Feasibility of Psychosocial Distress Screening and Management Program for Hospitalized Cancer Patients
Article information
Abstract
Objective
Although the diagnosis and treatment of cancer is associated with psychosocial distress, routine distress screening is difficult in hospitalized oncology settings. We developed a consecutive screening program for psychosocial distress to promote psychiatric treatment of cancer patients and evaluated the feasibility of our program by Distress Thermometer (DT) and Hospital Anxiety and Depression Scale (HADS).
Methods
Among 777 cancer inpatients recruited from the Catholic Comprehensive Institute of Seoul St. Mary's Hospital, 499 agreed to complete primary distress screening through DT. We conducted secondary distress screening through HADS in 229 patients who had high scores of DT.
Results
Of the 499 participants, 270 patients with low scores of DT were included in the distress education program. 229 patients with high scores of DT received secondary distress screening through HADS. Among 115 patients with low scores of HADS, 111 patients received distress management. Among 114 patients with high scores in the secondary distress screening, 38 patients received psychiatric consultation service whereas 76 patients refused psychiatric consultation.
Conclusion
Using consecutive screening for psychosocial distress appeared to be feasible in an inpatient oncology setting. Nevertheless, the low participation rate of psychiatric consultation service in cancer patients with high distress level should be improved.
INTRODUCTION
Clinicians have been attentive to psychological aspects of cancer patients because cancer is a life-threatening disease. Since Derogatis et al.1 reported that almost half of cancer patients who were diagnosed had psychiatric disorders, several studies have shown that pathological levels of distress are very prevalent in cancer patients, ranging from 15 to 50%.2345 Distress ranges from normal feelings of vulnerability, sadness, and fears, leading to problems such as depression, anxiety, panic, social isolation, and existential and spiritual crisis.6
Several investigators have suggested that a high distress level in cancer patients might be correlated with several negative consequences such as decreased medical adherence, increased lengths of hospital stays, reduced quality of life, more psychological distress of family members, and possible increased mortality.789101112
For detecting prevalent psychiatric diseases in cancer patients that could be beneath the surface, psychological distress screening can be an optimal strategy. Several studies showed that psychological distress screening successfully detected psychiatric disorders of cancer patients.131415 Various psychiatric interventions such as pharmacotherapy, psychotherapy, and other psychosocial intervention are effective in improving depressive or anxious symptoms, quality of life, and satisfaction in the care of cancer patients.1617 The National Comprehensive Cancer Network18 and the National Institute for Health and Care Excellence19 recommended routine screening for distress in clinical practice.
Nevertheless, psychological distress of patients with cancer tends to be underrated. Only 14.3% of oncologists used instruments for screening psychosocial distress20 because of various reasons, such as excessive workloads, insufficient skills, and poor motivation. Furthermore, patients with cancer might often concentrate on their physical and life-threatening disease, although psychological distress might interfere with their ability to cope effectively with cancer. Indeed, development and appliance of novel screening program to assess psychological distress of cancer patients could be beneficial for them. A distress screening program for cancer patients should take diverse cultural and institutional circumstances into consideration.
The primary objective of this study was to assess the effectiveness of a distress screening and management system in oncology practice. The secondary objective was to assess the feasibility of the stepwise applications of Distress Thermometer (DT) and Hospital Anxiety and Depression Scale (HADS) and recommendations for referral to psycho-oncologist.
METHODS
Participants
A total of 777 subjects were inpatients (aged 18 or over) with confirmed histological diagnosis of cancer from the Seoul St. Mary's Hospital, Seoul, Republic of Korea. Inclusion criteria were: 1) cancer patients who were firstly admitted in the Catholic Comprehensive Cancer Institute in July 2007; 2) patients who were stratified according to the site of cancer diagnosis (colorectal, stomach, hepatobiliary, gynecological, lung, breast, thyroid, head and neck, and other cancer diagnosis); and 3) those who were able to read and understand Korean. This study was conducted in accordance with the ethical and safety guidelines set forth by the local Institutional Review Board of the Catholic University of Korea. Of the 999 subjects, 129 were excluded to participate because their first admissions were not for hospitalized interventions of oncology. The confinement of participants to first admission for oncologic interventions could clarify our feasibility study by eliminating overlapped data of a patient who hospitalized several times during the study period. Furthermore, we could focus on psychological distress of patients who experienced first-ever admission for oncologic intervention. A total of 149 patients were also excluded in this study, including 87 who had severe medical conditions, 8 who were discharged early (<24 hours), 8 who had cognitive impairments, and 2 who had severe psychiatric disorders.
