Evaluation of a Functional Model of Acquired Capability for Suicide in a Nationwide Sample of Korean Adults
Article information
Abstract
Objective
We examined a functional model of acquired capability for suicide, which was elaborated from the “Interpersonal-Psychological Theory of Suicide”.
Methods
A total of 6,027 Korean community subjects were recruited from The Korean Epidemiologic Catchment Area study conducted in 2011. The subjects were assessed systematically using the Korean version of the Composite International Diagnostic Interview version 2.1, the Korean version of the Barratt Impulsiveness Scale, and the Korean version of the Mood Disorder Questionnaire. We used structural equation modeling to identify potential factors contributing to a suicide attempt.
Results
Most aspects of the model were supported by the data and “the short-term enhancer for the acquired capability for suicide” had direct effects on suicide attempts. However, the suicidal planning effects of “the short-term enhancer for the acquired capability for suicide” were eliminated by the rule of parsimony.
Conclusion
The main finding was that “the short-term enhancer for the acquired capability for suicide” is relevant to suicide attempts when it's direct, indirect, and reciprocal effects are tested within a more complete system of relationships than found in existing studies. The implications of these findings are discussed with regard to future conceptual work and empirical research.
INTRODUCTION
It is well known that not all people who have suicidal thoughts or ideation attempt suicide and that only a fraction of those who attempt suicide actually die. In response, Joiner1 claimed that “even if people desire to commit suicide, only those who are realistically capable in committing suicide end up dying due to suicide.” As a possible answer, Joiner2 developed the “Interpersonal-Psychological Theory of Suicide-a functional model of the acquired capability for suicide” as an integrated model for suicide attempts. He said that suicide can be explained in three dimensions: 1) thwarted belongingness; 2) perceived ineffectiveness and resultant burdensomeness to others; and 3) the acquired capability for suicide.
Joiner et al.3 suggested that the acquired capability for suicide can act as a limiting factor to determine who among individuals that experience a serious desire for death by suicide will and will not die by suicide. However, suicide is a statistically very rare incident, and the act of suicide contradicts millions of years of evolutionary self-preservation programming.4 Therefore, this capability for suicide typically involves a long and difficult process that develops over time, and Joiner describes that acquired capability as a condition involving a heightened degree of fearlessness and pain insensitivity such that the action and ideas involved in suicide are no longer alarming.1 This kind of experience was described in Solomon's opponent process theory.
In addition to Joiner's theory, Smith and Cukrowicz5 argued that life experiences containing painful and provocative elements occurring in conjunction with the specific diatheses described earlier result in fearlessness of suicide and tolerance to the physical pain involved in suicide. The first point on vulnerability stems from research suggesting that suicide attempters, particularly violent attempters, experience reduced serotonergic activity.67 Low levels of serotonin have been associated with personality variables, such as aggression and impulsivity.7 Impulsivity is a risk factor for suicide capability based, in part, on the fact that impulsive people are less likely to heed warning signs against self-harm. Of the vulnerabilities that stem from life events, the experience of physically painful and psychologically provocative life events is the most important.8 These experiences interact with the aforementioned dispositions, resulting in life threats or reduced warning signs against painful events, which, in turn, develop the capability of suicide.9 Hypothetical experiences, such as mental rehearsal for suicide, can accelerate acquired skill or ability.1 Smith et al.9 claimed that these experiences in the form of acquired skills help reduce the fears of suicide and develop the strength to bear the physical pain when attempting suicide. In contrast, cultures or religions, such as Catholicism, that oppose suicide are a protective factor.
Joiner1 described the acquired capability for suicide as a static process that involves crossing of some idiosyncratic threshold after which the individual is perpetually capable of suicide. However, Smith et al.9 suggested that an individual can develop the capability for suicide in the moment via intoxication, psychosis, and so forth. This is the main difference between their suicide models. Smith et al.9 called the reinforcer “capability for suicide in the moment (short-term capability)”. These actions or experiences that serve to reduce the perceptions of fear and sensations of pain involved in suicide in the short-term include substance intoxication, dissociative states, psychotic episodes, and manic episodes.101112
Therefore, the theoretical research of Smith et al.9 proposed a new concept in which the structural construction of the “the acquired capability for suicide” integrates a relatively time-stable factor as well as factors that can expedite the capability in the short-term. Furthermore, they have conceptualized not only serious and lethal suicide attempts, but also relatively less severe and successful suicide attempts. However, because the theoretical framework was proposed relatively recently, no study has validated the current model. The present experientially examined Smith et al.'s9 “A functional model of the acquired capability component of the interpersonal-psychological theory of suicide”.
