Mediating Effect of Resilience on the Association between Emotional Neglect and Depressive Symptoms
Article information
Abstract
Objective
Previous studies have reported that childhood maltreatment experiences could induce biological and psychological vulnerability in depressive disorders. However, it is still unclear that type-specific effects of childhood maltreatment on psychological resilience, depressive symptoms and interactions among childhood maltreatment experiences, resilience, and depressive symptoms.
Methods
A total of 438 medical students were included in the study. The Childhood Trauma Questionnaire-Short Form, the Conner-Davidson Resilience Scale, and the Beck Depression Inventory were used for measuring childhood maltreatment experiences, psychological resilience, and depressive symptoms, respectively. We investigated the effects of childhood maltreatment experiences on resilience and depressive symptoms using correlation analysis. In addition, we analyzed the mediating effect of resilience on the association between childhood maltreatment and symptoms of depression.
Results
Among childhood maltreatment, emotional neglect was a significant predictor of the scores of low resilience and high depressive symptoms in both gender groups (all ps<0.05). Furthermore, resilience was found to be a mediator connecting emotional neglect experiences with depressive symptoms.
Conclusion
Our results suggest that emotional neglect has detrimental effects on mood and resilience, and clinicians need to focus on the recovery of resilience when they deal with depressive symptoms in victims of childhood maltreatment.
INTRODUCTION
Experiences of childhood maltreatment (CM) are closely linked with various adult psychopathologies.12 Among various psychiatric disorders, major depression is one of the most common diseases related to CM. CM negatively affects the lifetime risk as well as the course of depression.34 Patients with depression and childhood maltreatment reported recurrent and persistent episodes of depression and low response to treatment for depression.3
CM could induce biological and psychological vulnerability in depression. Even in preclinical samples, abusive experiences damage the brain structure and function related to emotion processing. The main fiber tracts linking prefrontal and subcortical regions are altered by experiences of emotional abuse.56 CM experiences induce hyper-reactivity of the amygdala to negative emotional stimuli.789101112 Furthermore, aberrant functional connectivity between the ventromedial prefrontal cortex and the amygdala were reported in subjects with CM experiences.1213 Moreover, CM increases maladaptive psychological and behavioral problems, such as unusual aggression, low self-esteem, withdrawal from family and friends, and self-destructive behaviors.14 Therefore, these biological and psychological changes make the victims of CM more vulnerable to mood problems.
Although a relationship between CM and depression has been established, the role of psychological resilience on the onset and course of depression is still unclear. The term “resilience” has begun to attract attention because recent studies reported protective effects of psychological resilience on aggravation of psychiatric symptoms in subjects with CM experiences including post-traumatic stress disorder, depression, and suicidal behaviors.151617181920 However, to the best of our knowledge, only three studies reported moderating effects of resilience on depressive symptoms,152122 and differential effects between types of CM were not evaluated in these studies. The effects of CM on depressive symptoms and resilience can be differed among types of CM. While all types of CM are involved in the development of depression,2123 several studies represented that emotional abuse and neglect have a close relationship with depressive symptoms than other types of abuse.2425 In addition, only emotional abuse, emotional neglect and sexual abuse showed negative relationship with resilience.26 Therefore, further investigation is needed to understand type-specific effects of CM on psychological resilience, depressive symptoms and interactions among CM, resilience, and depressive symptoms.
In this study, we aimed to clarify the effects of CM on resilience and depressive symptoms. In addition, we verified whether the CM type-specific effect exists. In addition, we analyzed the mediating effect of resilience on the association between CM and symptoms of depression. We assumed that the CM experiences, especially emotional type of CM, have negative effects on psychological resilience and depressive symptoms, and low resilience could lead the victims of CM to a depressive state.
METHODS
Participants
All subjects were graduate medical students at the Kyungpook National University School of Medicine in South Korea. The Kyungpook National University School of Medicine conducted mental health assessment for students annually from 2009, and the data used in this study were drawn from first- and third-year students in 2012 and 2013. Among 440 students, 2 subjects were excluded from our analysis due to missing values. Therefore, in the final analysis, the data of 438 graduate students [265 male subjects and 173 female subjects; mean age (SD)=25.2 (2.5) years] were included. All subjects voluntarily participated and provided written consent, and this study was approved by the Ethics Committee of the Kyungpook National University School of Medicine (IRB No. 2013-05-026-001).
