Validation Study of Kim's Smoking Cessation Motivation Scale and Its Predictive Implications for Smoking Cessation
Article information
Abstract
Objective
The purpose of this study was to develop a scale to measure motivation for smoking cessation. Motivation is known to be important for success of smoking cessation. The reliability of the scale was assessed and its predictive validity for smoking cessation was evaluated.
Methods
We recruited 333 men aged 20 to 70 that visited smoking cessation clinics at seven public health centers. The demographic characteristics were recorded and the Korean version of Stages of Readiness for Change and Eagerness for Treatment Scale for Smoking (K-SO-CRATES-S) performed. A smoking cessation motivation scale was developed with 10 questions based on the theory of motivation enhancement therapy.
Results
The motivation scale was composed of four subscales based on the factor analysis; each subscale had an adequate degree of internal consistency. In addition, the newly developed scale had a high degree of validity based on its significant correlation with the smoking version of SOCRATES. Moreover, the precontemplation level of motivation was found to significantly predict the success of smoking cessation. And one of the subscales of the Korean Nicotine Dependence Syndrome Scale (K-NDSS), stereotypy which also significantly predicted the success of smoking cessation, significantly correlated with the preparation 1 and 2 level of motivation.
Conclusion
The smoking cessation motivation scale with 10 questions that was developed in this study was a highly reliable and valid scale for the prediction of success for smoking cessation for those who wanted to stop smoking.
Introduction
Seriousness of smoking and treatments in South Korea
Many common diseases are affected by smoking in South Korea. A large study conducted in the U.S. in 1982 showed that smoking was associated with various cancers including oral, pharyngeal, laryngeal, and esophageal cancers as well as lung cancer.1 In addition, passive smoking has been shown to have negative effects on health in humans.2 Because of the wide publicity of the negative effects of smoking many adults attempt to stop smoking. However, although every year many people try to stop smoking, a considerable number are not successful.3 Therefore, individuals who attempt smoking cessation require advice from professionals, systematic support and novel approaches to achieve smoking cessation.
In South Korea, there are smoking cessation clinics in local public health centers that are operated with support from the Ministry for Health, Welfare and Family Affairs. The average success rate for smoking cessation is relatively higher compared to that of other countries. Although this rate might be overestimated, as data for it were collected verbally, the results are encouraging.
Results of previous studies
Scales are necessary to evaluate the success rates of programs for the development of new programs for smoking cessation. Scales measuring smoking patterns are important for the evaluation of potential candidates for smoking cessation programs. Shiffman et al.4 developed the Nicotine Dependence Syndrome Scale (NDSS) that measures smoking patterns with five subscales that illustrate the degree of nicotine dependence. This scale has been translated and validated with the consent of the original authors; the translated version has high reliability (Cronbach's alpha=0.90) and some subscales have shown a high predictive validity for the success of smoking cessation.5 Smokers with low levels of continuity and stereotypy have been found to be more successful in their attempts to stop smoking. Investigators believe that the continuity and stereotypy subscales are associated with smoking patterns rather than smoking dependence and can be assessed as a predictive variable for the likelihood of successful smoking cessation. The motivation for smoking cessation may be an important variable that can predict the success of smoking cessation attempts. But a motivation scale for smoking cessation has not been developed yet in Korea, and it seems true of other countries. Stages of Readiness for Change and Eagerness for Treatment Scales version 8.0 (SOCRATES) was designed by Miller and Tonigan6 and validated for Koreans by Chun.7,8 But these SOCRATES and Korean version of the SOCRATES (K-SOCRATES) were scales for patients with alcohol dependence. Therefore development of smoking cessation motivation scale for patients with nicotine dependence is very necessary and important.
Significance of developing a motivation scale for smoking cessation
The development of a scale to measure motivation for smoking cessation might aid smoking cessation programs and future research on smoking cessation. Motivation enhancement therapy has been shown to be successful for the treatment of various dependencies including alcohol dependence.9 Therefore, a motivation scale based on motivation enhancement therapy was developed6 and our group modified it for smokers. If smokers have a low motivation for smoking cessation and a high failure rate, the success rate for smoking cessation might improve by providing intensive motivation enhancement therapy. Although all clients may benefit from motivation enhancement therapy, a more targeted approach is needed for the clinical setting where resources are limited. Therefore, a smoking cessation motivation scale was developed that could be used to evaluate baseline motivation and the effects of motivation enhancement therapy. The goal of this study was to develop a scale to measure motivation for smoking cessation and to determine its effect on smoking cessation.
Methods
Participants
Three hundred thirty three male clients who were attending smoking cessation clinics, were randomly selected at seven public health centers. They agreed to participate in this research by informed consent in May 2007. Their demographic characteristics are shown in Table 1.
