Polysomnography and Neuropsychological Analysis of Patients With Post-Traumatic Stress Disorder Two Years After the COVID-19 Pandemic in Wuhan
Article information

Abstract
Objective
We used polysomnography (PSG) monitoring and neuropsychological scales to explore the characteristics of coronavirus disease-2019 (COVID-19) patients diagnosed with post-traumatic stress disorder (PTSD) in Wuhan, two years after the onset of the COVID-19 pandemic.
Methods
A total of 42 patients in the Sleep Medicine Center were diagnosed with insomnia between December 2021 and May 2022; they were divided into the PTSD group (patients with PTSD diagnosed with insomnia after COVID-19 infection) and the non-PTSD group (patients with insomnia without PTSD). A healthy control group was simultaneously included.
Results
The PTSD group was more significant than the non-PTSD group in partial manifestations of sleep disorders, neuropsychological clinical symptoms, and partial PSG data. Patients with different COVID-19 subtypes showed significant differences in the course of disease, sleep disorders, neuropsychological clinical symptoms, relevant scale scores, and PSG data analysis.
Conclusion
The emotional anxiety and depression of COVID-19 patients diagnosed with PTSD two years after the COVID-19 pandemic in Wuhan are more significant, and will not be self-alleviated with the passage of time. It is necessary to continue to pay attention to the PTSD symptoms and sleep psychology of COVID-19 infected patients, and take appropriate measures. Patients with severe and critical COVID-19 have more severe sleep and mental disorders, and there is a significant correlation between the duration of the disease and the severity of mental and mental disorders and sleep disorders after recovery.
INTRODUCTION
The novel coronavirus disease-2019 (COVID-19)—transmitted by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)—was discovered in December 2019. The disease occurred suddenly, spread rapidly, and had a wide range of influence. The World Health Organization (WHO) declared it a public health emergency of international concern [1], and studies have demonstrated that this public health emergency has had a significant impact on society’s psychology. Patients with COVID-19 experience both negative emotions (such as anxiety, nervous fear, anger, complaint, guilt, depression, and despair) and physical symptoms (such as insomnia, palpitations, dyspnea, fatigue, and sweating) [2,3]; however, these symptoms do not only exist during the period of COVID-19 infection. With the increasing number of patients recovering from COVID-19, the mental health and sleep problems of these patients are becoming increasingly prominent. Some foreign studies refer to these symptoms as postacute COVID-19; this syndrome is characterized by persistent symptoms and/or delayed or long-term complications, similar to postacute viral syndromes described in survivors of other virulent coronavirus epidemics [4]. Post-traumatic stress disorder (PTSD) refers to the delayed emergence and long-term persistence of individuals after sudden, threatening, or catastrophic events. The core symptoms of PTSD include traumatic experience symptoms (after traumatic events, traumatic event-related intrusive symptoms occur), continuing to avoid stimulation, and traumatic events related to a traumatic event related to negative changes in cognition and mood began or worsen after a traumatic event occurs, and traumatic events related to alert or reactive significant change [5].
At present, it has been more than two years since the outbreak of the new crown epidemic in Wuhan of December 2019. Many patients still exhibit symptoms such as fear, dreams, nightmares, nervousness, and fear related to the epidemic; therefore, PTSD related to the epidemic should be identified and remain a focal point. Previous studies have also shown that sleep disorders are closely related to PTSD, anxiety, and depression [6-8]. Sleep disorder is one of the most common symptoms of PTSD [9]. There is a high degree of overlap between the symptoms of sleep disorder and PTSD [10], which seriously affects health and quality of life. Additionally, studies have shown that COVID-19 has pathological effects on multiple organs and tissues, including the brain and nervous system, including acute psychiatric symptoms in patients with COVID-19. Neuropsychological effects may persist from primary COVID-19 infection to recovery, but symptoms usually improve over time [11]. Still, the evaluation of sleep disorders in previous studies was mostly based on subjective evaluations—such as sleep diaries and questionnaires—and there was a lack of objective data from sample studies (laboratory PSG and home actigraphy) [12]. Based on this, we evaluated the sleep and neuropsychological changes of patients who recovered from COVID-19 in Wuhan two years after the epidemic using various tools and assessments. We hypothesized that the psychological and sleep changes of patients who recovered after the new crown epidemic are related.