Measures
Childhood Trauma Questionnaire-Short Form
The Childhood Trauma Questionnaire-Short Form (CTQ-SF) is a self-report questionnaire with 28-items developed to assess the severity of 5 types of maltreatment experiences, such as emotional abuse, physical abuse, sexual abuse, emotional neglect, and physical neglect during childhood and adolescence. 27 The severity of each maltreatment experience is measured through a 5-point, Likert-type scale ranging from never true (score=1) to very often true (score=5). The CTQ-SF showed good to excellent internal consistency both in clinical and community samples.2728 In this study, the Korean version of CTQ-SF was applied to assess the subjects' maltreatment experiences. The Korean version of CTQ-SF represented excellent internal consistency (Cronbach's alpha>0.9) and high test-retest reliability (Pearson r>0.8).29
Conner-Davidson Resilience Scale
The Conner-Davidson Resilience Scale (CD-RISC) is a questionnaire to evaluate psychological resilience related to coping skills on stressful events.30 This questionnaire consists of 25-items, and each item is rated using a self-reported 5-point scale (0 to 4). A higher score indicates greater psychological resilience. In factor analysis, the CD-RISC was divided into 5 sub-factors: hardness, persistence, optimism, support, and being spiritual. High reliability and validity of CD-RISC has been confirmed in a community sample, primary care patients, and psychiatric patients.30 The Korean version of CD-RISC was developed in 2010 with excellent internal consistency (Cronbach's alpha>0.9) and high test-retest reliability (Pearson r>0.9) in samples comprising university students, nurses, and firefighters.31 Furthermore, reliability and validity were verified in another study with general population and psychiatric outpatients.32
Beck Depression Inventory
Depressive symptoms in the subjects were measured using the Beck Depression Inventory (BDI). The cognitive, behavioral, affect, and somatic components of depressive symptoms are included in the BDI, a 21-item, self-report questionnaire.33 Using the BDI, the intensity of depressive symptoms in the week before the examination was measured. The Korean version of the BDI was standardized and showed a good internal consistency in depressed group (Cronbach's alpha=0.85).34
Statistical analysis
To evaluate effect of CM on depressive symptoms, our subjects were divided into two groups based on median score of CTQ-SF (high CM and low CM). T-test was used to measure the differences in scores of BDI between high CM and low CM groups. Also, binary logistic regression analysis was conducted to assess the differences in risk of clinically significant depressive symptoms (the scores of BDI 16 or above) between two groups. Also, we checked normality of the data using skewness and kurtosis. To assess the relationships between current depressive symptoms, resilience, and childhood trauma experiences, partial correlation analysis was applied (covariate: gender). In addition, multiple regression analysis was used to investigate the effects of each maltreatment experience on depressive symptoms and psychological resilience because various maltreatment experiences could influence each other. We analyzed the whole group after controlling for gender as well as male and female groups to evaluate the gender effects in multiple regression analysis. SPSS software (version 18; SPSS Inc., Chicago, IL, USA) was used in these analyses.
In addition, mediation analysis using structural equation modeling (SEM) was performed to determine the associations between childhood trauma experiences, resilience, and depressive symptoms. Based on the results of multiple regression analysis, we selected the independent variable (childhood trauma experiences) that is a significant predictor of the dependent variable (depressive symptoms) and the mediator (resilience), respectively. The mediating effects of resilience on predicting depressive symptoms using traumatic childhood experiences were evaluated using SEM analysis. Furthermore, an additional analysis including gender effects as a covariate was conducted. The significances on SEM analysis were supported by 1,000 times bootstrapping. AMOS software (version 18; SPSS Inc.) was applied for mediation analysis.
RESULTS
Group comparison analysis and Normality test
High CM group showed high scores of BDI compared to low CM group (7.4 in high CM and 4.9 in low CM groups, p<0.001). Also, high CM group represented high chance to have clinically significant depressive symptoms (odds ratio=3.82, 95% CI=1.50–9.71, p=0.005). In normality test using skewness (S) and kurtosis (K), several data represented highly skewed results [Emotional abuse: 2.8 (S) and 12.2 (K); Emotional neglect: 1.3 (S) and 2.2 (K); Sexual abuse: 5.4 (S) and 35.0 (K); Physical abuse: 3.4 (S) and 15.1 (K); Physical neglect: 1.0 (S) and 0.1 (K); CD-RISC: -0.4 (S) and 1.6 (K); BDI: 1.7 (S) and 4.4 (K)]. Therefore, we conducted additional analyses using transformed data applying natural logarithm transformation, and transformed data showed better results in skewness and kurtosis (except CD-RISC) (Supplementary Materials in the online-only Data Supplement).