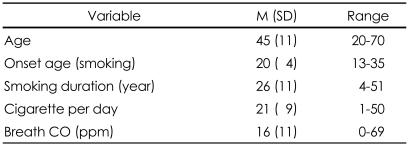
Demographic variables
Procedures
Development of a Smoking Cessation Motivation Scale
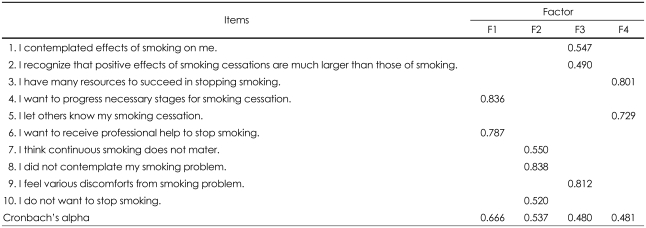
According to the Stage of Change Theory, suggested by the motivation enhancement therapy of Miller,6 20 preliminary questions assessing the pre-contemplation, contemplation and preparation levels were chosen. Then, a final 10 questions were chosen by two psychiatrists and a clinical psychologist. Questions related to the levels after preparation were excluded. This was because the questions were to be used to screen smokers with a high risk of failure for smoking cessation at an early stage of evaluation in the smoking cessation clinics; it was assumed that the action and maintenance levels would be rare among such patients. Ten questions were included in the scale based on motivation enhancement therapy. The ten questions were translated into English by two professionals fluent in both English and Korean and are shown in Table 2.
Factor structure and reliability of smoking cessation motivation scale
Administering of Smoking Related Scales and Evaluation of Success Rate of Smoking Cessation
The scales were administered to participants in the study and maintenance of smoking cessation was measured at the twelfth week after providing nicotine replacement therapy. The success with smoking cessation was self-reported verbally in person to interviewer. Participants needed to be completely smoke free throughout the twelve-week period to qualify as a success with smoking cessation.
Measurement
Kim's Smoking Cessation Motivation Scale
The scale developed for this study included 10 questions administered at the early stages of pre-contemplation, contemplation and preparation. The total scale consists of three subscales logically, and higher score of each subscale indicate greater level of motivation. Therefore the questions of pre-contemplation were scored inversely, and the total score means high motivation in smoking cessation.
The answers were graded by 1-5 points. To avoid the effects of random responses some questions were scored inversely. Inversely scored items were 7, 8, 10.
Korean version of Stages of Readiness for Change and Eagerness for Treatment Scale for Smoking
To verify the concurrent validity of Kim's Smoking Cessation Motivation Scale (KSCMS) developed for this study the K-SOCRATES-S was used by modifying it to a K-SOCRATES; this scale was originally designed by Miller and Tonigan6 and validated for Koreans by Chun7,8 and modified into a nicotine dependence scale by our group. The subscales were taking steps, recognition and ambivalence; the Cronbach's alphas were 0.889, 0.836 and 0.508, respectively.
Korean Nicotine Dependence Syndrome Scale
The Korean NDSS (K-NDSS) translated by Park et al.5 was used; it measured the patterns and degree of nicotine dependence by the five subscales developed by Shiffman et al.4 The K-NDSS was translated with the approval of the original author. The subscales of the K-NDSS were drive, priority, continuity, tolerance, and stereotypy. Their Cronbach's alpha for the total scale and each of the five subscales was 0.90, 0.85, 0.72, 0.71, 0.78, and 0.66 respectively.
Statistical analysis
Composition of Sub-scales of Kim's Smoking Cessation Motivation Scale and Their Internal Consistency
The subscales for the smoking cessation motivation scale were identified by factor analysis. Scales with over one in Eigenvalue were chosen and the principal axis factor analysis and varimax rotation were used. The internal consistency of each subscale was measured.
Concurrent Validity of Kim's Smoking Cessation Motivation Scale
Pearson's correlation analysis of the KSCMS and K-SOCRATES-S subscales was conducted to verify the concurrent validity of KSCMS. In addition, Pearson's correlation analysis of KSCMS and K-NDSS was conducted.
Predictive Validity of Kim's Smoking Cessation Motivation Scale
To determine whether the motivation scale significantly predicted the success rate of smoking cessation a logistic regression analysis was performed with scores from the subscales of the motivation scale and the subscales of the K-NDSS as the independent variables and the success of smoking cessation at twelfth week as the dependent variable.
Results
Factor structure and internal consistency of the Kim's Smoking Cessation Motivation Scale
Through factor analysis, four factors were identified for measurement: the precontemplation level of motivation, the contemplation level of motivation, the preparation level of motivation 1, and the preparation level of motivation 2. The preparation level subscale was divided into the slightly forwarding contemplation level and an action level. Cronbach's alpha for total scale and each of the four subscales was 0.679, 0.537, 0.480, 0.666, and 0.481, respectively (Table 2).
Concurrent validity-correlations between subscales of the Kim's Smoking Cessation Motivation Scale and those of the Korean version of the Stages of Readiness for Change and Eagerness for Treatment Scales for Smoking version 8.0
The results of the correlation analysis of the KSCMS and K-SOCRATES-S subscales, conducted to verify the validity of the motivation scale, precontemplation, showed that it was positively related to recognition (r=0.227, p<0.001) and negatively correlated with ambivalence (r=-0.277, p<0.001) with the K-SOCRATES-S. Contemplation from the KSCMS was related to recognition (r=0.398, p<0.001) and taking steps (r=0.162, p<0.001). The preparation 1 level was positively correlated with recognition (r=0.328, p<0.001) and negatively correlated with ambivalence (-0.112, p<0.05). In addition, the preparation 2 level was positively related to taking steps (r=0.346, p<0.001) and ambivalence (r=0.207, p<0.001)(Table 3). Moreover, the preparation levels 1 and 2 had a significant correlation with stereotypy in the K-NDSS (r=0.133 p<0.05 and r=0.128, p<0.05 respectively).