METHODS
In this study, 42 patients diagnosed with insomnia who were admitted to the Sleep Medicine Center of Wuhan First Hospital between December 2021 and May 2022 were reviewed; they were divided into PTSD (patients with PTSD diagnosed with insomnia after COVID-19 infection) and non-PTSD (patients with insomnia not infected with new coronary pneumonia) groups; 21 healthy controls were also included. To understand the sleep and neuropsychological conditions of patients infected with COVID-19 with PTSD in Wuhan two years after the epidemic, the sleep polysomnography (PSG) monitoring and sleep neuropsychological scales were evaluated. The trial was conducted in accordance with the guiding principles of the Declaration of Helsinki, and was approved by the Ethics Committee of Wuhan First Hospital (ethics number: W202005). All patients provided written informed consent.
Inclusion criteria for the PTSD group
All enrolled patients met the diagnostic criteria for PTSD in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) [5], and were confirmed to be infected with COVID-19 during the epidemic. The source of trauma was COVID-19, and they did not suffer any major mental or psychological stimulation, or traumatic event, in the past. Patients were required to cooperate to complete the neuropsychological tests and PSG monitoring; have been clinically cured of COVID-19, have no clinical symptoms related to COVID-19, and had negative nucleic acid test results.
Inclusion criteria for the non-PTSD group
All enrolled patients met the diagnostic criteria for insomnia in the International Classification of Sleep Disorders, Third Edition (ICSD-3) [13], and were not infected with COVID-19 (negative nucleic acid screening results during hospitalization). Additionally, they did not experience previous major mental or psychological stimulation, or major traumatic events; i.e., they did not meet the diagnostic criteria for PTSD in the DSM-5. Last, they could cooperate with the neuropsychological tests and PSG monitoring.
Inclusion criteria for the healthy control group
All enrolled patients were 20–70 years old, not infected with new coronavirus pneumonia, and had negative nucleic acid screening results. No major mental or psychological stimulation, or major traumatic events occurred in the past, and all patients could cooperate with the completion of the neuropsychological tests and PSG monitoring. Additionally, they had no previous sleep, neuropsychological, or related disorders, and did not experience sleep deprivation or take sleep-disrupting medications two weeks prior to the test.
Exclusion criteria for the PTSD and non-PTSD groups
The exclusion criteria included a history of neuropsychiatric disorders; current or past history of other secondary mental disorders; received formal psychotherapy or psychiatric drug treatment; past dependence on psychoactive substances (except nicotine), such as alcohol, coffee, and social drinking; other major physical diseases; and in pregnancy.
Routine laboratory tests
Sixty-three patients underwent physical examination, head magnetic resonance imaging examination, electroencephalogram (EEG), blood analysis, urine analysis, stool examination, liver and kidney function, electrolyte, blood lipid, blood glucose, electrocardiogram, and other related examinations to assist with diagnosis and screen for other possible etiologies. Nucleic acid, novel coronavirus antibody, and chest computed tomography (CT) data were reviewed.