Correlation analysis
In correlation analysis, childhood maltreatment experiences, except sexual abuse, have significant positive relationships with depressive symptoms in both genders (all ps<0.05). Experiences of physical abuse experiences in men and emotional abuse in women showed significant relationship with low resilience and high depressive symptoms (all ps<0.05). Among childhood maltreatment experiences, emotional neglect represented high correlations with total scores, scores of subscales (except spiritual) of CD-RISC, and the scores of the BDI in both genders (all ps<0.01). Detailed results are described in Table 1.
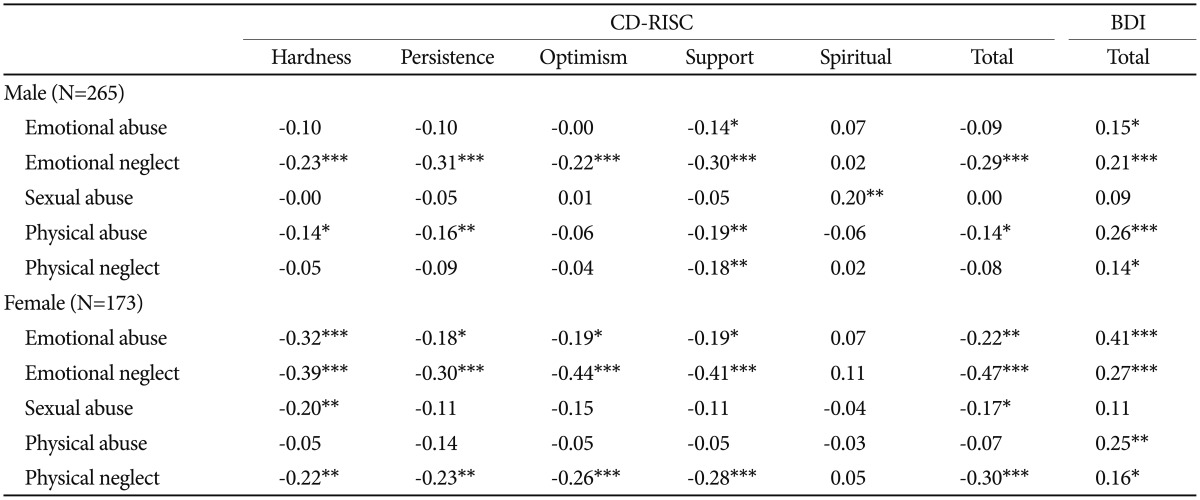
Pearson correlation coefficients among traumatic childhood experiences, resilience, and depressive symptoms
Multiple regression analysis
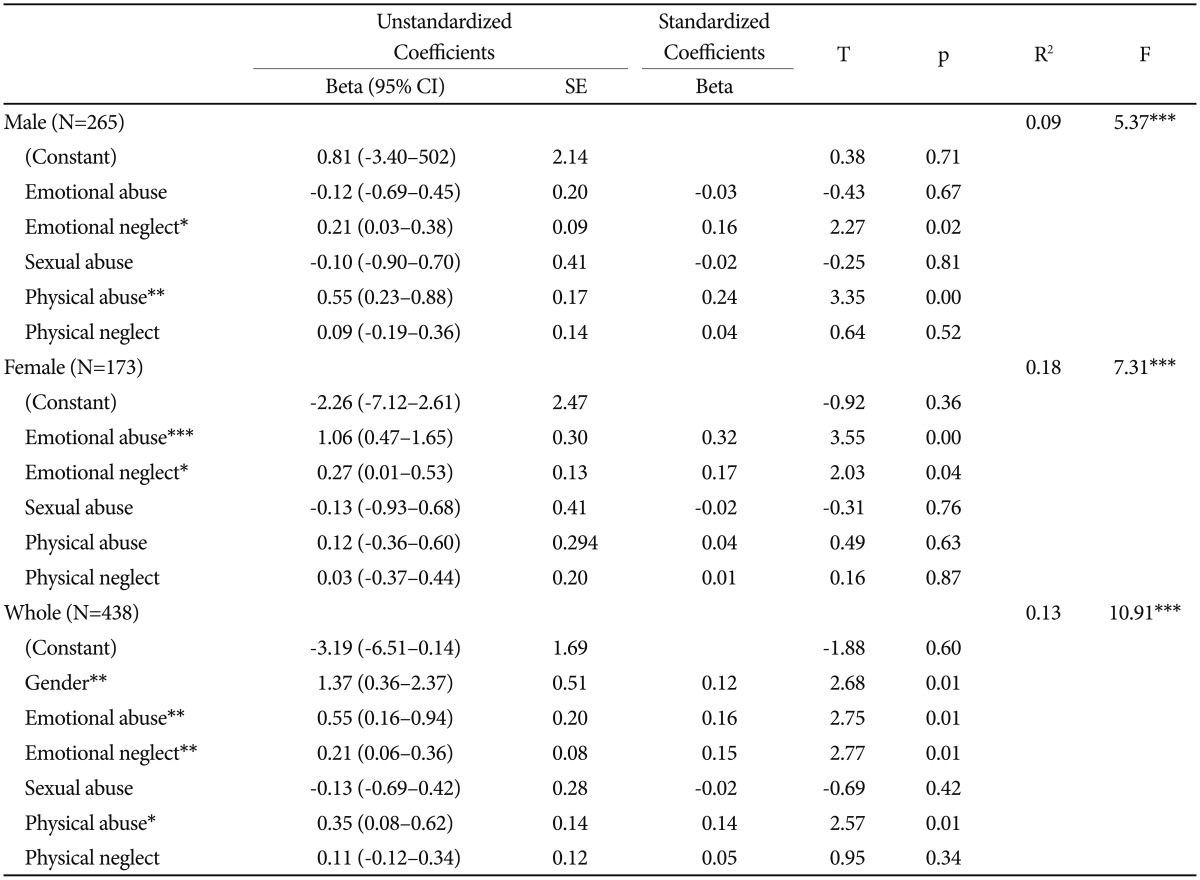
Emotional neglect was a significant predictor for low CD-RISC scores after adjusting for the effects of other types of maltreatment in male subjects, female subjects, and all groups (all ps<0.001). Furthermore, physical abuse was negatively associated with the scores of CD-RISC in the male group (p<0.05) (Table 2).
