Clinical Characteristics and Precipitating Factors of Adolescent Suicide Attempters Admitted for Psychiatric Inpatient Care in South Korea
Article information
Abstract
Objective
We aimed to examine the rates, correlates, methods, and precipitating factors of suicide attempts among adolescent patients admitted for psychiatric inpatient care from 1999 to 2010 in a university hospital in Korea.
Methods
The subjects consisted of 728 patients who were admitted for psychiatric inpatient care in a university hospital over a 12-year period and who were aged 10-19 years at the time of admission. We retrospectively investigated the information on suicidal behaviors and other clinical information by reviewing the subjects' electronic medical records. Whether these patients had completed their suicide on 31 December 2010 was determined by a link to the database of the National Statistical Office.
Results
Among 728 subjects, 21.7% had suicidal ideation at admission, and 10.7% admitted for suicidal attempts. Female gender, divorced/widowed parents, and the presence of mood disorders were associated with a significantly increased likelihood of suicide attempts. Most common method of suicide attempts was cutting, and most common reason for suicide attempts was relationship problems within the primary support group. A diagnosis of schizophrenia was associated with increased risk of death by suicide after discharge.
Conclusion
These results highlight the role of specific psychosocial factor (e.g., relational problems) and psychiatric disorders (e.g., mood disorders) in the suicide attempts of Korean adolescents, and the need for effective prevention strategies for adolescents at risk for suicide.
INTRODUCTION
Adolescent suicide, the third leading cause of death among youth 15 to 19 years old, is a major public health concern.1,2 A previous suicide attempt is well-known risk factor for death by suicide.3,4,5 The concern about suicide attempts is heightened by their association with increased psychological impairment,6,7,8 death by suicide, and potential cost to emergency departments and other urgent care facilities.9 Studies on adolescent suicide attempts are largely based on analyses of individual risk factors, often focused on mental health symptoms. Risk factors for adolescent suicide attempts include general mental health problems,10 substance abuse,11 low self-esteem, and impulsivity.12 From a psychosocial perspective, suicide attempts among adolescents have been associated with problems in family communication or problem solving13,14 and lower parental monitoring,13,14 death or previous suicide attempts by family members or friends,5,15,16,17,18,19 and interpersonal problems.20,21,22,23,24
In comparison to the abundant information on adolescent suicide attempts in Western countries, there is a paucity of data on risk factors for and characteristics of suicide attempts among adolescents in Asia.24,25,26,27 This omission is particularly significant for Koreans because suicide rates have increased rapidly and steadily in recent years, particularly among adolescents, in Korea: while in 2000, on average, 6.4 suicides per 100,000 adolescents aged 10-24 years were observed, in 2010 this rate was 9.4 suicides per 100,000 individuals, and the Korea's ranking of adolescent suicide rates climbed from 18th to 5th in the Organization for Economic Cooperation and Development (OECD) countries over the past ten years. These findings are contrary to a decreasing trend of suicide mortality in adolescents of other OECD countries: while in 2000, on average across all OECD countries, 7.7 suicides per 100,000 adolescents aged 10-24 years were observed, in 2010 this rate was 6.5 suicides per100,000 individuals.28
The purpose of this article is to present the first descriptive data regarding suicide attempts within a Korean adolescent sample. Because suicide attempts are common among adolescents with mental health problems,5 we examined the rates, correlates, methods, and precipitating factors of suicide attempts among adolescent patients admitted to a 20-bed child and adolescent psychiatric ward from 1999 to 2010 in a university hospital located in Seoul, Korea. Our psychiatric ward is one of two closed psychiatric ward exclusively for child and adolescent patients in Korea. The patients admitted in this ward have various emotional and behavioral symptoms as well as psychotic symptoms, severe enough for their admission to the closed ward. We also investigated the suicide mortality rates of these patients over the study period using the database of the National Statistical Office (NSO), to which all deaths in Korea are reported by a document of death notice containing the cause of death.
METHODS
Subjects and procedures
The subjects consisted of all patients who were admitted for psychiatric inpatient care in a national university hospital over a 12-year period (from January 1999 to December 2010) and who were aged 10-19 years at the time of admission. The 12-year period of recruitment was chosen because electronic medical records have been available in the hospital since 1999, and we launched this study in January 2011. The average length of stay is 60.1 (SD 33.6) days6, the number of admission of each patient ranged from 1 to 6 (mean 1.4, SD 1.0), and the rates of recurrent admission (admission more than two times during 12-years of period) were 27%. For patients who had recurrent admission, medical records of each admission were all reviewed.