Polysomnography
All 63 patients were treated with PSG (Grael series; Compumedics Limited, Victoria, Australia). Data were collected in accordance with the montage derivation combination of international standards, including reference derivation (EEG, electrooculogram [EOG], chin electromyography [chinEMG]), bipolar derivation (electroencephalogram [ECG], thermal flow, thorax and abdominal sensors, right and left anterior tibial EMG), and direct current lead (nasal pressure, SpO2); the international 10–20 positioning system was used to determine the position of the head electrode. The recommended EEG derivations were F4-M1, C4-M1, and O2-M1; the recommended EOG derivations were E1-M2 and E2-M2; and the recommended chinEMG derivations were chin1, chin2, and chinz (reference electrode). This was referred to in the American Academy of Sleep Medicine (AASM 2.6) [14] for respective acceptable and backup electrode derivation; backup derivation was recommended to provide redundancy in case of electrode malfunction. The ECG used lead II, the limbEMG recorded the muscle activity of the left and right anterior tibia, the blood oxygen saturation used pulse oxygen monitoring, and the respiratory-related signals used nasal pressure, thermal flow, respiratory inductance plethysmography (recording respiratory effort), etc. The monitoring process followed the provisions of the standard PSG process in the AASM 2.6; PSG data were collected in accordance with the 6-step method, including collecting, amplifying, converting, storing, analyzing, and displaying the data. None of the enrolled patients underwent PSG on the first night after admission, to avoid the influence of the “first-night effect” on monitoring results. During the monitoring period, we ensured that the environment was quiet, and the room temperature was appropriate. When the patient was drowsy, they turned off the light to fall asleep (no later than 23:00), and turned on the light when the patient woke up in the morning (no later than 07:00). Prior to monitoring, the patient filled out a consent form regarding PSG, as simultaneous video and audio recordings were taken in the monitoring room. During the monitoring process, technicians and medical staff were on duty all night to ensure that relevant measures were in place for any technical or medical problems that may arise. During data analysis, professional, PSG-registered technicians interpreted the data and issued relevant reports according to The AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications, Version 2.6 [14]. The physiological parameters analyzed in this study included: sleep latency (SL, the time from turning off the light to recording the first sleep stages); the number of wakefulness (NW, the number of awakenings from falling asleep to the end of sleep); wakefulness after sleep onset (WASO, the total waking time from falling asleep to the end of sleep); sleep efficiency (SE, the percentage value between the total sleep time [TST] and total bed time during monitoring); and the proportion of sleep stages non-rapid eye movement sleep stages 1–3, and rapid eye movement (REM) sleep in total sleep (N1%, N2%, N3%, R%).
Assessment methods of neuropsychology and sleepiness scales
Forty-two patients from our department underwent mental evaluation division in scale measurement. For the Pittsburgh Sleep Quality Index scale (PSQI), the total score of the scale was 21 points; the lower the score, the better the sleep quality of the patient [15]. The PTSD Checklist–Civilian Version (PCL-C) [16], comprises 17 items—including intrusion symptoms, avoidance symptoms, negative alterations in cognitions and mood, and alterations in arousal and reactivity—to assess the three main symptoms of PTSD. The PCL-C scale requires subjects to make an independent assessment based on their personal situation in the previous month. The 5-level scoring standard was adopted, and the total score for each item is added to judge the presence of PTSD; the higher the total scores on the scale, the greater the likelihood of PTSD. A score of 17–37 indicated no obvious symptoms of PTSD; a score of 38–49 indicated some degree of PTSD; and a score of 50–85 indicated significant symptoms of PTSD. The Insomnia Severity Index (ISI) [17] can assess the severity of insomnia in subjects and subjectively evaluate their insomnia symptoms over the previous two weeks. The scale is simple, convenient, and reliable for the evaluation of insomnia symptoms in different ages and groups; the higher the score, the more serious the degree of insomnia. The Epworth Sleepiness Scale (ESS) is a self-rating scale used to assess the severity of sleepiness in subjects; a score ≥10 is classified as excessive sleepiness [18,19]. Seventeen versions of the Hamilton Depression Scale (HAMD) [20] were used to evaluate the degree of patients’ depression, while the Hamilton Anxiety Scale (HAMA) [21] was used to evaluate the degree of patients’ anxiety. The aforementioned two scales included 14 items, and a 5-level scoring method was adopted; a HAMD score <8 was classified as no depression, ≥8 as mild depression, ≥17 as moderate depression, and ≥24 as severe depression. A HAMA score <6 was classified as no anxiety, ≥7 was classified as mild anxiety, ≥14 was classified as moderate anxiety, ≥21 was classified as severe anxiety, ≥29 was classified as severe anxiety. The depression self-assessment scale (Patient Health Questionnaire, PHQ-9) [22] is widely recognized globally, and is mainly used to screen for and identify depressive symptoms. It was used to evaluate the depression status of subjects over the previous two weeks; the higher the total scores on the 9-item questionnaire, the greater the likelihood of positively screening depressive symptoms. A score ≤4 indicated no depressive symptoms; 5–9 indicated mild depressive symptoms; 10–14 indicated moderate depressive symptoms; 15–19 indicated moderate to severe depressive symptoms; and 20–27 indicated severe depressive symptoms. The Self-Rating Anxiety Scale (SAS) [23] used to assess the subjective severity of anxiety in subjects. There were 20 items in this scale, including 15 forward scores and five reverse scores, each scored at four levels. The cumulative scores of each item resulted in a rough total score, which was multiplied by 1.25 to get the standard total score. A total score <50 indicated no anxiety, 50–59 indicated mild anxiety, 60–69 indicated moderate anxiety, and ≥70 indicated severe anxiety; the higher the score, the more serious the anxiety.