Multiple regression analysis for explaining resilience scores (CD-RISC) using the quantity of abusive experiences in male group, female groups, and all groups
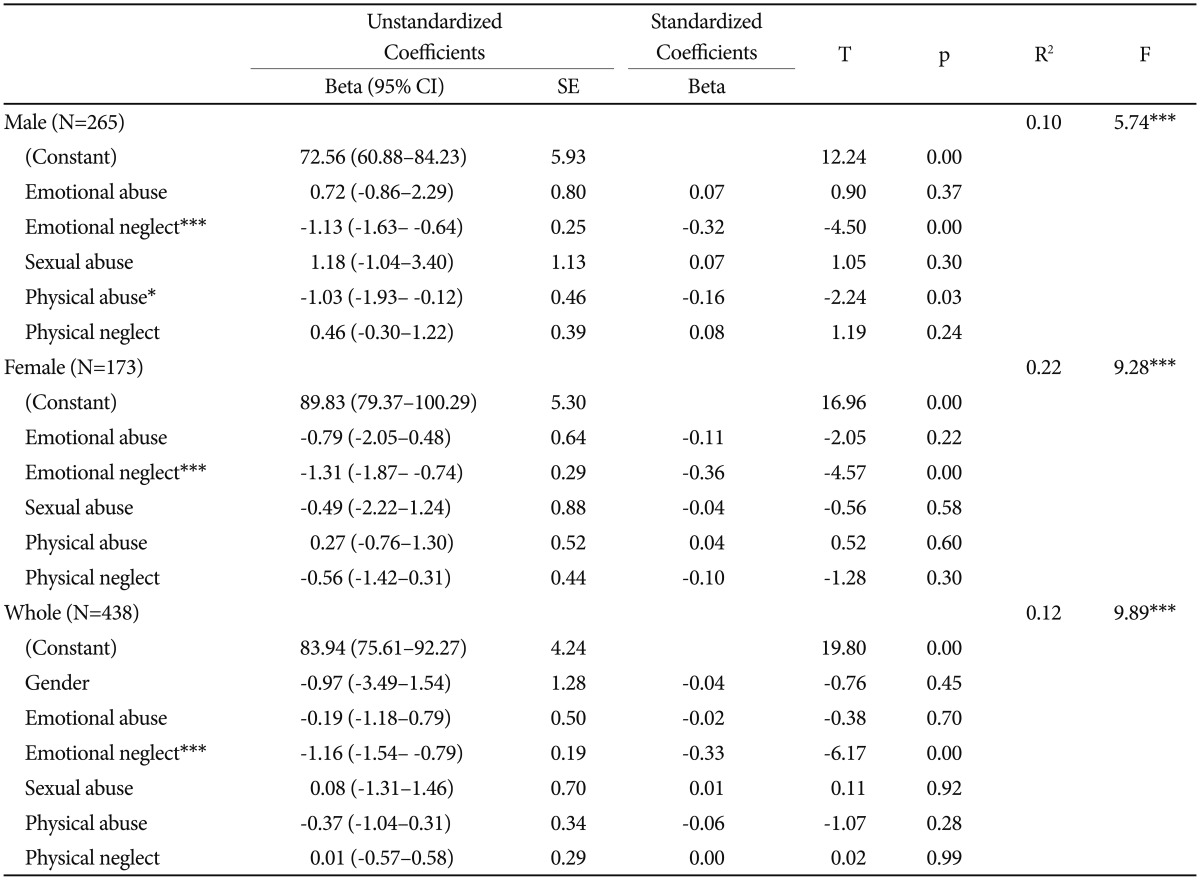
In addition, we observed that the higher the scores for emotional neglect were, the greater were the depressive symptoms in both male and female groups (all ps<0.05). While physical abuse experiences were a significant predictor of depressive symptoms in the male group (p<0.01), the female group represented significant effects of emotional abuse, and not physical abuse, on depressive symptoms (p<0.001) (Table 3).
Multiple regression analysis for explaining depression scores (BDI) using the quantity of abusive experiences in male group, female group, and all groups
To compensate distribution issues, we conducted additional multiple regression analysis using values that were transformed using natural logarithm, and the results were similar with analysis using raw data (Supplementary Table 1 in the online-only Data Supplement).
Mediation analysis using structural equation modeling (SEM)
The scores of emotional neglect were selected as independent variables in mediating regression analyses because emotional neglect had a significant relationship with low resilience and high depressive symptoms both in male and female groups. The scores of emotional neglect significantly predicted the scores of depressive symptoms and those of resilience (all ps<0.001). However, a significant path connecting emotional neglect and depressive symptoms disappeared in the analysis with no covariate or decreased (p<0.05) in the analysis with gender covariate when the mediating effects of resilience were included in the SEM analysis (Figure 1). In the model with gender covariance, standardized direct effect of emotional neglect on the depressive symptoms was 0.09 (95% CI=0.00–0.19, p<0.05); standardized indirect effect of resilience on depressive symptoms was 0.14 (95% CI=0.10–0.19, p=0.001). The model represented perfect fit indices since the model was saturated [χ2(0)=0.00, GFI=1, CFI=1, NFI=1].