Procedures
Included patients were contacted by a clinical research associate who introduced them to the objectives and procedures of the study. Oncology nurses or oncologists helped participants complete a primary distress screening through DT. Then the oncology nurses or oncologists helped participants with DT score over 4 complete a secondary distress screening using HADS. Patients with high score of HADS (over score of 13) were referred to psychiatric consultation service. Singer and colleagues reported that the best trade between sensitivity and specificity for the total scale was a ≥13 score for cancer patients.21 In primary distress screening, patients with DT score less than 4 were referred to distress education program. In secondary distress screening, patients with HADS score less than 13 were referred to the distress management program. Psychiatrists of psychiatric consultation service assessed patients with HADS score over 13 and applied various psychiatric interventions such as cognitive behavioral therapy, brief psychotherapy or pharmacotherapy.
Distress education
Patients with cancer was educated about psychological distress and coping method by oncologic nurses.
Distress management
Patients with cancer was received supportive psychotherapy three times by trained psychiatric nurses.
Psychiatric consultation service
Psychiatrist conducted psychiatric interviewing, diagnosed psychiatric disease, assessed disease severity, and decided appropriate interventions.
Measures
For all participants, medical data (type of cancer site, metastasis, medical comorbidity, time since diagnosis, reason to admission, and performance status), demographic data (age, sex, education, marital status, socioeconomic status, occupational status, residence, religion, smoking, and alcohol drinking), and psychosocial information were collected from a package that included questionnaires and interviews by oncology nurses, oncologists, and psychiatrists.
Distress Thermometer
In recent years, considering patients with cancer have difficulty in finishing long time interview or surveys, National Comprehensive Cancer Center Network (NCCN) suggested to use DT, a visual measurement scale with one sentence.22 Several investigators have reported that DT is simple with high validity.1823 DT was designed to score distress of cancer patients in a scale of 0 to 10. Score of 0 means ‘No distress’ whereas score of 10 means ‘Extreme distress’. In this study, we used the Korean version of DT previously validated by Shim and colleagues.24 The cutoff score was 4. Scores less than 4 means mild distress whereas score greater than 4 indicated severe distress.
Hospital Anxiety and Depression Scale
HADS, a self-assessment scale, was developed to detect states of depression, anxiety and psychological distress amongst patients who were being treated for a variety of clinical problems.25 Osborne and colleagues reported that HADS was an effective screening tool to measure anxiety and depression among inpatients with cancer.26 HADS consisted of 7 questions relating to depression and 7 questions relating to anxiety. Thus, HADS has a total of 14 items. Response to each question was scored on a scale of 0–3, with 3 indicating higher symptom frequencies. Score for each subscale (anxiety and depression) can range from 0–21. Total score was categorized into the following: normal (0–7), mild (8–10), moderate (11–14), and severe (15–21). Total score (emotional distress) ranged from 0–42, with higher scores indicating more distress. However, Dolbeault and colleagues studied several papers and reported that cutoff scores for overall psychological distress could vary when HADS was used as a global scale.2 We chose a cutoff value of the total score of HADS (depression score+anxiety score) greater than or equal to 13 to detect patients with significant level of emotional distress.
Statistical analyses
Statistical analyses for demographic and clinical data were performed with the Statistical Package for Social Sciences software (SPSS version 12.0, SPSS Inc., Chicago, IL, USA). For assessing potential differences between groups (non-distressed group vs. distressed group on primary distress screening, low-scored group vs. high-scored group on secondary distress screening, and refused group vs. accepted group of a psychiatric consultation service, respectively), independent t test for continuous variables and χ2 test for categorical variables were used. Fisher's exact test was applied if there are more than 20% of cells having expected number less than 5. All statistical analyses had a two-tailed α level of <0.05 for statistical significance.