Statistical methods
Baseline characteristics between the PTSD and non-PTSD groups, as well as the neuropsychological scores, sleepiness scale, and PSG monitoring results of patients with different types of pneumonia, were analyzed using the χ2 test. The count data were displayed by rate (%), and measured data with normal distribution was expressed as mean±standard deviation. Comparisons between two groups were performed using the t-test for two independent samples, and comparisons between multiple groups were performed using one-way analysis of variance; post-hoc t-tests were used after one-way analysis of variance. If the measurement data exhibited non-normal distribution, the median (interquartile range) was used. The Mann–Whitney U test was used for analysis between two groups, and the Kruskal–Wallis rank sum test was used for analysis between multiple groups. Between multiple sets of pairwise comparisons using the Bonferroni method for correction, an adjusted p<0.05 was considered statistically significant. Spearman’s correlation analysis was used to investigate the correlation between the duration of disease, and neuropsychological scales, the sleepiness scale, and PSG. A two-sided p<0.05 was considered statistically significant, and all analyses were performed using SAS 9.4 (SAS Institute, Cary, NC, USA).
RESULTS
Basic information and general examination results of patients in the two groups
There was no statistical significance regarding gender, age, or education level between the three groups (non-PTSD vs. healthy control group, PTSD vs. healthy control group, and PTSD vs. non-PTSD group; p-values were all >0.05), and the data were comparable (Table 1).

Baseline characteristics of three groups
Basic information regarding COVID-19 infection in patients with PTSD
There were 21 patients in the PTSD group; 19 (90.48%) had fever, 15 (71.43%) had cough, and individual patients had headache, fatigue, eye distension, diarrhea, palpation, panting, and other atypical manifestations. All 21 patients were diagnosed via complete imaging examination (lung CT); there were five cases of mild pneumonia (23.81%), 10 cases of moderate pneumonia (47.62%), one case of severe pneumonia (4.76%), and five cases of critical pneumonia (23.81%) [24]. In the COVID-19 infection stage, 17 patients (80.95%) were found to be positive via the nucleic acid test; 21 patients (100.00%) were positive for IgG antibodies, among which 11 patients (52.38%) were positive for IgM antibody. During the study period, all patients were negative for COVID-19 via nucleic acid testing (Table 2, Supplementary Material and Supplementary Table 1 in the online-only Data Supplement).

Basic information of patients with COVID-19 in PTSD group (N=21)
Compared with the non-PTSD group, the wake up at night, nightmares/multiple dreams increased in the PTSD group (p<0.05). Regarding neuropsychological manifestations, the PTSD group exhibited more significant rates of nervousness, anxiety, fear, phobia epidemic, panic attack/flashback, other dzsymptoms (depression, world weariness, hallucination), and other manifestations than the non-PTSD group (p<0.05) (Table 3).

Sleep status, emotional performance of patients in the PTSD group and non-PTSD group (N=42)
Relationship regarding neuropsychological scale, sleepiness scale, and PSG data between the three groups
The researchers analyzed subjects’ neuropsychological scale, sleepiness scale, PSG, and other data. Regarding the sleep scale, there were significant statistical differences observed in the PSQI scores between the three groups (p, p*, p**, and p***-values were all <0.05); there were no significant differences in ISI and ESS scores between the PTSD and nonPTSD groups (p***>0.05). Concerning the neuropsychological scale, significant differences were observed in the PCL-C, HAMD, HAMA, PHQ-9, and SAS scores between the three groups (p, p*, p**, and p***-values were all <0.05); there was no significant difference in the SAS scale score between the non-PTSD and healthy control groups (p*>0.05). PSG data analysis revealed significant differences between three groups regarding SE, WASO, N1%, N3%, and R% (p, p*, p**, p***<0.01). The WASO, N1%, N2%, N3% were significantly different (p***<0.05) in the PTSD group when compared with the non-PTSD group. Compared with the healthy control group, the TST, SE, SL, WASO, N1%, N2%, N3% were significantly different (p**<0.05) in the PTSD group. The TST, SE and disorder of the sleep structure was more significant in the PTSD group (Table 4).

