Increased Long-Term Risk of Dementia in Patients With Carbon Monoxide Poisoning: A Systematic Review and Meta-Analysis of Cohort Studies
Article information

Abstract
Objective
To assess whether carbon monoxide (CO) poisoning increases the incidence of dementia.
Methods
We searched the Cochrane Library, PubMed, and EMBASE from inception to 14 August 2022. Two authors independently selected studies, assessed the quality of included studies, and extracted data. Any disagreement was resolved by discussion with a third author. Only cohort study with an enough follow-up period was included for systematic reviews and meta-analysis.
Results
Thirty-three full texts were initially searched, but only three studies met our inclusion criteria, and they were comprised of 134,563 participants who were initially free of dementia. The follow-up period ranged from 9 to 12 years. We found that CO poisoning increased the risk of dementia incidence (adjusted hazard ratio 2.61, 95% confidence interval 1.56 to 4.36, p=0.0003). Subgroup analysis showed that the increased dementia risk was significant in males but not in females, and the highest risk was in young age group, followed by in middle age group, but not in the old one.
Conclusion
Overall the evidence from prospective cohort studies supported a link between CO exposure and an increased dementia risk, although all the included studies were limited to Taiwanese population.
INTRODUCTION
Dementia is a kind of brain diseases that is characterized by a long-term and progressive loss of cognitive functioning. It is severe enough to affect a person’s daily life and activities such as the ability to think, remember and reason. Dementia has been thought the 5th common chronic disease by Global Burden of Disease Study [1]. As the global population ages, dementia prevalence is expected to rise substantially over the next several decades, especially in low- to middle-income countries. Up to 2017, there are about 260,000 people suffering from dementia in Taiwan. Although we are not well known the etiology of dementia, the existing report showed that it seemed to have relation with advanced age, female sex, genetic factors, and some potentially modifiable, acquired and environmental risk factors [2-8].
Carbon monoxide (CO) at low concentrations is a colorless, tasteless, odorless gas. CO formation is generally caused by incomplete combustion of carbon compounds. CO binds to hemoglobin (Hb) in the blood with approximately 240 times the affinity of oxygen, forming carboxyhemoglobin (COHb) and resulting in impaired oxygen transport and utilization. CO poisoning will cause several kinds of neurological symptoms, headache, weakness, dizziness, nausea, and vomiting [9]. It could even develop unconsciousness, respiratory arrest, and even death [10]. In addition, about 30% of CO poisoning patients would exhibit chronic neuropsychiatric symptoms several months later, such as mental deterioration, gait disturbance, incontinence, mutism, and Parkinsonism [11]. Several studies have reported that CO poisoning increased the risk of dementia [12-14]. It is estimated that the cumulative incidence rate and mortality of CO poisoning worldwide are 137 and 4.6 cases per million person-years in 2017, respectively [15]. In Taiwan, the mortality rate of unintentional CO poisoning continued to rise from 1.6 to 3.5 per million person-years during the period 1997–2003, and the most common events of CO poisoning are using heating appliances in enclosed space or suicide [16]. Furthermore, the incidence of intentional CO poisoning including suicide by charcoal burning has also increased [17].
In this study, we performed a systematic literature review and meta-analysis of cohort studies to assess the long-term risk of dementia, Alzheimer’s disease, and cognitive disorder in people with experience of CO poisoning.
METHODS
Literature search
We conducted and reported this study according to MOOSE (Meta-analysis Of Observational Studies in Epidemiology) guidelines [18]. The search was carried out without language restriction on the electronic databases Cochrane, PubMed, and EMBASE up to 14 August 2022. The search strategy contained two components: 1) Charcoal-burning OR Carbon monoxide poisoning OR Carbaxyhemoglobinemia OR Carboxyhemoglobin OR Charcoal-burning suicide, and 2) Neurodegenerative Disease OR Alzheimer OR Dementia OR Cognitive Decline OR Chronic traumatic encephalopathy. These components were combined using the Boolean “AND” operator to obtain any link between them. The search strategy was modified when searching other databases. No hand-searching was worked.