A board-certified child and adolescent psychiatrist reviewed the subjects' electronic medical records and determined whether the patients had suicidal ideation at admission or were admitted for suicide attempts. This information had been recorded in the admission notes. A suicide attempt was defined as "an act with nonfatal outcome, in which an individual deliberately initiates a noninhabitual behavior that, without intervention form others, will cause self-harm, or deliberately ingests a substance in excess of the prescribed or generally recognized therapeutic dosage, and which is aimed at realizing changes which the subject desired via the actual or expected physical consequences".29 For patients with suicide attempts, the method and precipitating factors of the suicide attempt were investigated. Socio-demographic and clinical characteristics as well as family-related factors (socio-economic status and family history of suicide) of the subjects were obtained by a child and adolescent psychiatry fellow through a retrospective chart review. The IQ had been measured by a psychologist using the Korean Educational Development Institute Wechsler Intelligence Scale for Children-Revised (KEDI-WISC-R).30 Family history of suicide had been obtained from the parent's report. The study was approved by the institutional review board (IRB) for human subjects at the Seoul National University College of Medicine.
Instruments
Psychiatric diagnosis
The medical record requirements of the participating hospital included one primary diagnosis and several auxiliary diagnoses based on the of the International Classification of Disease, 10th edition (ICD-10)31 coding in a discharge summary, which had been recorded by an attending board-certified psychiatrist after close inpatient observation, neuropsychological test, and clinical interview. The diagnosis of patients with multiple psychiatric disorders was made according to the primary ICD-10 diagnosis provided in the electronic medical records. For the purposes of the present study, these diagnoses were collapsed into eight diagnostic groups: organic mental disorders (F10-F19), psychotic disorders (F20-F29), affective disorders (F30-F33), neurotic disorders (F40-F48), disruptive behavioral disorders (F90-F92), mental retardation (F70-F79), eating disorders (F50), and Tourette's disorder (F95.2).
Method of suicide
Suicide methods were classified according to the international self-harm section (X60-X84) of the ICD-10 codes31: self-poisoning (X60-X69), hanging (X70), drowning (X71), firearms (X72-X74), burning (X75-X77), self-harm by sharp object (X78), self-harm by blunt objects (X79), jumping from a high place (X80), and others (X81-X84). For patients who used two (or more) methods of suicide (i.e., subjects who jumped from a height after drug intoxication), both methods were counted separately.
Precipitating factor of suicide
The reviewing psychiatrist determined the precipitating factors for suicide attempt according to the International Classification of External Causes of Injury (ICECI) system 32 based on the description about suicide causes and suicide-related events in the medical records. The ICECI classification of precipitating factors is as follows: 1) conflict in relationship with family member, partner, or friend, 2) death of a relative, partner, or friend, 3) physical problem, 4) psychological/psychiatric condition, 5) income-related/financial problem, 6) abuse, 7) legal system encounters, 8) other specified proximal risk factors, and 9) unspecified proximal risk factor. Among several precipitating factors of suicide attempt, the most recent crisis that led to the self-harm, which corresponds to the definition of 'proximal risk factor' of the ICECI, was considered as a precipitating factor in this study. According to this definition, for example, in case of a girl who had suffered from peer relationship problems over 1 year prior and was affected by psychotic symptoms recently and attempted suicide, the precipitating factor would not be peer relationship problems but rather psychotic symptoms. In the case of suicide attempters with multiple precipitating factors, only one precipitating factor, the most temporally recent crisis that led to a suicide attempt, was selected.
Suicide mortality
Information about whether the patients had been alive at the time of December 31, 2010 was provided by linkage to the database of the NSO. The NSO data and hospital records were matched using the unique national identification number assigned to all Korean citizens. Data were censored either on date of death or on 31 December 2010. Person-years were calculated for each patient. For those dead, causes of death were also established through linkage to the database of the NSO. The causes of death were categorized based on the ICD-10 classification as follows:31 1) infectious diseases, 2) neoplasms, 3) hematological diseases, 4) endocrine diseases, 5) mental and behavioral diseases, 6) nervous system diseases, 7) circulatory system diseases, 8) respiratory system diseases, 9) digestive system diseases, 10) skin and subcutaneous system diseases, 11) musculoskeletal system and connective tissue disease, 12) genitourinary system diseases, 13) diseases ill defined, and 14) traumatic episodes (injury, poisoning and certain other consequences of external causes). For traumatic episodes, external causes of death were also established as follows: 1) accident, 2) intentional self-harm, 3) assault, and 4) event of undetermined intent. Among these external causes of death, only death by intentional self-harm was considered as a completed suicide.