Based on previous studies related to suicide and the acquired capability theory, the research topics of this study are: 1) Impulsivity, attitudes toward religion, pain and trauma experience as latent variables for acquired suicide capability. 2) Manic symptoms, alcohol-related disorder, and psychosis as latent variables of short-term enhancers for acquired capability. Path hypotheses are as follows. 1) and 2) “Suicidal ideation” is positively related to “the short-term enhancer for the acquired capability and suicidal plan”. 3) and 4) “Suicide plan” is positively related to “the short-term enhancer and the acquired capability for suicide”. 5) “The short-term enhancer” is positively related to “the acquired capability for suicide”. 6) “The acquired capability for suicide: is positively related to “suicide attempt”.
METHODS
Sample
The Korean Epidemiologic Catchment Area (KECA) study was conducted in 200113 and 200614 using the Korean version of the Composite International Diagnostic Interview 2.1 (K-CIDI 2.1).15 A follow-up to the KECA study was conducted in 2011. This follow-up was designed to determine the lifetime and 12-month prevalence, socioeconomic correlates, and comorbidities of major mental disorders in the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) among Korean adults. Subjects were selected using a stratified, multi-stage, clustered sample design, based on a population census conducted by community registry offices in 2010. One individual per selected household, with the earliest birthday, with reference to the day of the birth month, was chosen randomly. From an initially selected 8,196 subjects (age, 18–74 years), 6,027 face-to-face interviews (73.5% response rate) were conducted.
Seventy-eight interviewers were recruited from each catchment area for the 78 interview. These interviewers were psychiatric nurses, social workers, and medical students, all of whom were familiar with psychiatric epidemiologic surveys. The three psychiatrists who served as trainers were certified by the Composite International Diagnostic Interview training center at the University of Michigan (USA). All interviewers participated in a 5-day training session that included didactic sessions to review general interview skills and the interview instrument, mock interviews, and role-playing exercises.1617 Trainers monitored interviews on closed-circuit television and provided feedback.
Assessment
Korean version of the Composite International Diagnostic Interview
Trained lay interviewers administered the K-CIDI15 to each subject. The CIDI18 is a fully structured diagnostic modality designed to establish psychiatric diagnoses based on the definitions and criteria in the DSM-IV.19 The K-CIDI was developed according to World Health Organization (WHO) guidelines.20 The inter-rater reliability, test/retest reliability, and validity of the K-CIDI showed kappa values of 0.86–1.00, 0.42–0.89, and 0.50–1.00, respectively. In the present study, we analyzed the relationships between exposure to childhood trauma and lifetime prevalence of specific psychiatric disorders. Each variable containing a missing value was estimated using the maximum likelihood method (MLM).
Religious attitudes
A demographics item (DE3) in the CIDI interview was used to explore religious attitudes. We hypothesized that the responders' positive attitude about their religion was negatively correlated with suicide attempts. Religious attitudes were assessed with a single question: “How important is religion to you (if you have a religion)?” Religious attitude were evaluated using quartiles of one (not at all important) to four (very important).
Pain experience
Using the Pain disorder section of the K-CIDI, chronic pain experience (at any time during life) was assessed, including abdominal pain, back pain, arthralgia, limb pain, chest pain, headache, menstrual pain, dysuria, penile pain, and any other pain. Each pain experience was counted as 1 point, and the sum of the total score was recorded (0–10).
Traumatic event experience
Using the Post-Traumatic Stress Disorder section of the K-CIDI, exposure to the following post-traumatic events (at any time during life) was initially assessed, including military combat, sudden injury/accident, natural disaster, seeing someone hurt or killed, rape, sexual assault, physical assault, threat/kidnapping, torture, or other traumatic event. The subject's age at the time of the event was also recorded. Each traumatic experience was counted as 1 point, and the sum of the total score was recorded (0–12).