Study selection
Studies were included for meta-analysis if they met the following criteria: 1) cohort study design was used, 2) the exposure was CO poisoning, 3) the end point was incidence of dementia, Alzheimer, and cognitive disorder, 4) the study reported quantitative estimates of hazard ratio (HR), or relative risk with 95% confidence intervals (CIs) or sufficient data for determination for dementia related to CO poisoning, and 5) the cohort had an adequate follow-up interval. We excluded cross-sectional or case-control studies, as well as conference abstracts that provided limited information. We screened the relevant studies using their titles and abstracts first and scrutinized the full text to determine whether information was potentially related finally. Two of the investigators (H-S W and ZL J) independently identified eligible studies and reviewed all relevant articles, with confusion resolved by discussion with a third author.
Data extraction and quality assessment
The following information was extracted from each study using a standardized data-extraction form: the first author’s name, year of publication, country, study design, study duration, participants’ characteristics, sample size, database, and risk estimates. Two authors (H-S W and ZL J) independently performed the quality assessment of included studies using the Newcastle-Ottawa Scale (NOS) for cohort studies [19]. The scale assesses aspects regarding population/sampling methods, exposure/outcome collections, as well as statistical matching/adjustments of the data. A maximum of nine quality scores were assigned for each study. Studies with seven or more scores were awarded high quality [18]. Discrepancies were resolved by the third investigator.
Statistical analysis
We synthesized all available association estimates between exposure to CO poisoning and risk of dementia in Review Manager version 5.3 (The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen, Denmark). The estimate risk of outcome as HRs and 95% CIs were pooled under a random-effects model because of considerable clinical heterogeneity. We assessed heterogeneity using the I2 statistic, which evaluates the degree of variation across studies that is due to heterogeneity rather than chance alone. An I2 value of ≥50% indicates substantial heterogeneity [20,21].
RESULTS
Results of literature search
A total of 218 unique citations were identified by our search strategy (137 from PubMed, 106 from Embase, and 11 from the Cochrane Library, with 36 duplicates), of which 33 were accepted for full text review after screening by titles and abstracts. From the remaining 33 articles, we excluded papers with irrelevant content (n=9), different outcome (n=7), case report (n=11), animal experiment (n=2), and conference abstracts (n=1). Ultimately, three articles were eligible and included in our meta-analysis [12-14], and two studies have the stratified data [13,14]. A detailed screening flow is shown in Figure 1.
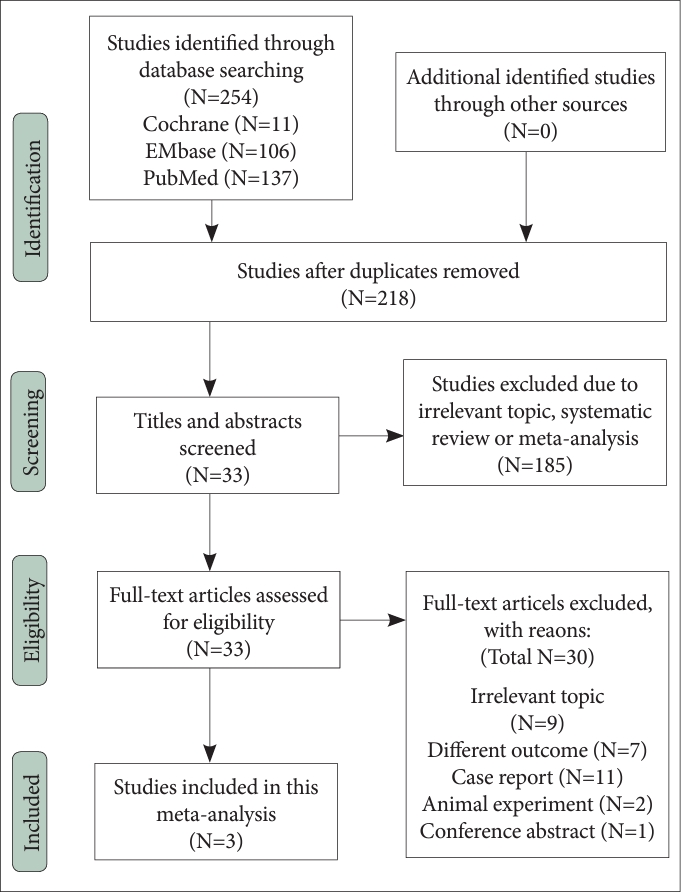
PRISMA flow diagram of study search and selection.