Statistical analysis
Descriptive statistics of sample characteristics and methods and precipitating factor of suicide were presented. We compared socio-demographic and clinical differences between adolescent inpatients with and without suicide attempts using an independent t-test for continuous variables and the chi-square or Fisher's exact tests for categorical variables. Multivariate logistic regression analysis was used to identify correlates of suicide attempts among adolescent inpatients. All statistical analyses were performed using SPSS (version 19.0; SPSS Inc., Chicago, IL, USA), with statistical significance defined as an alpha level <0.05.
The frequency of death by suicide was calculated as the number of deaths by suicide as a function of the person-years of follow-up. Standardized mortality ratios (SMRs) were calculated with PAMCOMP 1.41.33 SMRs compare the observed numbers of deaths with the expected numbers of deaths. The expected number of suicide-specific deaths was calculated from the suicide mortality rate in Korea for different age groups of males and females from 1999 to 2010.
RESULTS
A total of 728 patients (441 boys and 287 girls) were enrolled in the study. Of these patients, 553 (63.2%) were males, and the remaining 322 (36.8%) were females. The mean age was 14.6 (SD 1.7) years. Of the patients in the study, 22 percent (20.4% of boys and 23.7% of girls) had suicidal ideation at admission, and 10.7 percent of patients (8.2% of boys and 14.6% of girls) were admitted for suicidal attempts (Table 1).
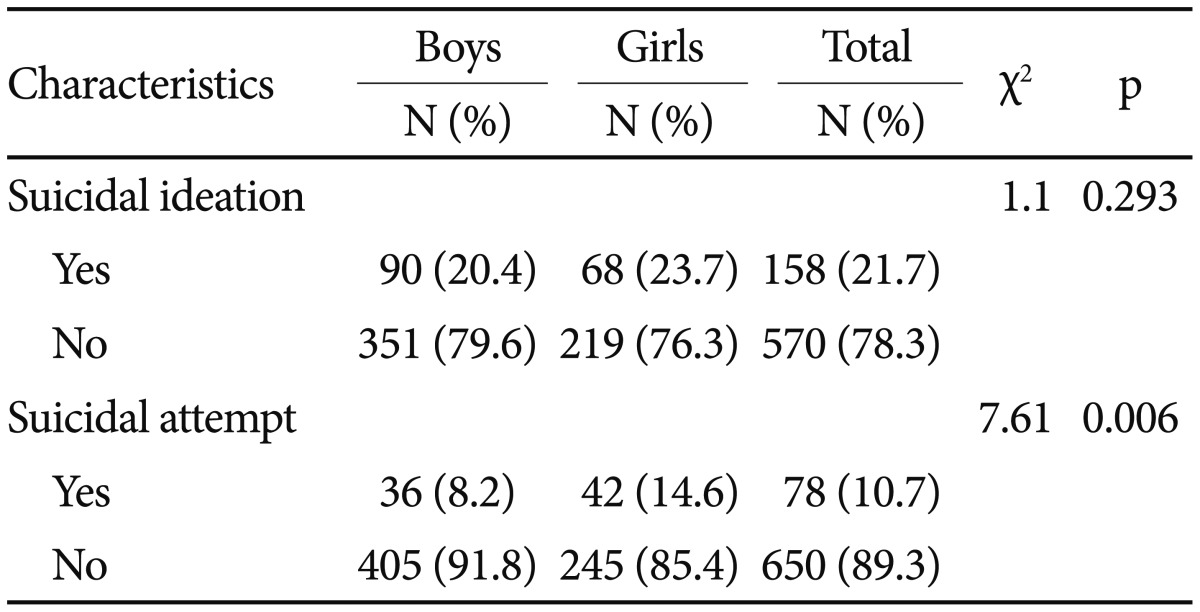
Prevalence of suicidal ideation, attempts, and family history of suicide among child and adolescent inpatients (N=728)
Patients with suicide attempts were older and were more likely to be female and to have higher IQ, divorced or widowed parents, and mood disorder (Table 2). They were less likely to have disruptive behavioral disorders or mental retardation than were patients without suicide attempts (Table 3).