Suicidality
We used the K-CIDI module on suicide to assess lifetime suicidality, including suicidal ideation, suicidal plans, and suicide attempts. These questions were used in the WHO-Suicide Prevention Multisite Intervention Study on Suicidal Behaviors.212223 Suicidal ideation was assessed with the following question: “Have you ever seriously thought about committing suicide?” Existence of a suicide plan was assessed with the following question: “Have you ever concretely planned suicide?” Suicide attempts were assessed with the following question: “Have you ever attempted suicide?” Information on age at the time of the first suicide attempt and number of suicide attempts was also collected.
Korean version of the Barratt Impulsiveness Scale
The BIS was translated to Korean by Lee,24 and we used the standardized BIS 11. The BIS is comprised of 23 items divided into three subcategories: nine questions pertain to unplanned/impulsivity, eight to motor impulsivity, and six to cognitive impulsivity. The internal consistencies determined in a previous study that used the impulsivity scale in terms of unplanned/impulsivity, motor impulsivity, and cognitive impulsivity were 0.30, 81, and 0.51, respectively. The current study's total internal consistency was 0.86.
Korean version of the Mood Disorder Questionnaire
Hirschfeld et al.25 developed the MDQ to distinguish bipolar disorder. This self-report questionnaire was developed based on the DSM-IV criteria for bipolar disorder in which in criterion 1 of the 13 items they must report “yes” to at least seven. These items must appear at the same time for criterion 2, and significant impairment must be experienced due to these symptoms for criterion 3. Therefore, if all three criteria are satisfied, bipolar spectrum disorder is concluded. However, the K-MDQ was translated and standardized by Jon et al.26 and unlike the original questionnaire, criteria 2 and 3 have been omitted, and bipolar disorder is determined by a minimum score of 7 on criterion 1.
Latent variables
Acquired capability for suicide
The variables that comprise the acquired capability for suicide are: attitudes toward religion (sociocultural background of suicide), pain experience (habituation of distress), traumatic experience (habituation of psychological distress), and impulsivity (dispositional factors).
Short-term enhancer (of acquired capability for suicide)
Latent variables that may temporarily increase the acquired capability for suicide have been assumed, and alcohol use disorder and manic symptoms (K-MDQ) of the variables were measured.
Statistical analysis
Descriptive statistics are used for the entire sample with SPSS 18.0 software (SPSS Inc., Chicago, IL, USA). A structural equation model (SEM) analysis was performed with AMOS 18.0. The SEM analysis is used to assess the causal relationships among exogenous, mediator, and criterion variables simultaneously.2728 We organized the SEMs, which consisted of observed and latent variables, using AMOS 18.0 software, and then calculated the maximum likelihood estimate for the model parameters using covariance of the total sample. Goodness of fit of the data for the proposed model was assessed with chi-square indices (χ2), the normed fit index (NFI), the comparative fit index (CFI), and the root mean square error of approximation (RMSEA).
RESULTS
Sociodemographic characteristics of the subjects
A total of 6,022 respondents were included (2,308 males and 3,714 females; male: female ratio, 1 : 1.61. In total, 4,894 respondents (1,910 males and 2,984 females) were <64 years. A 12-year education was the most common with 2,161 respondents and 1,694 respondents reported being unemployed. A total of 3,494 respondents reported having a religion and the majority of the respondents lived in an urban district (Table 1).