Pearson correlation of between motivation sub-scales
Predictive validity of the success of smoking cessation by the Kim's Smoking Cessation Motivation Scale and the Korean Nicotine Dependence Syndrome Scale
The proportion of succeeded participants to relapsed participants for smoking cessation was 39% (n=130) to 61% (n=203) respectively. The logistic regression analysis showed that the precontemplation from the KSCMS and the continuity and stereotypy from the K-NDSS significantly predicted the success rate of smoking cessation. The results are shown in Table 4. Therefore, a higher level of motivation during the precontemplation stage, a higher level of stereotypy and a lower level of continuity of the smoking patterns resulted in a higher success rate for smoking cessation.
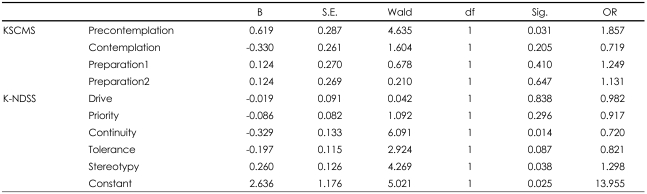
Logistic regression of success for smoking cessation
Discussion
Patients with addictive diseases have a high likelihood of very low treatment motivation in contrast to other diseases. They expect strong pleasure sensations and the positive feelings provided by their dependent drug and/or behavior. The use of motivation enhancement therapy as an intervention in such patients does not force them to accept their dependence as a disease; it encourages them to evaluate the positive and negative effects separate from the dependence, and changes in behavior to improve critical thinking and to strengthen the motivation to change.5 Changes in behavior have five stages: precontemplation, contemplation, preparation, action, and maintenance. It is assumed that a higher level of motivation leads to higher stages of change and finally results in behavior change and successful treatment of the dependency.10
SOCRATES has been used to measure the stages of change or motivation for change in patients with alcohol dependency; as translated by Chun7 and used in South Korea. This scale showed a high level of reliability and validity and was reported to accurately measure the motivation for change among participants. However, modification was required to apply it to smoking dependency and the large number of questions required further refinement.
In an attempt to improve the smoking cessation success rate among men attending local public health centers for aide in smoking cessation, we developed a simple motivation scale that is easy to administer and specific to smoking. The scales are based on the theory of motivation enhancement therapy. This therapy has been applied previously to dependency problems and its effectiveness confirmed locally and worldwide. Development of a scale easily applied with a small number of brief questions was provided that was adapted specifically to smoking cessation. The goal of the developed scales was to target smokers with low motivation so that they could be treated with more intensive motivation enhancement therapy. Once the high risk smokers were identified during early evaluation in a smoking cessation program the 10 questions developed could focus on the precontemplation, contemplation and preparation levels for more intensive therapy.
The results of this study showed that KSCMS consisted of four subscales, Cronbach's alpha for total scale and each of the four subscales was 0.679, 0.537, 0.480, 0.666, and 0.481, respectively. The concurrent validity of the scale was verified; it was significantly correlated with the translated SOCRATES-S sub-factors used for measuring the motivation for smoking cessation. In addition, when logistic regression analysis was performed on the success of smoking cessation at three month after the beginning of the intervention as a dependent variable and the sub-factors of the KSCMS and K-NDSS at the early evaluation stage as independent variables, the level of motivation at the precontemplation stage and continuity and stereotypy of the smoking patterns were found to be significantly effective measures. The results suggest that the smoking cessation motivation scale had a high level of predictive validity and showed that smokers with low motivation during the precontemplation stage and with low stereotypy and high continuity of smoking patterns had a high risk of failing their attempts at smoking cessation.
The results of this study have several limitations. Firstly, participants were all men visiting a clinic for smoking cessation. The findings cannot be applied to women who smoke. Further study is needed to confirm the findings and apply the methods used to a larger population of smokers including women. Secondly, the measurement of smoking cessation in this study was only self-reported verbally, not biochemically verified. Further study needs to use biochemical verification of smoking status.
Despite these limitations, these findings have clinical implications. Firstly, a smoking cessation motivation scale was developed in this study. Secondly, we investigated predictive variables of success for smoking cessation by logistic repression. The results of this study showed that a group of subjects at high risk for smoking cessation failure could be targeted early for more intensive therapy early during a smoking cessation program. This will hopefully lead to improved outcomes for smoking cessation. Further study is needed to further evaluate the scales used and confirm our findings.
Acknowledgments
This study was supported by a grant of the Korea Health 21R&D Project, Ministry for Health, Welfare and Family Affairs, Republic of Korea (A090058). And no author has any competing interest.