Study characteristics
The primary characteristics of the included studies are summarized in Table 1. These studies were published between 2016 and 2018, based on the National Health Insurance Research Database in Taiwan. All three cohort studies included both sexes and similar age ranges. The sample size in the exposure group of each study was 4,103; 9,041; and 14,590, respectively. Overall, 27,734 adults with CO poisoning as exposure groups and 106,829 controls were included in this meta-analysis. They recruited incident patients with newly diagnosed CO poisoning or charcoal-burning suicide attempts at baseline, except one study using prevalent patients with CO poisoning. All controls were non-CO poisoning, two studies were designed as individual matched for sex, age, and index year in a ratio of 1:4 or 1:3, and the other is frequency-matched. Reporting of follow-up varied between studies and length ranged from 9 to 12 years. As shown in Table 1, various sets of diagnostic codes were used for outcome measurement. The adjusted effect estimates (HRs) of all studies were reported in all studies. Adjustment for potential confounding factors differed across studies, and the main adjusted factors were age, sex, comorbidity and so on. In addition, all three studies were rated nine stars on the NOS and were considered of high quality.

Characteristics of studies included in the meta-analysis
Association between CO poisoning and dementia
All three selected studies were assessed to have high quality with a mean score of 9. The level of agreement between reviewers was 100%. Figure 2 shows a forest plot presenting the association between CO poisoning and the risk for dementia. The adjusted effect estimates of all three studies were shown after adjustment for age, sex and comorbidities including hypertension, diabetes and cerebrovascular disease. However, three studies were different with adjustment for other comorbidities, and only one study adjusted for geographic area and urbanization level of residence, and monthly insured premium. Heterogeneity across studies was also found to be statistically significant (I2=92%, p<0.001). The random effect model suggested significant increased risk for dementia in those who were exposed to CO poisoning compared with those who were not (overall HR=2.61, 95% CI 1.56–4.36). The quality of evidence for this outcome was rated as high.
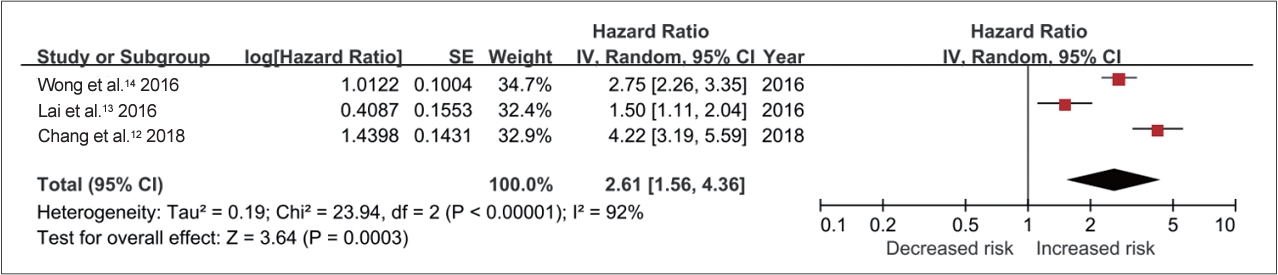
Hazard ratios for the association of CO poisoning with risk of dementia from pooled analysis of three cohort studies. SE, standard error; CI, confidence intervals; CO, carbon monoxide.
Subgroup analyses
Two published studies by Lai et al. [13] and Wong et al. [14] provided detailed data on the stratified analysis based on the sex of CO poisoning patients. Overall, 23,631 patients with CO poisoning and 94,520 controls were included, with 49.4% (n=11,681) female. As illustrated in Figure 3, there was substantial heterogeneity across the studies (I2=79% in males and 85% in females), indicating a very high degree of variation. A random-effects model meta-analysis found no increase in the risk of dementia in subjects with female patients (HR 1.78; 95% CI 0.80–3.97). The quality of evidence for this outcome was rated as very low. The risk of dementia was increased in male patients with CO poisoning (HR 2.31; 95% CI 1.39–3.85). We interpreted the quality of evidence for this outcome as high.