RESULTS
Demographic and clinical characteristics
Data from 499 participants were analyzed. Demographic and clinical characteristics of participants are summarized in Table 1. Mean age of the study sample was 57.7±11.5 years. A total of 148 (29.7%) patients were over the age of 65 years. Of the 499 participants, 335 (67.1%) had education level over high school diploma, 423 (84.8%) were married. Cancer type, time since diagnosis, metastasis, and reason to admission were heterogeneous across patients. Twelve (2.6%) patients had psychiatric history. Four hundred and ninety one (98.4%) patients were at ambulatory state. Performance status was defined by Eastern Cooperative Oncology Group (ECOG).27
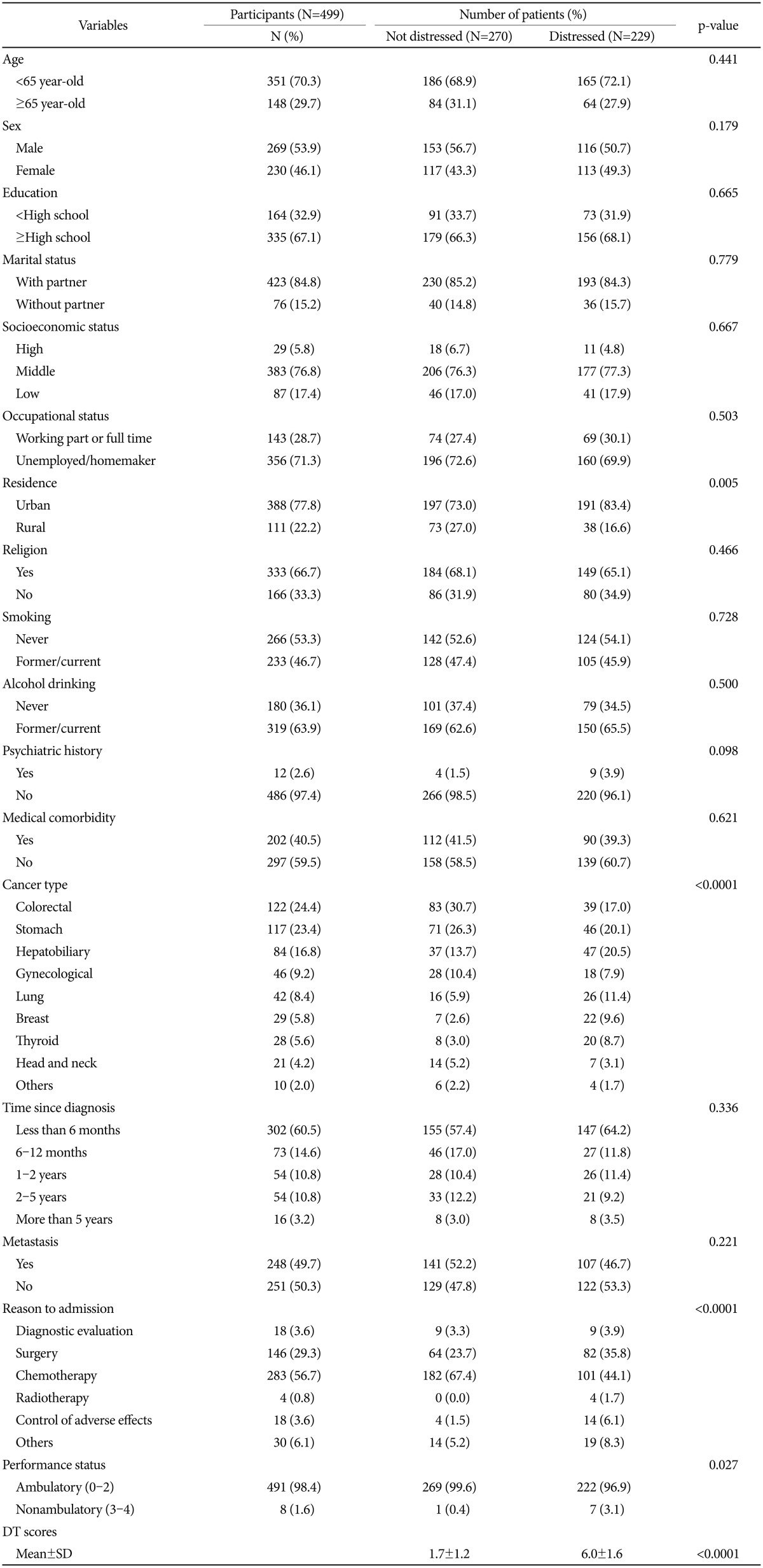
Demographic and clinical characteristics & comparison between cancer patients who not distressed and distressed using the Distress Thermometer from the primary distress screening
Feasibility
Among eligible participants (n=561) who had some form of DT, 62 (11.05%, 62/561) refused to be screened. A total of 499 patients (88.95%, 499/561) finished the primary distress screening using DT. The distribution of DT response of participants at the primary distress screening is shown in Figure 1. Of these 499 patients, 270 (54.10%, 