.99%±10.29%) and those with depressive disorder (7.96%±10.15%) but there was no significant difference between three disease groups (p=0.632) (Figure 3).
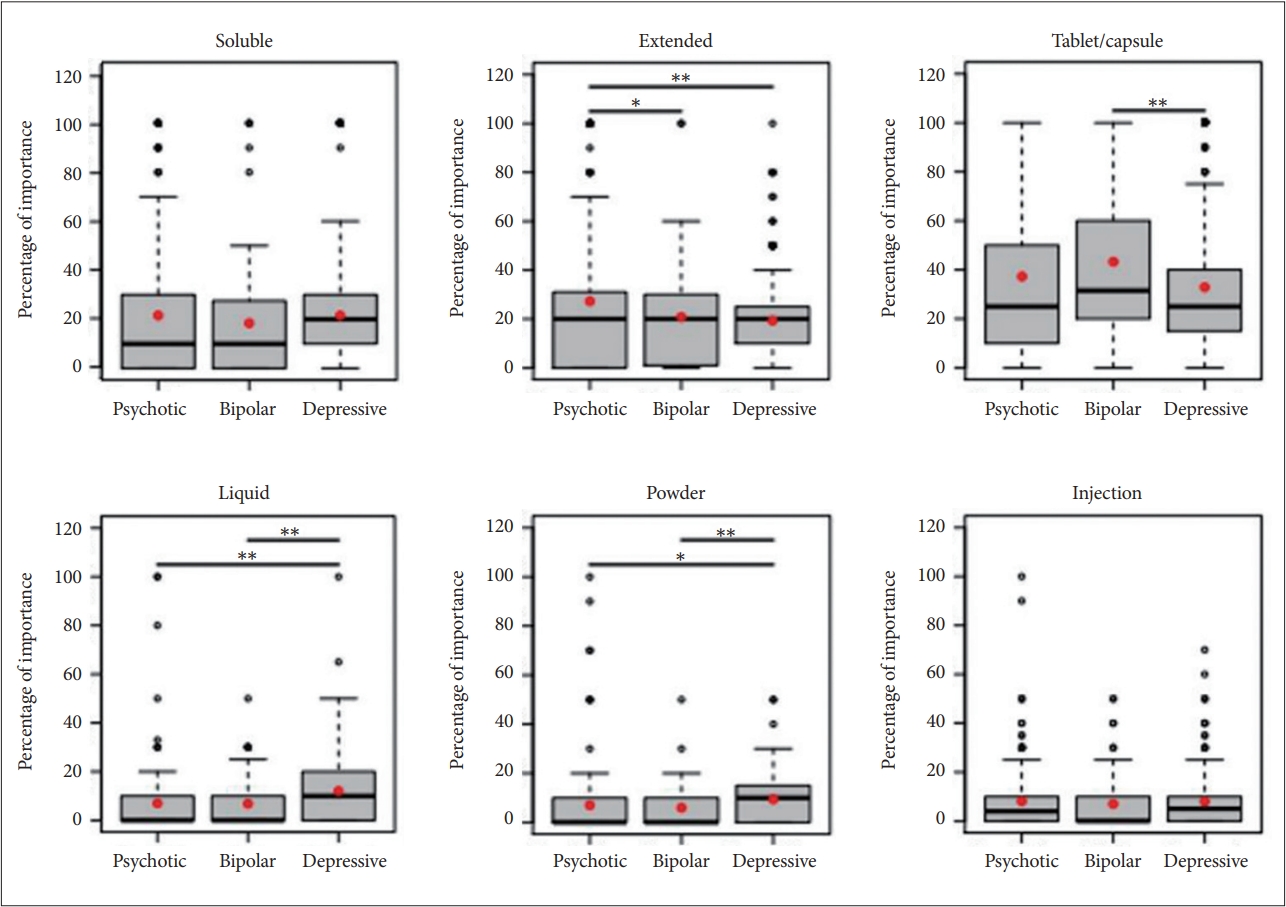
Patients’ preferred type of drug based on the diagnosis (soluble, extended, tablet/capsule, liquid, powder, injection). *p≤0.05; **p≤0.01.
DISCUSSION
This was the first multicentered survey-based study to examine expectations and preferences for medication of patients with depressive disorder, bipolar disorder, or psychotic disorder in Korea. The result of our survey showed that in the total population, patients with major psychiatric illnesses considered high efficacy as the main wish for medication, themselves and a doctor as the main treatment decision makers, and tablet/capsule as the preferred formulation. The preference ratio of high efficacy in the depressive group was significantly lower and the ratio of less amount was significantly higher compared to the psychotic and bipolar groups. Preference ratio of a doctor as the important treatment decision maker in the bipolar group was higher compared to the other disorder groups. Psychotic group had a higher preference rate for extended release drugs compared to other two groups in preferred drug type category. The significant differences between the disorders confirms the importance of this survey in identifying patients’ preferences and values for medication and incorporating them into treatment.
In studies of factors affecting medication adherence, efficacy and side effects are considered to be tied for importance, and in this study, high efficacy was the most desired value by patients, followed by low side effects. The rate of valuing the high effects of drugs was significantly higher in the psychotic disorders and bipolar disorders groups than that in the depression group. According to Achtyes et al. [13], patients with schizophrenia spectrum disorders rated efficacy as the most important factor for using a drug. In the study which explored the views of patients, caregivers, and experts on factors influencing medication adherence in patients with schizophrenia; both patients and caregivers rated efficacy as the most important factor, and prioritized side effects relatively lower over positive drug aspects [14]. Similarly, in a study of depressed type I bipolar patient, the most commonly expressed expectations were a reduction in symptoms and a balanced mood [10]. This shows similar results to our study.