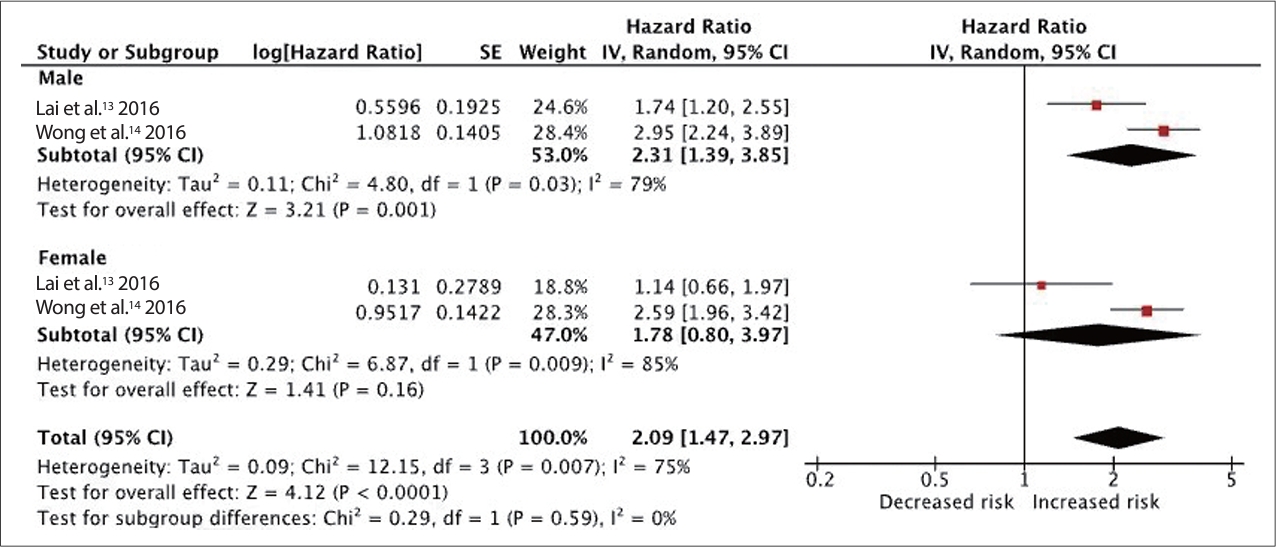
Hazard ratios for the association of CO poisoning with risk of dementia in male and female subgroups from pooled analysis of two cohort studies. SE, standard error; CI, confidence intervals; CO, carbon monoxide.
Although the boundary values of age groups between the two studies are different, they can be divided into three groups according to the young, middle and old groups. Figure 4 shows the adjusted HRs for the association between CO exposure and incident dementia were 5.18 (95% CI 1.30–20.59) in young group, 3.74 (95% CI 1.11–12.60) in middle age group and 1.70 (95% CI 0.69–4.17) in old group, respectively. We judged the quality of evidence for this outcome as high.
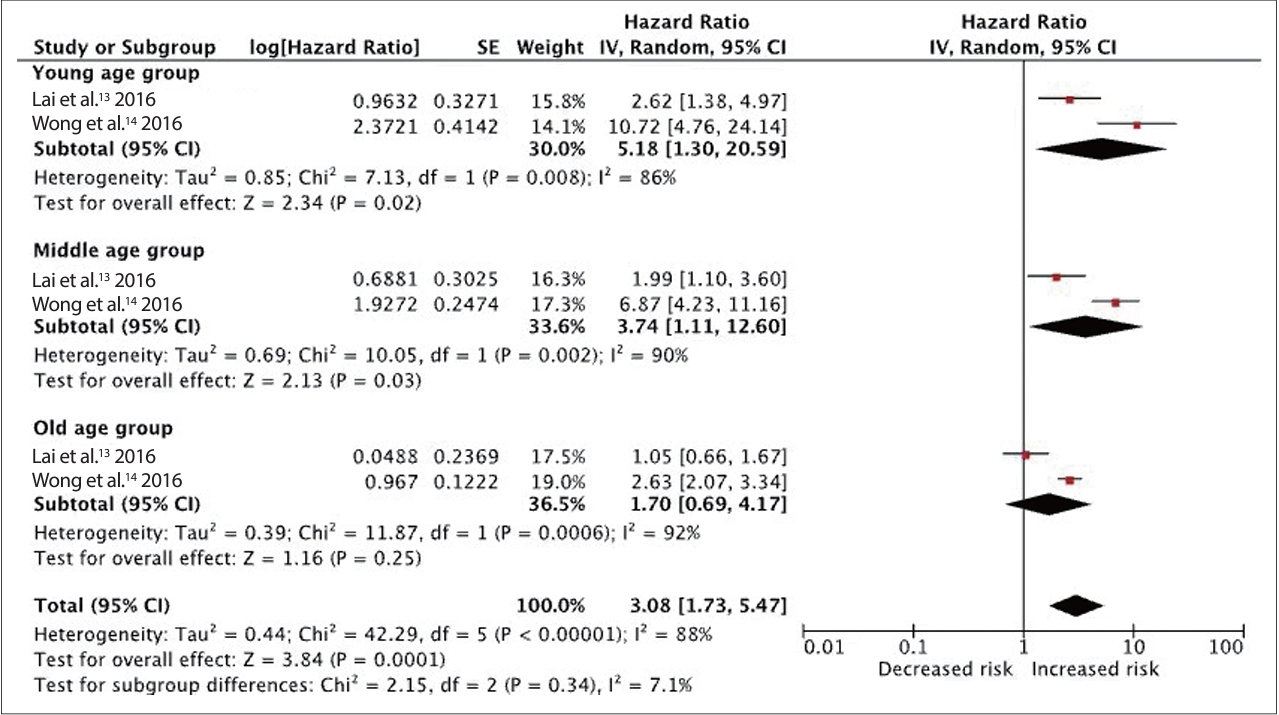
Hazard ratios for the association of CO poisoning with risk of dementia in young-, middle-, and old-age groups from pooled analysis of two cohort studies. SE, standard error; CI, confidence intervals; CO, carbon monoxide.