Differences between child and adolescent inpatients with and without suicide attempt

Comparison of diagnosis between child and adolescent inpatients with and without suicide attempt
Multivariate analyses showed that female gender, divorced or widowed parents, and the presence of mood disorders were independently associated with suicide attempts upon presentation at the hospital (Table 4).
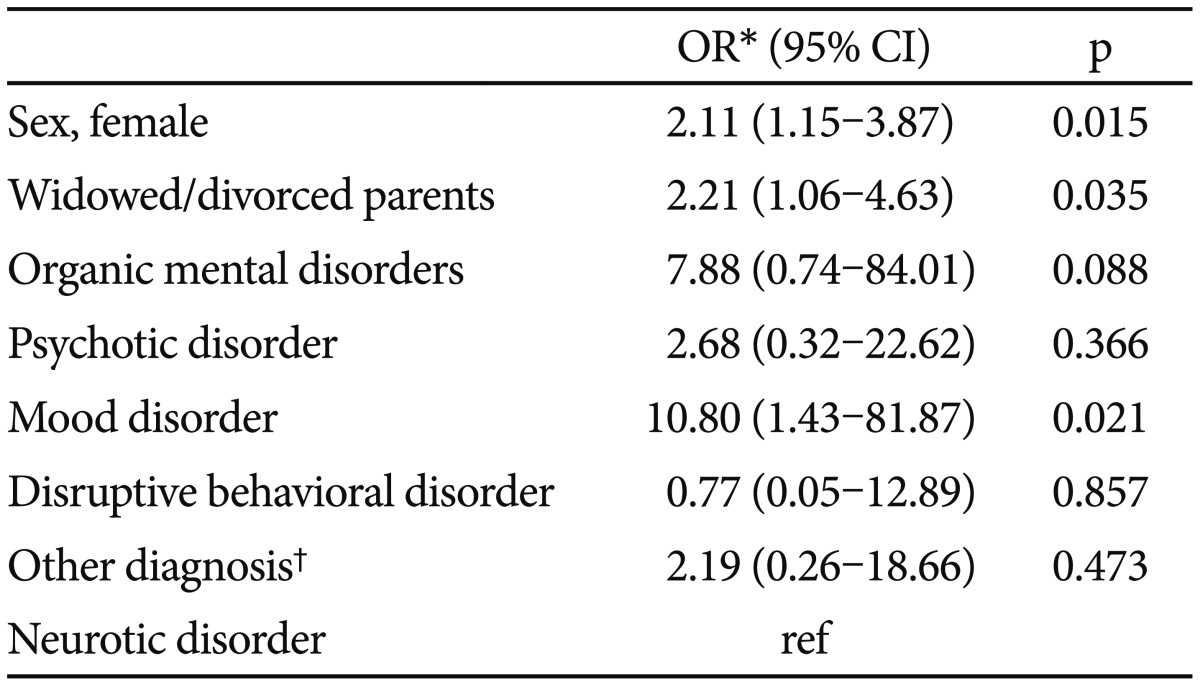
Correlates of suicide attempts among child and adolescent inpatients
Common methods of suicide attempts were cutting and jumping for boys (n=12, 33.3% for each) and cutting (n=25, 59.5%) and drug intoxication (n=10, 27.8%) for girls. Jumping was more common as suicide methods for boys than for girls (n=12, 33.3% vs. n=5, 12.2%), and cutting was more common for girls than for boys (n=25, 59.5% vs. n=12, 33.3%) (Table 5).
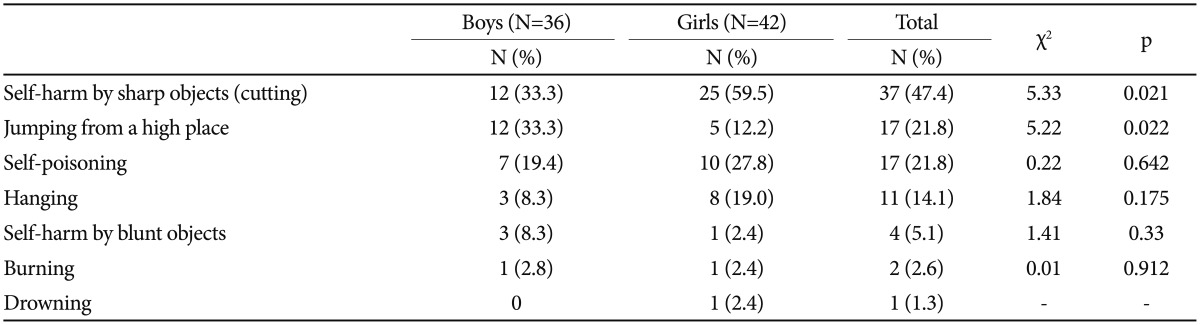
Methods of suicide attempts among child and adolescent inpatients
Common precipitating factors for suicide attempts were bullying or collective social exclusion (n=22, 28.2%), parent-child relationship problems (n=12, 28.2%), and psychotic symptoms (n=16, 20.5%). Psychotic symptoms were more common as precipitating factors for boys than for girls (n=12, 33.3% vs. n=4, 9.5%), and depression was more common for girls than for boys (n=4, 11.1% vs. n=7, 16.7%) (Table 6).