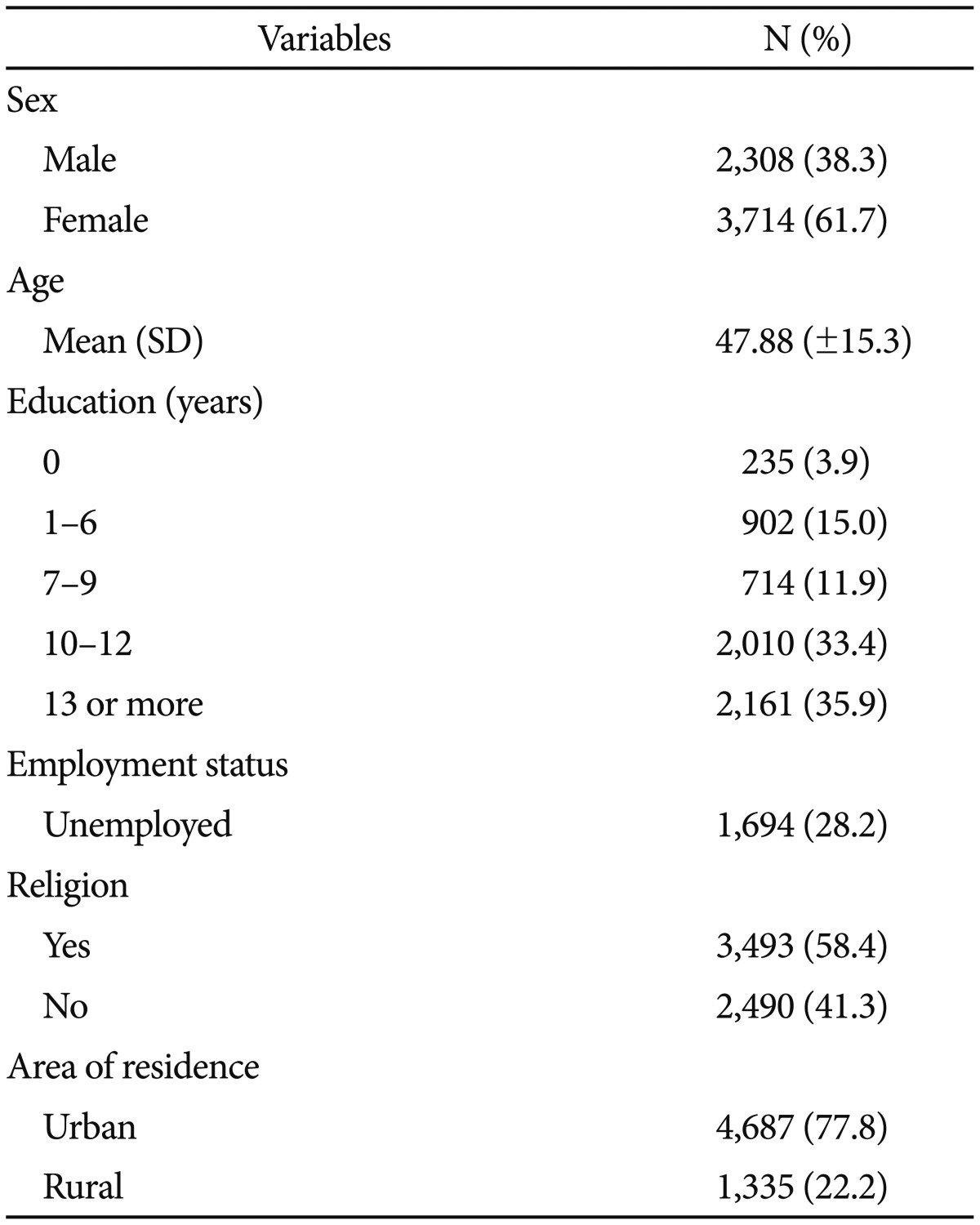
Socio-demographic characteristics of subjects
The clinical characteristics of the respondents were suggested by constructing three latent variables from the observed variables. As results, mean BIS scale score was 45.19 [standard deviation (SD)=0.18], and the means of each religious attitude are shown in Table 2. A total of 1,143 (19%) respondents reported chronic pain symptoms and 1,556 (25.8%) reported traumatic experiences. Mean MDQ score was 20.96 (SD=0.01). A total of 647 (10.7%) respondents had an alcohol-related disorder, 34 (0.6%) suffered from psychosis, 951 (15.8%) had experienced suicidal ideation, 210 (3.5%) had a suicide plan, and 201 (3.3%) had attempted suicide (Table 2).