270/499) who had DT scores less than 4 received distress education. A total of 229 patients (45.89%, 229/499) who had DT scores greater than 4 received the secondary distress screening through HADS. A total of 115 patients (50.22%, 115/229) had HADS scores less than 13 were screened again, of which 4 (3.48%, 4/115) refused to move on to the next step. Therefore, a total of 111 patients (96.52%, 111/115) received the distress management. Of 229 patients who had the secondary distress screening, 114 patients (49.78%, 114/229) had HADS score greater than 13, of which 38 (33.33%, 38/114) received psychiatric consultation service whereas 76 patients (66.67%, 76/114) refused the psychiatric consultation service (Figure 2). Of cancer patients who received the psychiatric consultation service, final diagnoses were major depressive disorder in 5 patients (13.16%), depressive disorder not otherwise specified in 12 patients (31.58%), generalized anxiety disorder in 2 patients (5.26%), anxiety disorder not otherwise specified in 5 patients (13.16%), and adjustment disorder in 14 patients (36.84%) according to the DSM-IV.
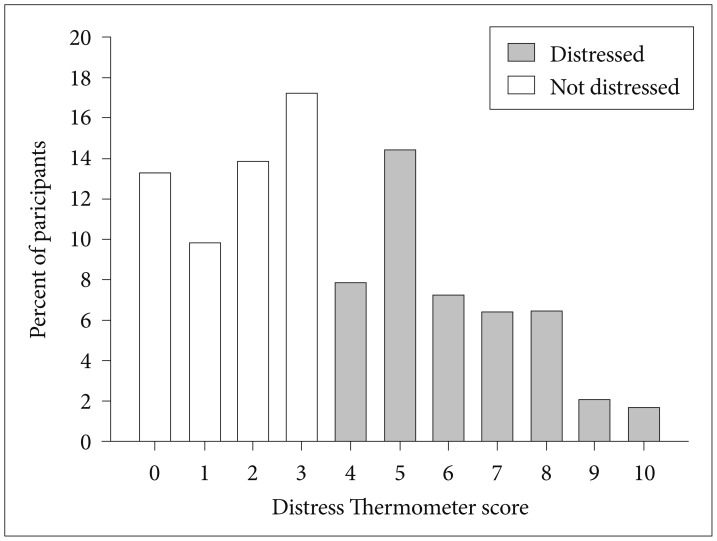
Distribution of the Distress Thermometer response of participants (N=499) at the primary distress screening.