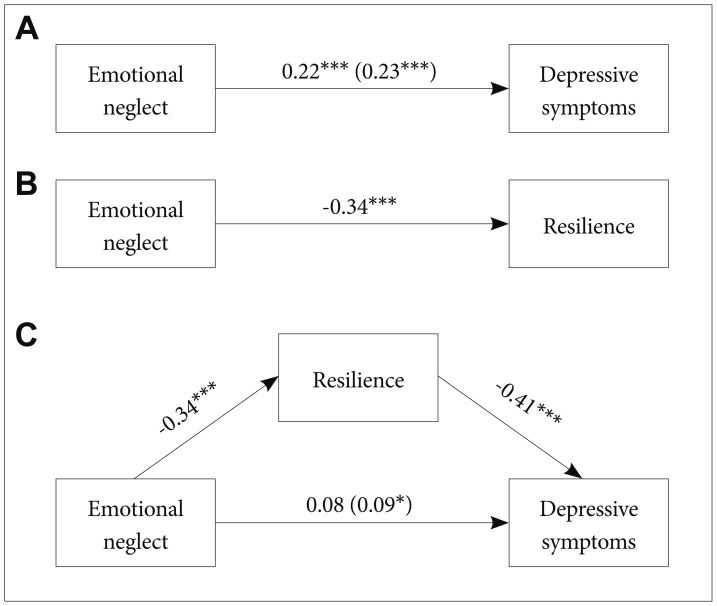
The mediating effect of resilience on the relationship between previous emotional neglect experiences and current depressive symptoms. (A) and (B) represent a direct effect of emotional neglect on depressive symptoms and resilience, respectively. The mediating effect of resilience is shown in (C). The changed values after controlling for gender were described within the bracket. Total scores of CD-RISC and BDI are used for resilience and depressive symptoms, respectively. *p<0.05, ***p<0.001. CD-RISC: Connor-Davidson Resilience Scale, BDI: Beck Depression Inventory.
We conducted additional SEM analysis using values that were transformed using natural logarithm, and the results were similar with analysis using raw data (Supplementary Figure 1A in the online-only Data Supplement). It was also examined whether measurements were similar across the types of abuse. Physical abuse in male and emotional abuse in female were selected since significant relationships with current depressive symptoms were reported in multiple regression analysis. Indirect effects of resilience on depressive symptoms were significant in both physical abuse in male and emotional abuse in female (Supplementary Figure 1B and C in the online-only Data Supplement).
DISCUSSION
Our results showed that CM experiences are significantly related to psychological resilience and depressive symptoms. Among various CM experiences, emotional neglect is a consistent and significant factor for predicting low scores of resilience and high scores of depressive symptoms in both genders. In addition, we found that resilience could be a mediator in connecting emotional neglect experiences with depressive symptoms. These results suggest that emotional neglect, which is an easily neglected form of CM, has considerable effects on psychological resilience that can lead people to depression.
While child neglect is the most prevalent type of CM, its effects seem to be neglected in previous studies. Category of neglect had the highest percentage (about 60%) of CM experiences in the United States.35 In a recent meta-analysis, the overall estimated prevalence rates were 16.3% for physical neglect and 18.4% for emotional neglect.36 Emotional neglect is characterized by the acts ignoring the child's basic emotional needs, such as insufficient or no emotional interaction between parents and the child.37 The consequences of emotional neglect should not be overlooked. Emotional neglect experiences were strongly linked with symptoms of anxiety, depression, and suicidal attempt in recent meta-analysis.38 Also, several recent studies try to discover the possible mediators between emotional neglect and depression. In college students, emotional neglect was related to symptoms of depression, anxiety, and depression and was mediated by specific schemas including shame.39 Dysfunction in ventral striatum40 and specific emotional regulation strategy, such as behavioral avoidance41 can be mediators between emotional neglect and depression. Also, the neglect experiences can be associated with a risky sexual behavior,42 a diminished economic well-being,43 a dysfunctional attachment style,44 and an increased violence risk.45
In our results, only emotional neglect was a consistent and significant factor showing relationships with low resilience scores and high depressive symptoms scores in both genders. There were two possible explanations for these results. First, the medical school is considered one of the most competitive departments for admission in South Korea. Previous studies reported CM experiences could lead to impaired school performance including low grade point average.4647 Adolescents with CM experiences, mostly, physical abuse or sexual abuse, showed lower neurocognitive functioning.48 Severe physical abuse experiences was associated with low education years.49 Therefore, severe cases of CM might be excluded from our samples. We could predict the prevalence rates of CM using original cutoff scores for “moderate to severe” exposure.50 In our study, emotional neglect (7.8%) and physical neglect (14.2%) were the two most common types of CM (physical abuse: 6.2%, sexual abuse 3.4%, and emotional abuse: 0.7%). Although population based studies reported large variation in prevalence rates of CM experiences,51 overall prevalence rates of CM experiences were relatively low in our study compared to other previous studies.52535455 In recent studies using meta-analysis, the overall estimated prevalence rates were 12.7% for sexual abuse,56 26.7% for emotional abuse,57 and 17.7% for physical abuse.58 Also, CTQ-SF scores of physical abuse, sexual abuse, and emotional abuse showed high skewness and kurtosis in normality test. Therefore, our subjects' characteristics may have affected our results. Second, the emotional type of CM could have dominantly affected depressive symptoms. Emotional type of CM has been reported to have a close relationship with depressive symptoms than other types of abuse.2425 Emotional abuse and neglect were significant predictors of depressive disorders after controlling for sexual and physical abuse in psychiatric outpatients.25 The effects of emotional abuse could be underestimated due to the very low prevalence (0.7%), and finally, emotional neglect appears as a significant factor while the prevalence of physical neglect was relatively high. In our study, female reported significantly high scores in emotional abuse experiences compared to male (t=−3.37, p=0.001), and emotional abuse experiences were important factors related to low resilience and high depressive symptoms in female. These results support the effect of emotional type of CM on depressive symptoms.