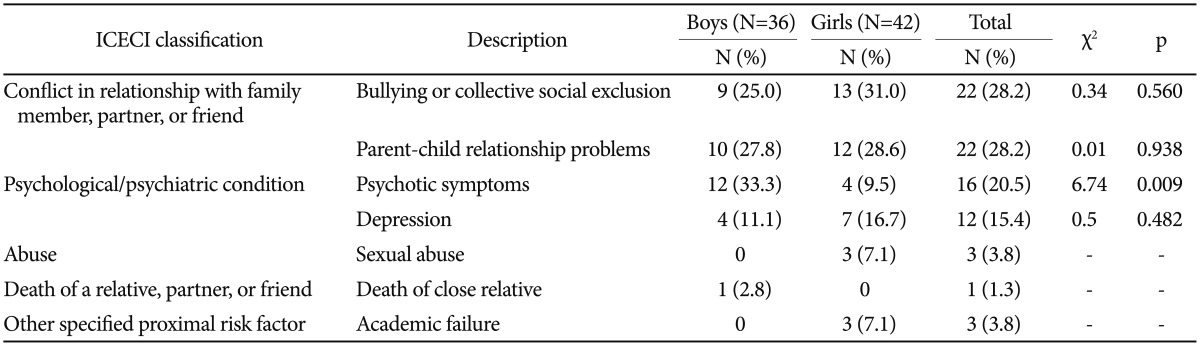
Precipitating factors for suicide attempts among child and adolescent inpatients
Of the 728 patients, 7 (0.96%, 3 females and 4 males) had died by December 2010. Among these 7 patients, 4 (0.55%, 3 females and 1 male) had died from suicide, and remaining 3 had died from digestive system disease, mental and behavioral diseases, diseases ill defined. Based on SMRs adjusted for age and gender differences between the study population and the general Korean population, the suicide mortality rate of the adolescent psychiatric patients was 17.7 times (95% CI 4.8-45.4) higher than that of the general population. All 4 patients who completed their suicide had been diagnosed with schizophrenia at admission, and only one patient had been admitted for a suicide attempt.
DISCUSSION
Among adolescent psychiatric patients, approximately twenty percent had suicidal ideation at admission, and 10.7 percent attempted suicide prior to hospitalization. Female gender, having a divorced or widowed parent, and the presence of mood disorder were associated with a significantly increased likelihood of suicide attempt upon presentation at the hospital. Cutting was the most common method of attempted suicide, and relationship problems with the primary support group were frequent precipitating factors for suicide.