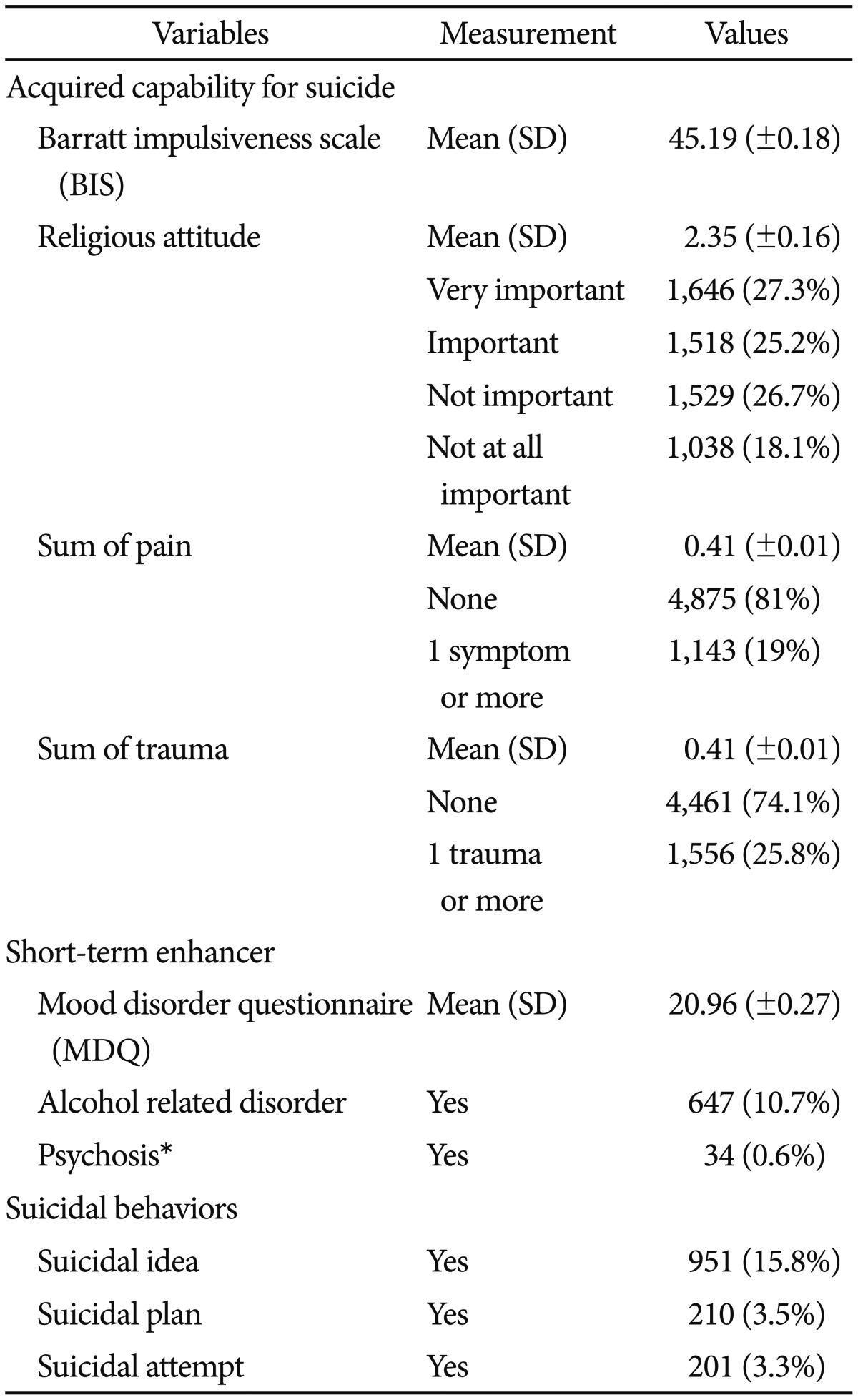
Clinical characteristics of subjects
Evaluation of proposed models
SEM was used to assess the relationships between the suicidal ideation, suicide attempts, and other related factors of the acquired capability for suicide for the Korean community sample based on the factor analysis results of the combined data. SEM is a technique to simultaneously estimate the relationships between observed and latent variables (measurement model) and the relationships between latent variables (structural model). SEM has gained popularity because it combines confirmatory factor analysis and regression analysis to model a variety of psychological, sociological, and other relationships.
We designed the SEM to examine the relationships between latent and observed variables. Our primary purpose was to identify the existence of mediating variables that were not studied clearly in the “acquired capability for suicide model”. Based on a literature review, we designed a causal relationship model between suicidal ideation and suicide attempts. We then added and tested the relationships between “the acquired capability for suicide”, “the short-term enhancer of acquired capability”, and “suicide plan” as multiple mediating variables.