Subgroup analyses indicate that these findings were robust, as the same direction in HRs was evident in male and female, and younger and older age groups, even though it was not significant in some subgroups.
Sensitivity analyses
In this study, the results of sensitivity analyses show that the pooled positive effect estimate was no longer statistically significant after omitting one of selected studies, which indicated that there was a significant trend that the overall result was influenced by an individual study [14].
DISCUSSION
Clinical implications
To the best of our knowledge, this is the first systematic review and meta-analysis focusing on the contribution of CO poisoning on the incident dementia. The results indicate that the risk of dementia in the CO exposed cohorts was more than twofold higher than that in reference population. Subgroup analysis based on sex and age of participants find most of subgroups of CO poisoning to be associated with an increased risk of dementia. The present study is robust because of high quality of the prospective study design and minimized the selection and recall bias. Nonetheless, it is important to note that the heterogeneity of selected studies might attenuate the strength of the result to some degree.
The neurobiological mechanism underlying the association between CO poisoning and dementia has to be elucidated. CO poisoning causes impaired oxygen delivery and mitochondrial oxygen utilization as well as generation of reactive oxygen species. Because of the strong binding to Hb facilitated by the high affinity for the iron ions, high levels of CO exposure diminishes the oxygen-carrying and delivery capacity of the blood. CO poisoning causes brain hypoxia, which may lead to inflammation and subsequent injury. An earlier study found from 63 suspected patients that CO poisoning could cause acute inflammatory responses, even for patients with short-term exposure [22]. Extravascular CO is bound to molecules such as myoglobin, cytochromes, and nicotinamide adenine dinucleotide phosphate reductase, resulting in impairment of oxidative phosphorylation at the mitochondrial level. Besides, subsequent oxidative stress, and inflammatory responses induced by many hypoxia-independent pathways also contribute to cause nerve damage [12]. Much evidence suggests that CO toxicity may result in increased reactive oxygen species, free radical, or neuronal nitric oxide, which likely contributes to lipid peroxidation and neuronal and/or cellular injury. Oxidative stress is usually caused by an increase in the production of reactive oxygen species, or an inefficient antioxidant defense system, or a combination of both. Oxidative stress can trigger a series of pathophysiological processes leading to cellular injury and toxicity [23].
A randomized clinical trial has found CO poisoning can induce apolipoprotein E (APOE) epsilon4 carriers suffer greater morbidity [24], and the APOE epsilon4 allele was a well known genetic risk factor for dementia [25,26] and Alzheimer’s disease [27], the primary cause of dementia in the elderly. Currently, we realized that CO poisoning could cause neurological and neuropsychological problems, but the incidence of sequelae after poisoning was unclear. A registry-based observational study in Korea showed that 26.1% of patients with acute CO poisoning developed delayed neurological sequelae within 6 weeks of discharge [28]. According to the Weaver’s reported, 46% of patients with CO poisoning had abnormal neuropsychological findings and symptoms at 6 weeks [29], 19% had cognitive impairment [30], and 37% had abnormal neurologic findings on examination during 6-year follow up [31]. The studies included in this meta-analysis reported that the incidence rate of dementia was from 15.2 ranging to 23.33 per 10,000 person-years in patients with CO poisoning.