Relatively, compared to the other groups, depressed patients were less likely to value efficacy and significantly more likely to favor fewer pills. Studies have shown that other factors may be more important than simply efficacy in influencing medication adherence in depressed patients [11]. The results of a study by Srimongkon et al. [15], which investigated consumer-related factors that affect antidepressant adherence, treatment efficacy, beliefs, and perceptions about antidepressants, were major influencing factors during the implementation phase of adherence. This study also showed that most participants were motivated to remain adherent when the benefits of the medication outweighed the harm; however, if the negative factors far outweighed the positive factors, patients would consider discontinuing treatment. According to a study by Eisen et al. [16], compliance improved dramatically as the frequency of drug administration decreased. In a study on treatment compliance of antidepressants, Demyttenaere [17] reported that monotherapy generally results in better compliance than polypharmacy and suggested that for antidepressants, a one-day regimen and drugs with a longer half-life are preferable.
Taken together, efficacy and side effects are the main factors that patients value the most from medication, and especially in depressed patients, considering the number of pills or other factors that patients view as positive or negative and applying them to treatment may lead to better outcomes.
As for the main treatment decision making, patients’ opinions were found to be the most important in the overall group with doctors’ opinions almost as important. This is consistent with the finding of other study that patients with mental illness have a desire to be involved in medication and hospitalization decisions and have a higher preference for participation in decision-making compared to patients with general physical illness [18].
However, in the bipolar disorders group, the proportion of doctors’ opinions being important was higher than that of patients. In a study by De Las Cuevas et al. [19] that evaluated the extent to which psychiatric patients’ treatment adherence was affected by the concordance between preferred and actual participation in decision-making, most psychiatric outpatients preferred a collaborative role in decision-making. Self-reported adherence was significantly higher in patients in whom there was concordance between their preferences and their experiences of participation in decision-making, regardless of the type of participation preferred. In a study by Lazary et al. [20] comparing six self-reported variables related to medication adherence in patients with schizophrenia, bipolar disorder, and depression, high doctor locus of control was significantly associated with increased treatment adherence only in the bipolar disorder group, suggesting that the patient-psychiatrist relationship may be particularly relevant to medication adherence in patients with bipolar disorder.
Tablets/capsules were the most preferred formulation in the overall population and were the same within disease groups, likely because they are the most commonly used form. Injectables were the least preferred formulation in the overall population. In a study of schizophrenia patients’ preferences for long-acting injectables and oral antipsychotics by Blackwood et al. [21], the most common reasons cited by patients who preferred pills to injectables were “feeling less embarrassed ”(46%) and “feeling less pain”(18%). Lee et al. [22] found that patients who preferred oral medications to long-acting injectables (LAIs) cited “disliking injections” (32.4%) and “thinking oral medications were sufficient” (43.4%) as reasons for not using LAIs. While these results may explain the low preference for injection, it is possible that the patient’s disease itself had a significant impact on the preference survey, as the “injection” as a treatment formula may be unfamiliar to certain patients for which LAIs are underutilized, which would be a limitation of our study.
This study had several limitations. Firstly, the participants in this study did not include patients from primary care, the results may not represent the entire patient group. Additionally, the survey results may have been influenced by a selection bias since only individuals who voluntarily participated were included. This could potentially introduce a bias towards patients who were more cooperative or had more favorable attitudes towards their doctors and treatment. Moreover, it was challenging to ascertain the characteristics of the patients who refused to participate. Furthermore, the inclusion of certain medication formulations (e.g., injections) as options in a survey about preferred drug types may have biased the results, particularly in patient populations where these formulations are not commonly used. It is important to note that the survey did not utilize a standard questionnaire. Although the constant sum scale method employed in the survey was effective in determining the relative importance of different factors, it may have posed difficulties for patients who have difficulty matching the sum of 100. Lastly, the observed significant differences between disease groups could be attributed to inherent differences in the diseases themselves, introducing a bias in the study. Nevertheless, this study is meaningful in that it is the first multicenter survey-study to identify the expectation for medication, main treatment decision-makers, and preferred drug types in patients with three disorder groups—psychotic disorders, bipolar disorder, and depressive disorder. Our study is particularly significant as the recent rise of personalized medicine and patient-centered care is changing the once one-sided patient–physician relationship to a mutually collaborative way.
Still, there is often disagreement about whether shared decision-making can help improve adherence and treatment effectiveness by ensuring that care reflects patients’ expectations, values, and preferences for care. However, in many cases, their reduced capacity can be compensated for by more intensive educational interventions [23]. If the patient’s preference is matched to the treatment modality, the patient’s satisfaction and treatment adherence will increase, thereby improving treatment participation and consequently alleviating symptoms. Recognizing that patients have a desire to participate in the treatment decision-making process, identifying the most expected elements of medication, the level of shared decision-making participation, and the patient’s preferences for medication formulations, and providing healthcare services accordingly will improve adherence to treatment and lead to better treatment outcomes.
Notes
Availability of Data and Material
The data are not publicly available due to privacy and ethical concerns, but are available from the principal investigator upon reasonable request.
Conflicts of Interest
The authors have no potential conflicts of interest to disclose.
Author Contributions
Conceptualization: Hoo Rim Song. Data curation: all authors. Formal analysis: all authors. Funding acquisition: Hoo Rim Song. Investigation: all authors. Methodology: all authors. Project administration: all authors. Writing—original draft: Seoyun Han, Hoo Rim Song, Minha Hong. Writing—review & editing: Seoyun Han, Hoo Rim Song, Minha Hong.
Funding Statement
This study was supported by the funding from Jisan Cultural Psychiatry Fund of the Korean Neuropsychiatric Association.