The proposed model hypothesized that significant causal relationships exist between two latent constructs of “the acquired capability for suicide”, “the short-term enhancer for acquired capability”, and three observed variables, such as “suicide ideation”, “suicide plan”, and “suicide attempt”. The causal relationships represented the six hypotheses in the path model (Figure 1). Empirical evaluation of such hypotheses is complicated by the fact that latent constructs are not directly observable. The evaluation was based on sets of observed or measured variables that serve as indicators of latent variables, and the relationships between the observed and latent variables were estimated using factor analysis.
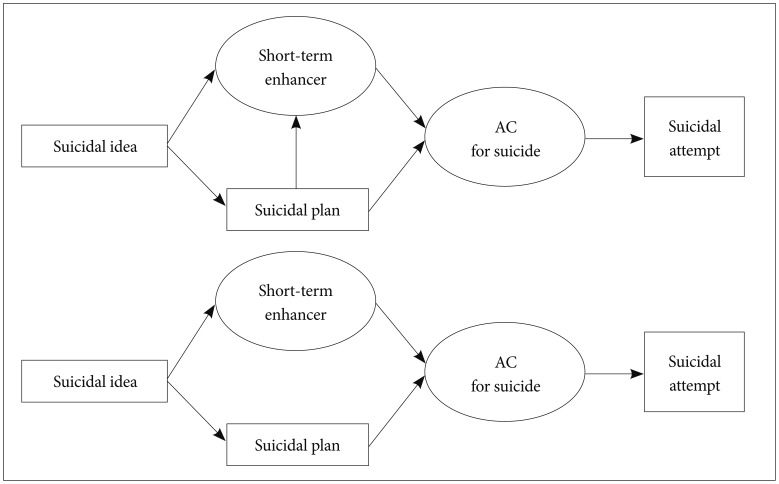
Comparison between the original model (including the pathway from suicide plan to short-term enhancer) and the modified model (not including that pathway). AC: Acquired Capability.
As a result, all estimated factor loadings were significantly related between the latent and observed variables (Table 3). We detected positive relationships for all variables, except religious attitudes. This result supports our premise that religious attitudes are a protective factor for suicide attempts.
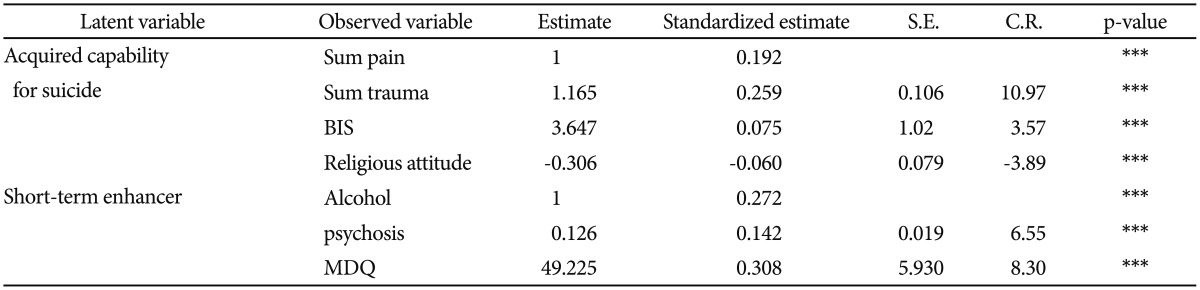
Estimation of relationship between observed variables and latent variables
All path coefficients were significantly related with each other. Path hypotheses 1 and 2 (i.e., “suicidal idea” is positively related to “ the short-term enhancer for the acquired capability and suicidal plan”) were supported at an optimal level with a standardized estimate of 0.431 (p<0.001) and a standardized estimate of 0.504 (p<0.001). Path hypotheses 3 and 4 (i.e., “suicide plan” is positively related to “the short-term enhancer and the acquired capability for suicide”) was supported with a standardized estimate of 0.100 (p<0.013) and a standardized estimate of 0.684 (p<0.001). Path hypothesis 5 (i.e., “the short-term enhancer” is positively related to “the acquired capability for suicide”) was supported with a standardized estimate of 0.596 (p<0.001). Path hypothesis 6 (i.e., “the acquired capability for suicide” is positively related to “suicide attempt”) was supported at a standardized estimate of 0.690 (p<0.001) (Table 4).