In this study, HRs for the association of CO exposure with incident dementia were highest in young age, followed by middle-aged group. And it was also higher in male than in female. It implied that young and male CO-poisoning patients are more prone to suffer from dementia and need exclusive clinical care. The increasing incidence of mental disorders and intentional or suicide attempt by CO poisoning in the young [32] may be a potential cause for the association of CO poisoning with increased risk of dementia, but further research is needed to confirm this possibility. Due to the difference in alveolar ventilation and total Hb mass between genders, women had a shorter CO clearance compared to men, even after adjusting for ventilation rate [33]. This could explain for the greater likelihood of dementia related CO poisoning in the young-and middle-aged males. Therefore, we should focus on preventing CO poisoning accidents occurred at home and in the workplace and public areas [16]. In addition, charcoal-burning suicides became popular in some East Asian countries in the first decade of the 21st century [34]. Taiwan and Hong Kong were the epicenter of the charcoal burning suicide epidemic [35]. Suicides by CO poisoning were more likely to be males and ages 18 to 64 years, and least likely to have a previously identified mental disorder. But they had the highest risk of dementia after CO poisoning according to this meta-analysis. This has important public health implications given that the young- and middle-aged males, as a group, are known to be less likely to be cared. It highlights that they are worthy to be more concern.
There have been no recent new options for therapy [36]. The standard treatment for CO poisoning includes the administration of oxygen and general supportive care [37]. Hyperbaric oxygen (HBO) treatment significantly reduces the half-life of COHb [38]. Several evidences have showed the benefits from HBO therapy on memory [29,39], delayed neuropsychological sequelae [40,41] and lowing mortality [42], but evidences supporting the use of HBO in patients with CO poisoning come from randomized trials with significant limitations and observational studies. So, identifying patients who will benefit from HBO treatment remains uncertain. In addition, some discordant findings were noted in a randomized trial of 191 patients with CO poisoning, which failed to document benefit, but found more delayed neurologic sequelae for HBO-treated patients [43]. The risk for poisoning-related cognitive sequelae was influenced by various factors such as age, CO exposure interval, poisoning severity and genetic predisposition [25,44]. Thus, whether the benefits outweigh the potential harms of using HBO to treat CO poisoning remains unclear.
Methodological considerations
There are several limitations to this study. Firstly, only limited cohort studies were identified, and the subjects were based on Taiwanese population. Whether the risk of dementia differs in patients with CO poisoning elsewhere in the world is unclear. Secondly, all studies included in this systematic review based on the same database. Thus, the same patient may have been included repeatedly 1 to 3 times in this systematic review, and this database’s disadvantages would similarly present in this meta-analysis. For instance, dementia diagnosis based on International Classification of Diseases, Ninth Revision, Clinical Modification codes may be less accurate than that obtained through a complete interview and neurological examination. Furthermore, the generalizability of the results to populations in other countries is limited. Thirdly, we were unable to conduct subgroup analyses based on the severity level of CO poisoning because the included studies did not provide adequate data. Fourthly, patients who attempted charcoal burning suicide might have suffered more severe brain damage than patients of occupationally related CO poisoning. However, none of the three studies reported the rate of CO poisoning after charcoal-burning suicide.
Conclusion
These findings support a link between CO poisoning and dementia. This evidence implied that we should not only pay attention to the acute symptom in patients with CO poisoning, but also the long-term impact. Further studies that provide data for different ethnic groups are needed to clarify whether a subgroup of patients with CO exposure has an elevated risk of dementia.
Notes
Availability of Data and Material
All data generated or analyzed during the study are included in this published article (and its supplementary information files).
Conflicts of Interest
The authors have no potential conflicts of interest to disclose.
Author Contributions
Conceptualization: Tao-Hsin Tung, Ching-Wen Chien, Ping Tao. Data curation: Zhu Liduzi Jiesisibieke, Ho-Shan Wei, Pei-En Chen. Formal analysis: Zhu Liduzi Jiesisibieke, Ho-Shan Wei. Methodology: Tao-Hsin Tung. Supervision: Tao-Hsin Tung. Writing—original draft: Meixian Zhang, Zhu Liduzi Jiesisibiek. Writing—review & editing: Meixian Zhang, Tao-Hsin Tung.
Funding Statement
None
Acknowledgements
None