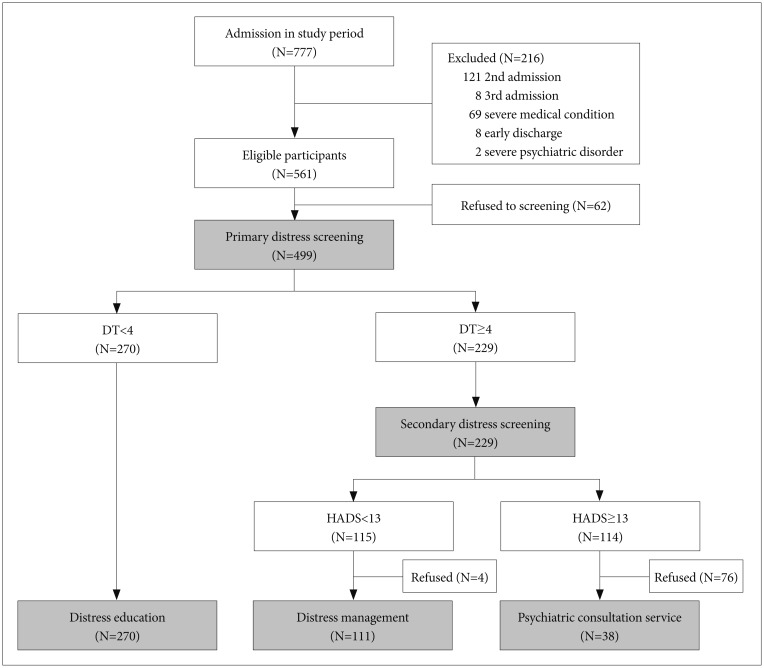
Procedure of the distress screening and management and number of patients at each stage. DT: Distress Thermometer, HADS: Hospital Anxiety and Depression Scale.
Differences of demographic, medical, and psychosocial characteristics between groups from the primary screening and the secondary distress screening
Patients who were residing in urban area showed higher DT score than patients who were residing in rural area (Table 1). Whether the DT score met the cutoff score of 4 was significantly related to cancer type, reason to admission, and performance status among clinical variables. HADS score that met the cutoff score of 13 on secondary distress screening was only associated with cancer type among clinical and clinical variables (Table 2).

Comparison between cancer patients on secondary distress screening by Hospital Anxiety and Depression Scale (patients with <13 score versus patients with ≥13 score)
Relationship of refusal of psychiatric consultation service with demographic, medical, and psychosocial characteristics
The comparison between cancer patients who refused psychiatric consultation service and those who accepted the service is shown in Table 3. No demographic variable was related to refusal of psychiatric consultation service in cancer patient. However, refusal of psychiatric consultation service was associated with cancer type, metastasis, and reason to admission among medical and psychosocial variables (Table 3).
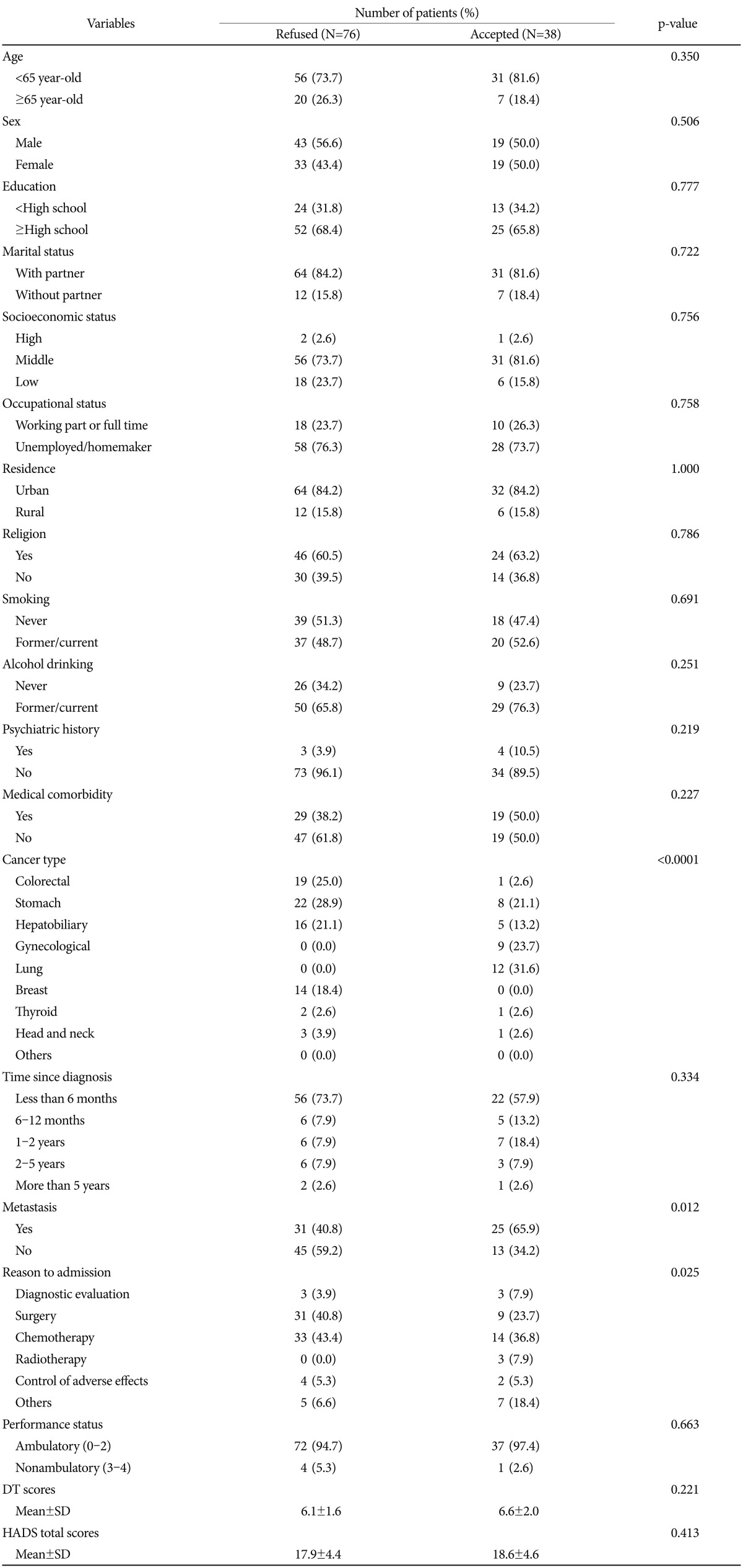
Comparison between cancer patients who refused and accepted a psychiatric consultation service among the positively screened patients (N=114) in the secondary distress screening
DISCUSSION
In this study, we developed a novel program of psychosocial distress-screening and intervention for hospitalized cancer patients and evaluated the feasibility of our program. Our study is not the first research to evaluate the feasibility of a novel intervention program to unburden psychosocial distress of cancer patients. However, we used a novel phased-approach to evaluate and treat inpatients with various types of cancer through cooperation between oncology and psychiatry teams. Since researchers could change the course of the trials while processing feasibility studies, we finished this study with the same procedure from the beginning to the end in a short period of time (1 month). All participants were hospitalized patients. Due to the nature of cancer diagnosis and treatment, almost