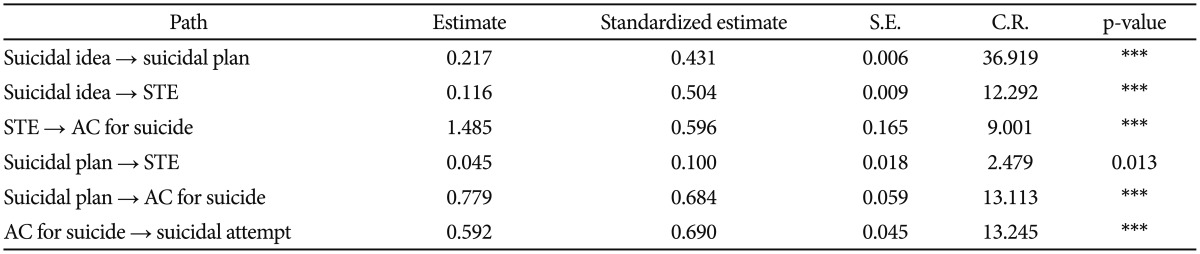
Estimation of path coefficients
We adopted the SEM model comparison method as a model selection strategy. First, we added a modified model to the original model and calculated the difference in model fit. Our modified model was a nested model in which a pathway was removed from the original model (Figure 1). Model fit determines the degree to which the SEM fits the sample data.29 As a result, all confirmatory factor analyses (CFAs) of constructs and path analyses produced a relatively good fit, as indicated by the goodness of fit indices, such as CFI >0.90 and a RMSEA value <0.08.30 The results of the absolute measures for the original and modified models clearly surpassed the cut-off values, confirming that the structural model highly fit the sample data (original model: χ2=389.996, df=33, NFI=0.924, CFI=0.930, RMSEA=0.042; modified model: χ2=393.204, df=34, NFI= 0.923, CFI=0.929, RMSEA=0.042). We used the MLM to estimate the parameters.
We examined the chi-square difference test to compare the original and modified models (Figure 1). Because the modified model is nested in the original model, a chi-square difference test can be applied to determine relative parsimony. According to the model fit analysis, the difference between the two models was 3.208 (Δdf=1), which is smaller than 3.84 (0.95 χ2 2). Therefore, the modified model was selected by the rule of parsimony as the final model, and the path from suicide plan to short-term enhancer was eliminated. This result seems reasonable because the short-term enhancer has an indiscreet and reckless property. Thus, we accepted our modified model as the final model (Figure 2).
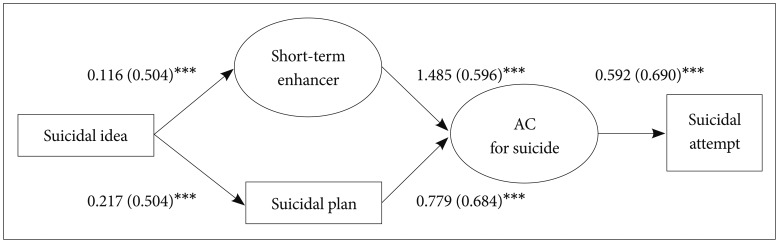
Final structural model of the constructs for suicidal behavior, including standardized path coefficients and levels of significance (***p<0.001). AC: Acquired Capability.
Previous studies have supported a causal relationship between “the acquired capability for suicide” and “suicide attempts” in patients with a psychiatric disorder.313233 Joiner's1 concept of the “acquired capability for suicide” has gradual and intentional growth by (internal) psychological rehearsal or (external) physical exposure. However, Smith et al.9 added the variable, “short-term bolstering of the capability for suicide during a suicide attempt'(we call it “short-term enhancer” in this study). This variable could be an explanation for non-intentional suicide attempt. In this context, our finding of no causal relationship between suicide planning and short-term enhancer may be a more plausible result than that of the original model.