Furthermore, the results of mediation analysis showed resilience may have mediating effects on the association between CM and depressive symptoms. The meaning of resilience is rather vague and hard to define in a sentence. Resilience is a multidimensional construct containing the meaning of the capacity for, the process of, or the outcome of successful adaptation despite threatening circumstances.59 Resilience can be the process of effectively mobilizing individual and environmental resources to manage in the face of distressful or traumatic events.60 Our results represented that CM experiences might inhibit the growth of individual resilience, and low resilience might mediate depressive symptoms related to CM. A recent study suggests that resilience could be a protective factor against developing major depressive disorder in patients with CM experiences and even in subjects without CM experiences.21 Our results suggest that increasing resilience can be an important factor to prevent or treat depression in patients with CM experiences.
There are several limitations of the study to be considered. First, our study is a cross-sectional design. Mediation analysis is more acceptable for prospective studies than cross-sectional studies, and our results could not determine a definite causal relationship among CM, resilience, and depressive symptoms. The results should be interpreted in a cautious manner. However, our results could inform future studies on the effects of CM on resilience and depressive symptoms. Second, only medical students were included in our study. High level of intellectual functioning may be related to high resilience, 61 and our samples represented low rate of CM experiences. Therefore, our results are hard to generalize. However, there is a lack of study considering the effects of emotional neglect and its relationship with resilience. Also, our results suggest that the need for careful investigation about emotional neglect experiences in highly-educated group. Furthermore, in medical students, depressive symptoms are highly prevalent, and it could be related to functional impairment in professional and academic skills.62 Medical students may be reluctant to seek care due to fear of academic jeopardy63 or concerns about confidentiality.64 Therefore, considering the influence of physicians on our health care system, verifying the effects of CM on psychological resilience and depressive symptoms in medical students can be important. Third, the scores of CTQ-SF were measured based on autobiographical memory that could be easily biased in case of traumatic events.65 Also, depressive subjects tend to focus on negative memory, and negatively appraise previous experiences.6667 Further studies with prospective and population-based design are needed to compensate our limitations.
Despite these limitations, our study showed the detrimental effects of emotional neglect on resilience and how resilience mediate the association between CM experiences and depressive symptoms. These results indicate the need for a careful consideration of emotional neglect experiences and providing increased attention to enhancing resilience for alleviating symptoms of depression.
Acknowledgments
This research was supported by Kyungpook National University Research Fund, 2015.
References
Supplementary Materials
The online-only Data Supplement is available with this article at https://doi.org/10.4306/pi.2018.15.1.62.
Supplementary Materials
Supplementary Figure 1
The mediating effect of resilience on the relationship between previous abuse experiences and current depressive symptoms. (A) Natural logarithm transformed data were applied except CD-RISC. The changed values after controlling for gender were described within the bracket. Indirect effects of resilience on depressive symptoms were significant in both physical abuse in male (B) and emotional abuse in female (C). Total scores of CD-RISC and BDI are used for resilience and depressive symptoms, respectively. *p<0.05, **p<0.01, ***p<0.001. CD-RISC: Connor-Davidson Resilience Scale, BDI: Beck Depression Inventory.
Supplementary Table 1
Multiple regression analysis for explaining resilience scores (CD-RISC) and depression scores (BDI) using the quantity of abusive experiences