all patients initially experienced admission for diagnosis and treatment. Therefore, oncology and psychiatric team could have enough time to conduct phased-approach distress screenings. Moreover, the medical team could be emphatic about the necessity of psychosocial distress assessment. Distress screening program through admission can facilitate psychiatric intensive care for patients who need the distress intervention. We tried to conduct primary distress screening on the admission day for all patients and to evaluate whether the distress at the time of psychiatric illness was aggravated. Based on the primary distress screening, psychiatrists, oncologists, nurses, psychologists, and social workers were involved in the assessment and treatment using various psychiatric interventions.
We found that DT and HADS could classify psychosocial interventions for cancer patients into the following three groups: distress education group, distress management group, and psychiatric consultation service group. The refusal rates to primary and secondary distress screening were 11.05% and 0%, respectively. The refusal rates to distress education, management, and psychiatric consultation service were 0%, 3.48%, and 66.67%, respectively. While patients with relatively lower distress tended to participant in psychosocial interventions for relieving patients' distress, patients with higher distress were inclined to refuse psychosocial intervention (psychiatric consultation service). Regarding the lower participation rate of the psychiatric consultation service, we agree to the explanations of Fukui et al.28 who have suggested that one of the reasons for lower level of Japanese psychosocial interventions might be due to cultural difference. Daneshpour and colleagues reported that discussing personal problems with someone outside of the family might bring a deep sense of shame in Asian countries.29 Korean people have similar tendency to be ashamed of their psychiatric diagnosis and treatment as well. In addition, since planned oncologic examinations and treatments could dominate patients who are recently diagnosed with cancer, intensive psychosocial intervention such as psychiatric consultation might be less important to the patients. In the oriental cultural point of view, the participation rate in psychiatric consultation service might be increased by more explanations and educations to the patients by the oncologic medical team about the importance of psychosocial distress control.