The relationship between the neuropsychological scale, sleep scale, and PSG data of the three groups of patients
Relationship between COVID-19 classification and sleep status, emotional performance, and PSG data in the PTSD group
In this study, patients in the PTSD group were divided into three subgroups according to the new coronary pneumonia classification, including 5, 10, and 6 patients with mild, moderate, and severe or critical severity, respectively. There were significant differences regarding the duration of disease, neuropsychological scale (HAMA, HAMD, PCL-C, PHQ-9, SAS), sleepiness scale (PSQI, ISI, ESS), sleep structure (N1%, N2%, N3%, R%), WASO, and NW among the three groups (p<0.05). There were no significant differences regarding the total recording time, TST, SE, and SL between the three groups (p> 0.05), indicating that there was no significant correlation between the severity of pneumonia in the PTSD group, and the changes in total recording time, TST, SE, and SL during PSG (Table 5).
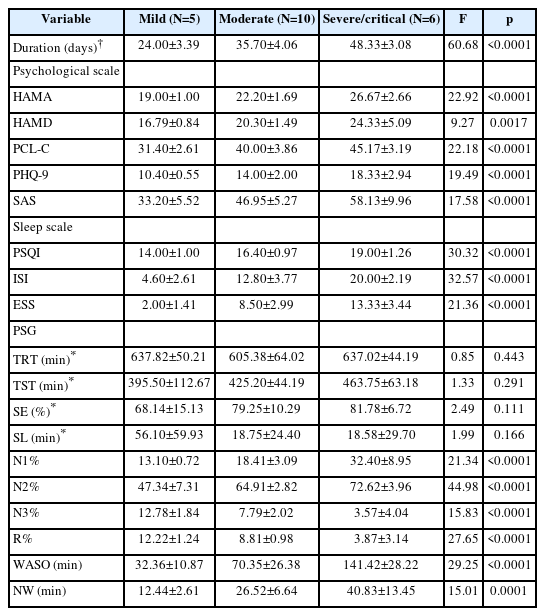
The relationship between COVID-19 classifications and sleep and neuropsychology in PTSD group (N=21)
Comparisons were made between the three groups regarding the neuropsychological scale, sleepiness scale, sleep structure, WASO, NW, and other aspects; the p-values were all <0.05, indicating that the differences between groups were statistically significant. We found that the more severe the COVID-19 classification, the longer the course of disease, the higher the neuropsychological scale (HAMA, HAMD, PCL-C, PHQ-9, SAS) and insomnia scale (PSQI, ISI, ESS) scores, the more obvious the degree of sleep structure disorder, and the greater the waking time and frequency of PSG at night (Table 6).

Relationship between sleep and neuropsychology among patients with different COVID-19 types (N=21)
Relationship between the duration of COVID-19 and psychiatric disorders, sleep disorders, and PSG data in the PTSD group
Spearman’s correlation coefficient was used to analyze the correlation between the duration of COVID-19 in the PTSD group, and the neuropsychological scale, sleepiness scale, and PSG data; all p-values were <0.05, indicating a clear correlation between the data. In the PTSD group, the duration of COVID-19 positively correlated with HAMA, HAMD, PCL-C, PHQ-9, and SAS scale scores (all positive r-values), indicating that the longer the duration of COVID-19, the higher the neuropsychological scale score; the SAS scale exhibited the strongest correlation with duration length (|r|=0.84). The duration of COVID-19 positively correlated with the PSQI, ISI, and ESS scores (r-values were all positive), indicating that the longer the duration of COVID-19, the higher the sleep disorder scale score; the ISI scale exhibited the strongest correlation with duration length (|r|=0.91). The duration of COVID-19 positively correlated with N1%, N2%, WASO, and NW during PSG (r-values were all positive), indicating that the longer the disease duration, the greater the N1% or N2% ratio, and the greater the WASO and NW. Conversely, the duration of COVID-19 negatively correlated with N3% and R% (r-values were negative), indicating that the longer the duration of COVID-19, the smaller the proportion of N3% and R%; the R% ratio (|r|=0.92) and WASO (|r|=0.93) were most strongly associated with the duration of COVID-19 (Tables 7 and 8).