DISCUSSION
We examined “a functional model of the acquired capability for suicide”9 and our data support their conceptual model. In our model, the short-term enhancer, as a latent variable, was also supported empirically, which is our most important finding. In our study, short-term enhancers may have been a useful concept to evaluate unintentional and unplanned suicide attempts. Further research in this field is needed to discuss integrating short-term enhancers for the acquired capability theory. It is a very important finding that Smith and Cukrowicz's model was supported with an optimal level of model fit in a large Korean communuity sample. Therefore, preventing suicide should have different interventions between those who have specific suicide plans and others who have drug addictions, psychotic episodes, or manic episodes.101112
Our study holds additional significance beyond the aforementioned findings. First, as a nation that has received attention due to its high suicide rate, we explored the psychological factors that may influence suicidal ideation leading to an actual suicide attempt in a large community sample through the SEM. This study was made possible with exemplary data because of expansion of the representative sample due to acquisition of national data. The 2011 Korean Mental Illness Epidemiological Investigation allowed inclusive and strict data to be acquired to measure sociocultural backgrounds in relation to suicide, mental illnesses that increase the possibility of suicide attempts, subjective experiences of trauma and pain, impulsivity, and manic tendencies. Beyond lethal suicide attempts, models related to unsuccessful suicide attempts were also explored. Kessler et al.34 referred to the 2001–2003 American National Comorbidity Survey, in which 3.3% of Americans reported suicidal ideation but the actual percentage of who attempted suicide was only 42.5%. In contrast, those who had attempted suicide previously reported more suicide-related symptoms,35 with greater chances of more lethal suicide attempts.36 Joiner2 responded to this phenomenon by developing the “Interpersonal-Psychological Theory of Suicide–a functional model of the acquired capability for suicide” as an integrated model for suicide attempts. Joiner1 claimed that painful or stimulating experiences, such as physical violence, self-injury, and substance abuse, can indirectly help develop suicidal capability, even if such experiences are not explicitly related to an actual suicidal attempt. In agreement with Joiner's claim, many studies have shown that substance abuse, prostitution, and physically violent activities are related to suicide attempts and death due to suicide and are therefore contributing factors that heighten the danger of suicide.373839 While Joiner's1 the model aims to predict serious and lethal suicide attempts, Smith et al.'s9 model aims to conceptualize nonlethal suicide-related behaviors. Therefore, an empirical study that examines experiential data of unsuccessful suicide attempters within an inclusive model increases the overall understanding of suicidal behavior. Although such attempters did not succeed in committing suicide, distinguishing these people who may show progressive danger early on, is useful.
Although this study supports our proposed model with a good model fit, the limitations include weak homogeneity on the religious attitude sub-scale. Previous studies mentioned that religion affects suicide, particularly the “Catholic tradition” which has the strictest dogma regarding suicide.5 However, our “religious attitude” item included Catholicism, Buddhism, Protestantism, Protestant Christianity, and other religions. The second limitation was only including the sample of community-dwelling individuals, as particular populations have a higher prevalence of mental health problems. Third, most of the diagnostic information was based on life-time prevalence; therefore, differences based on age were not considered. Fourth, sex differences in the acquired capability for suicide were not explored. Previous studies have reported that males acquire the capability for suicide more frequently than that of females, and males report greater sensation-seeking tendencies.40 Fifth, the relationship between capability for suicide and an actual measured scale was not executed (e.g., Nademin et al.'s42 the “acquired capability for suicide scale”). Sixth, we could not include all variables related to suicide (e.g., neurological process, abuse history, accidental experience, profession, etc). Due to the physical limitations of such a large-scale interview, we omitted some important variables because our data set is a part of product from the nationwide mental health program. At the time (2009–2010) that mental health program had designed, Smith et al.'s9 model was not published. However, we believed that the crucial observed variables can support the conceptual model in our study. Finally, our data were cross-sectional. In fact, the cross-sectional nature of the study was a limitation, as we could not establish definite causal relationships. We attempted to examine the possibility of suicide attempts via the impulsive pathway.
In summary, we verified Smith et al.'s9 “functional model of the acquired capability for suicide.” Notwithstanding the limitations, this study holds significance as the first large-scale community sample in which statistics supported the model. Because the data were acquired previously, new variables were unable to be introduced. However, the goodness-of-fit of the model was sufficient for future investigations. It is hoped that future studies do not merely gather data in terms of mental health and suicide but rather investigate the direction of a more developed and structured model.
Acknowledgments
This study was funded by the Korean Ministry of Health and Welfare. The authors wish to express gratitude to 12 local investigators and 79 interviewers. This study was supported by the Korea Healthcare Technology R&D project, Ministry of Health & Welfare, Republic of Korea (grant number A120051).