This feasibility study provided a lot of information about psychosocial evaluations and interventions of distress in patients with cancer. Table 1 showed the comparisons between cancer patients who were not distressed and those who were distressed using DT from the primary distress screening. Our results showed that psychosocial distress was associated with residence, cancer type, and reason to admission (Table 1). Table 2 showed the comparisons between cancer patients who had relatively lower distress and those who had higher distress using HADS from the secondary distress screening. Our results showed that psychosocial distress of cancer patients with high DT scores was associated with cancer type. On residence occasion, patients who resided in rural area tended to be less distressed than patients who lived in urban area. However, Weaver and colleague showed that cancer survivors who resided in rural areas were at greater risk of a variety of poor health outcomes. Therefore, recommendation of residence in rural areas where cancer patients were less distressed is controversial. In terms of cancer type, patients with hepatobiliary, lung, breast, and thyroid cancer tended to be more distressed than patients with stomach, gynecological, and head & neck cancer in primary distress screening (Table 1). Admiraal and colleague reported that patients with prostate cancer were significantly less distressed than patients with other cancer types.30 Linden and colleague also suggested that he levels of anxiety and depression varied widely by cancer type.31 Our results could be an extension of these previous studies. In secondary distress screening, breast cancer showed the same results as primary distress screening, which showed patients with breast cancer tended to suffer more psychological distress (Table 2). These findings may be caused by several clinical factors, such as cosmetic problem. However, Kwak and colleague32 showed dissimilar results. They reported that the cancer type was not associated with distress. In our study, the results of the primary and secondary distress screening were the same only for colorectal, breast, and head & neck cancer. Therefore, more studies are needed to determine the association between cancer type and psychosocial distress.
Several researchers showed that distress was significantly associated with poor performance status.1224 In consistent with this result, we also found that patients who were admitted for chemotherapy tended to be less distressful than patients who were admitted for diagnostic evaluation, surgery, or radiotherapy. Cancer patients experience considerable stress on chemotherapy.33 Especially, cancer patients were most distressful before the first chemotherapy. As chemotherapy was repeated, cancer patients experienced less distress.34 In this study, 10.2 percent of patients admitted for chemotherapy were hospitalized for the first time. And the rest of the patients have already experienced several cases of chemotherapy. However, we could not convince the reason why patients who were admitted for diagnostic evaluation, surgery, or radiotherapy tended to be more distressed than patients who were admitted for chemotherapy. Therefore, oncology and psychiatric team should be concerned about the reason to admission.
Table 3 showed the comparison between cancer patients who refused psychiatric consultation service and those who accepted psychiatric consultation service among positively screened patients in the secondary distress screening. Whether cancer patients refused or accepted the psychiatric consultation service was associated with cancer type, metastasis, and reason to admission. However, the distress level was not associated with the refusal to the psychiatric consultation service. These results suggested that clinical variables such as cancer type, metastasis, and reason to admission could be crucial factors influencing the decision on whether a psychiatric consultation service would be refused or accepted by cancer patients with considerable distress level (higher scores of the DT or HADS). Therefore, clinicians should consider various clinical factors, especially the cancer type, metastasis, and reason to admission.
The current study has some limitations. First, it might be difficult to generalize about all patients with cancer from our study because it was a cross-sectional study with small sample size. More research including longitudinal studies with larger sample size is needed to confirm our findings. Second, the current study was conducted at one institution which might lead to institutional bias. Therefore, our findings could be more generalizable after multi-institutional studies. Third, the refusal rate to psychiatric intervention (a psychiatric consultation service) was rather high. Although our findings showed that the distress level was not associated with the refusal rate, the cut-off score of HADS could be controversial.
In this study, we demonstrated a novel feasible phased-approach of distress screening and management program for hospitalized cancer patients. This strategy of using mutual cooperation between oncologist and psychiatrist could increase the awareness to psychosocial distress experienced by cancer patients amongst medical team, cancer patients, and their caregivers. Follow-up studies on the clinical effectiveness of this strategy through realistic and optimal modifications are warranted.
Acknowledgments
This work was supported by the Basic Science Research Program through the National Research Foundation of Korea funded by the Ministry of Education, Science and Technology (2010-0003505) and by the Catholic Medical Center Research Foundation made in the program year of 2014.