DISCUSSION
Regarding sleep disorders in patients with COVID-19 diagnosed with PTSD in Wuhan, the wakefulness index, SL, and WASO increased significantly, while the TST and SE decreased significantly, two years after the pandemic when compared with the healthy control and non-PTSD groups. Patients with COVID-19 diagnosed with PTSD were more likely to experience multiple dreams or nightmares at night. Nocturnal nightmares are an important core symptom of PTSD, and patients often repeatedly experience previous traumatic events in dreams, often dreaming about people or things related to these traumatic events [25]. Regarding sleep structure, the proportion of N1% and N2% significantly increased in patients with COVID-19 diagnosed with PTSD, while the proportion of N3% and R% significantly decreased, indicating a significant disturbance in sleep structure. Patients with PTSD also had sleep disorders characterized by decreased TST, slow-wave sleep, and SE, and increased WASO. High PTSD severity was associated with a decreased SE and percentage of slow-wave sleep. Moreover, the percentage of REM sleep in patients with PTSD was significantly lower than in patients without PTSD in a previous study [25], which was consistent with the results of our study and was considered to be associated with intrusive symptoms in patients with PTSD. “Intrusive symptoms” refers to the repeated experience of traumatic events during sleep (including flashbacks, full or partial recurrence of events in dreams) [3]; this leads to repeated interruptions of REM sleep, a decrease in REM ratio, and deep memory of dream contents. Additionally, big data studies have demonstrated associations between COVID-19 and dream recall frequency (DRF), and related social, health, and mental health factors. This resulted in an increase in reports of high DRF during the COVID-19 pandemic, as people who have experienced major trauma tend to have disturbing and repetitive trauma-related dreams [26].
Regarding mental psychology, patients with COVID-19 diagnosed with PTSD were found to be prone to anxiety and depression. Studies have shown that patients diagnosed with COVID-19 face great psychological pressure, and symptoms of depression and anxiety were observed to be moderate [27]. The pain tolerance of patients with COVID-19 significantly correlated with the clinical level of symptoms for depression, anxiety, and PTSD [28]. Sample data from Ireland revealed that COVID-19-related PTSD was also associated with high rates of generalized anxiety disorder (49.5%) and depression (53.8%) [29].
The severity of COVID-19 infection during the epidemic correlates with the severity of anxiety, depression, and sleep disorders after recovery. The more severe the degree of infection in patients with COVID-19, the more significant their psychological, sleep, and sleep structure disorders. The severity of COVID-19 infection has been highlighted as a risk factor for PTSD, with two studies reporting that patients discharged from intensive care units are more likely to develop PTSD than non-intensive care unit patients [11]. A big data study in Greece [30] revealed that 37.6% of participants were found to have sleep problems during the COVID-19 pandemic; additionally, COVID-19-related anxiety, loneliness, and depressive symptoms were found to be significantly associated with the incidence of insomnia.
The duration of COVID-19 infection correlated with the severity of mental, psychological, and sleep disorders after recovery; the longer the course of COVID-19 infection, the more significant the manifestations of mental and psychological disorders, sleep disorders, and sleep structure disorders. After the COVID-19 pandemic, the incidence of sleep disorders, generalized anxiety, and other disorders remained high over time. One study evaluated 81 patients at 3 months and 1 year after COVID-19, and 18% of patients had significant cognitive deficits. Symptoms of depression, anxiety, and PTSD occurred in 6%, 29%, and 10% of patients, respectively, 1 year after infection. These mental and cognitive impairments were not improved after 3 months of follow-up and were relieved to varying degrees after 1 year [31]. Thus, clinicians should be aware of postpandemic depression, anxiety, fatigue, sleep disorders, PTSD, and the possibility of rare neuropsychiatric syndromes. Additionally, public awareness of the need for psychological interventions to address the short- and long-term psychopathological effects of the COVID-19 pandemic is necessary [32,33]. Some studies have pointed out that sleep disorders in patients with PTSD are caused by the characteristics of PTSD symptoms, and their sleep disorders affect the progression of PTSD in many ways. Aggravating the degree of both will form a vicious cycle of the condition and seriously affect the prognosis of patients, indicating that PTSD and sleep disorders are closely related and mutually influenced. Other studies have shown that difficulty falling asleep and sleep deprivation caused by nightmares can worsen PTSD symptoms [34]. The performances and scores observed in this study were inconsistent with other research, as PSG itself requires patients to complete monitoring throughout the night; this takes a long time and causes poor comfort, leading to poor patient compliance and unsatisfactory data. Patients also tend to be in a state of anxiety and depression, and their compliance with examinations and enthusiasm for inclusion were not high, leading to the small sample size of this study. Additionally, the short duration of disease and lack of research centers also played an important role.