Previous studies have reported that the prevalence rates of suicide attempts are two to three times higher in females than in males,34 although males have higher rates of death by suicide in adolescence and adulthood.34,35 We also found that suicide attempts were more common in girls than in boys. Consistent with previous studies conducted in adolescent psychiatric inpatients,13,14 suicide attempters were more likely to have a divorced or widowed parent. Adolescents from non-intact family are less likely to have and maintain healthy relationships with their parents, and these parent-child relationship problems are common precipitating factors for suicide attempts.5,15,16,17
Consistent with previous studies,1,15,17 we found that mood disorders had a substantial impact on the risks of suicide attempts in adolescent psychiatric patients. Longitudinal studies also support associations between mood disorders and attempted or completed suicide.36
Cutting, jumping, and drug intoxication were the most common methods of attempted suicide by adolescents. Previous research has found that intentional overdose and wrist cutting are the most common methods of attempting suicide in Western adolescent psychiatric inpatients.37,38 Jumping from heights is the second most common method for suicide attempters in our study, although attempted suicide by jumping is a relatively uncommon method in most Western countries. These differences in methods of suicide between countries may be related to the methods' availability. In Korea, drugs are difficult to access by adolescents. Thus, many adolescents living in high-rise buildings choose to jump from heights, a readily available method. When we compared the methods of suicide attempt by gender, boys were more likely to use jumping, while girls were more likely to do it by cutting. The high lethality of jumping, a suicide method commonly used by boys, contributes to the higher suicide mortality in boys, although girls typically have a higher rate of suicide attempts than boys do.34
Our findings of relationship problems with the primary support group, such as parents and friends, as the most commonly reported central precipitating factor for suicide attempts among both males and females should guide interventions designed to address these problems. Several previous studies have found that relational problems are central to the development toward a suicide attempt in adolescent psychiatric patients.14,39 Negative parent-child relationships have a central and enduring role in the suicidal behavior of adolescents and young adults.15,40 In our study, peer relationship problems (22.2%) were reported as precipitating factors as often as relationship problems with parents (22.8%) and mainly included bullying or collective social exclusion. Victimization in school by peers has an association to suicide that exceeds the risks of age, race, gender, and even depressive symptoms.41 Fear of social exclusion from the peer group may be particularly strong in a collective society such as Korea.42 Despite the high frequency of mood disorder in suicide attempters (29.8%), depression was reported as a precipitating factor only in a 15.4% of suicide attempters. This result may be due that we selected only one precipitating factor in each patient. Many depressive patients also had another precipitating factor such as a conflict in relationship with parent or friend, and such event was often judged as the most temporally recent crisis that led to a suicide attempt in many cases. When we compared the precipitating factor by gender, predominant psychotic symptoms for boys and predominant depression for girls seem to be consistent with other studies that examined factors associated with suicide attempts among adolescents.10 In our study, other problems, such as sexual abuse and academic failure, were identified as precipitating factors, but only for females.
In our clinical sample, 0.55% of the adolescents had completed their suicide by December 2010, a number 15 times higher than expected in the general population of Korean adolescents. Although this conclusion is based on only four cases, this figure is almost identical to those reported in previous Swedish,43 Finnish,44 and US studies.45 The four adolescents who committed suicide were suffering from schizophrenia, which is a commonly reported risk factor for suicide.43,56,47 Suicide by schizophrenic patients often occurs early in the course of the disease.48,49,50,51 Therefore, adolescents with schizophrenia are particularly at risk. In our study, only one patient was a former suicide attempter, suggesting that adolescents with schizophrenia merit clinical attention to safeguard against suicide risk even if they have no history of previous suicide attempts. It should be noted that NSO data may underestimate the number of deaths due to suicide because some suicides may have been classified as "undetermined" deaths.52,53 Among seven deaths in our patients, there were two undetermined deaths-death from diseases ill-defined and death from mental and behavioral disease.
The present study has several limitations. First, the study employed a retrospective methodological design. Because data were gathered from electronic medical charts rather than face-to-face interviews, some important information such as severity of the suicide attempt or number of previous attempt was not available in many patients, so was not included as a correlate variable in this study. Moreover, chart review was not done by the attending psychiatric resident or fellow who had recorded medical chart, but by another psychiatrist. Second, because the study was conducted in a single university hospital, the findings may not be representative of all psychiatric adolescent inpatients in Korea. Third, we could not examine the effect of comorbid psychiatric conditions on suicide attempts because only a primary diagnosis was considered in this study. Prior research has suggested that patients with comorbid conditions are at elevated risk of suicide.5,50,54 Finally, the very low number of deaths by suicide limited the statistical analysis of risk factors for completed suicide. Although suicide was more common in our psychiatric population than in the general population, large sample sizes are needed to study rare outcomes. Thus, additional prospective, controlled studies in many hospitals nationwide are required.
Despite these limitations, the present observations highlight the role of specific psychosocial factor (e.g., relational problems) and psychiatric disorders (e.g., mood disorders) in the suicide attempts of Korean adolescents. In terms of clinical implications, our results indicate that preventive work should be directed toward solving relational issues, both at home and at school, and active treatment of mood or psychotic disorders.
Acknowledgments
This study was supported by grant 04-2011-0620 from the Seoul National University Hospital Research Fund and by the National Research Foundation of Korea (NRF Grant funded by the Korean Govrnment (MSIP) (No. 2014R1A1A3049818).