This study focused on sleep and neuropsychological performance without biological indicators—such as the expression of genes [35,36], inflammatory proteins (interleukin 1β [IL-1β] and c-reactive protein), and neurotransmitters (glucocorticoid receptor, neurosteroid biosynthesis, GABAA receptor subunit)—in patients with COVID-19 [37]. Moreover, as an international public health event, the COVID-19 pandemic had a significant impact on all levels of society; the disease impact was not limited to patients with COVID-19, and ordinary people, medical workers, and epidemic areas of people from all over the world were affected. The types of changes that occur in during sleep, neuropsychology, and how to effectively intervene, are also worthy of further study. In addition, the factors affecting PTSD are not comprehensively considered, and this paper only discusses the symptoms of PTSD after COVID-19 infection. There are many stress factors of PTSD, such as growing experience and personality factors, which have not been discussed.
In conclusion, two years after the COVID-19 pandemic in Wuhan, patients with COVID-19 diagnosed with PTSD exhibited decreased SE, delayed SL, increased WASO, increased incidence of nocturnal polysomnosis and nightmares, and disturbed sleep structure (with a decreased rate of deep sleep and increased rate of light sleep) when compared with patients with general insomnia. Additionally, patients with COVID-19 diagnosed with PTSD exhibited significantly higher levels of emotional anxiety and depression than those with general insomnia; this was not relieved over time, suggesting that we need to pay continuous attention to PTSD and sleep psychology in patients infected with COVID-19. Compared with patients with mild and moderate COVID-19, patients with severe or critical COVID-19 exhibited more severe sleep and neuropsychological disorders. Last, we observed a significant correlation between the duration of COVID-19 infection and the severity of mental disorders and sleep disorders after recovery. These provide references for the timely prevention and treatment of PTSD.
Supplementary Materials
The online-only Data Supplement is available with this article athttps://doi.org/10.30773/pi.2023.0095.
Questionnaire for patients with sleep and mood disorders
Time information of enrolled patients
Notes
Availability of Data and Material
The data that support the findings of this study are available from the corresponding author, Qing Yang, upon reasonable request.
Conflicts of Interest
The authors have no potential conflicts of interest to disclose.
Author Contributions
Conceptualization: Yilong Wang, Qing Yang. Data curation: Weiqi Chen, Yicong Wang. Formal analysis: Weiqi Chen, Yicong Wang. Funding acquisition: Xue Gong, Jinmei Xu, Guohua Chen, Zhaohong Kong, Yilong Wang. Investigation: Yanjie Xu, Junhua Mei, Qing Yang, Yicong Wang. Methodology: Yanjie Xu, Junhua Mei, Qing Yang, Yicong Wang. Resources: Yanjie Xu, Junhua Mei, Qing Yang, Yicong Wang. Supervision: Yanjie Xu, Junhua Mei, Qing Yang, Yicong Wang. Validation: Yanjie Xu, Junhua Mei, Qing Yang, Yicong Wang. Writing—original draft: Junhua Mei, Yanjie Xu, Qing Yang. Writing—review & editing: Junhua Mei, Yanjie Xu, Qing Yang.
Funding Statement
This study was funded by Special grant of Prevention and Control of COVID-19 Epidemic of Wuhan Municipal Health Commission (EX20M03) and Hubei Province Traditional Chinese medicine research project (ZY2023F057).
Acknowledgements
We gratefully acknowledge all hospitals participating in the study and thank all enrolled participants and their relatives.