Factors Associated with Emotional Exhaustion in South Korean Nurses: A Cross-Sectional Study
Article information
Abstract
Objective
We examined associations between emotional exhaustion and selected sociodemographic and psychological factors among nurses in inpatient and outpatient nursing units at a university hospital in South Korea.
Methods
The participants were 386 nurses who completed the Maslach Burnout Inventory, a measure of emotional exhaustion. Psychological characteristics were evaluated, including hardiness, self-esteem, experience of trauma, resilience, perceived stress, and social support. Correlation analyses examined the relationships between emotional exhaustion with sociodemographic, occupational, and psychological characteristics. Linear regression was used to evaluate the associations between emotional exhaustion and the assessed characteristics.
Results
Higher emotional exhaustion scores were associated with greater depression, anxiety, traumatic experience, and perceived stress. Exhaustion was inversely associated with hardiness, self-esteem, resilience, and quality of life. The regression analysis indicated that gender, marriage, resilience, depression, perceived stress, and secondary traumatic stress were significantly associated with emotional exhaustion.
Conclusion
This study showed that psychological characteristics, such as resilience, depression, and secondary traumatic experiences, may cause emotional exhaustion. Understanding the needs of people with distinct demographic and psychological characteristics offers valuable direction for the development of intervention programs to prevent burnout among nurses.
INTRODUCTION
Burnout has been defined as a psychological state resulting from prolonged emotional or psychological stress on the job [1]. Burnout has been found to impair workers’ ability to regulate negative emotions [2] and to function at work [3]. Health professionals, especially nurses, are known to be at higher risk for the development of burnout than are those in other occupations [4,5]. Previous studies showed that 30–50% of nursing personnel experience clinical levels of burnout [4,6,7].
Large numbers of studies have evaluated factors related to burnout in nurses, as burnout has a significant impact not only on nurses’ well-being but also on the quality of healthcare [8]. Burnout negatively affects nurses’ work performance, patient safety [6], and patient satisfaction [9]. Previous studies related to burnout among nurses have examined occupation-related factors, such as job overload, conflicts of responsibilities, monotonous work, and the pressure of time limits. Demographic characteristics have also been relatively well studied [10]. However, most previous research focused on factors related to the work environment and demographic factors that are difficult to change.
Burnout could be defined as a psychological state resulting from emotional stress, and associated psychological characteristics associated with emotional exhaustion could be crucial determinants of burnout. Emotional exhaustion is a chronic state of physical and emotional depletion that results from excessive job and/or personal demands and continuous stress [11]. Emotional exhaustion in nurses could be prevented with prevent proper interventions if the psychological factors associated with burnout are known. Despite the importance of nurses’ psychological backgrounds in relation to burnout, few studies on this topic have been conducted.
Recent research has shown a link between resilience and burnout [12,13], and resilience appeared to be protective against emotional exhaustion [14]. Additionally, a previous study showed that self-esteem and exhaustion were inversely correlated [15]. Moreover, secondary traumatic experiences caused by repetitive demands for compassion could affect emotional exhaustion [16]. These findings imply that several psychological factors could affect exhaustion in nurses.
Emotional exhaustion is considered to have high predictive value in anticipating the impact of stress on health in the active work population [1]. Therefore, we focused on the association between psychological correlates and emotional exhaustion. The present study explored the hypothesis that the level of emotional exhaustion is influenced by the psychological characteristics of the study population. Specifically, greater resilience, self-esteem, and hardiness are hypothesized to be inversely related to emotional exhaustion. In contrast, higher scores for depression, traumatic experiences, and stress are expected to result in greater exhaustion. Furthermore, we hypothesized that the psychological characteristics associated with burnout could significantly explain exhaustion.
METHODS
Participants
Informed consent was obtained from all study participants. The study enrolled 386 nurses (13 men and 373 women) with a mean age of 30.10±7.26 years. The study included all nursing personnel who worked in the hospital’s inpatient and outpatient units (intensive care unit, intermediate care unit, operating room, recovery room, general ward, emergency department, and outpatient unit) and who were willing to participate in the study. This study and all protocols were approved by the Institutional Review Board and Ethics Committee of Soonchunhyang University Hospital (IRB number: 2015-05-013). The study was performed in accordance with approved guidelines.
Psychological measures
To assess emotional exhaustion, the Maslach Burnout Inventory-General Survey (MBI-GS) was administered [1,17]. The MBI is the gold standard for detecting burnout. Furthermore, it has been shown to perform adequately and have a stable factorial structure among nurses from different populations and in varied contexts [18]. The MBI-GS, a 16-item questionnaire designed to assess the presence of burnout in healthcare providers, contains 3 subscales, each evaluating 1 of the underlying constructs of burnout: emotional exhaustion, depersonalization, and personal achievement. Each subscale comprises several items, and each of these is rated by the respondent on a 7-point Likert scale according to the frequency of their occurrence (0=‘‘Never’’ to 6=‘‘Every day’’). The Professional Quality of Life (ProQOL) scale is the most commonly used measure of the negative and positive affects of helping others who experience suffering and trauma. The ProQOL has sub-scales for compassion satisfaction, burnout and compassion fatigue [19].
To evaluate hardiness, the 15-item Hardiness Scale was applied. Hardiness has been found to be a stress/health moderator [20]. To measure the severity of depressive and anxiety symptoms, the Patient Health Questionnaire (PHQ) and Generalized Anxiety Disorder 7 (GAD-7) scale were used [21,22]. The Davidson Trauma Scale, which is composed of 18 items, is a commonly used measure of traumatic experiences. To assess secondary traumatic stress, a secondary traumatic stress scale was administered. Secondary traumatic stress has been defined as “the natural, consequent behaviors and emotions resulting from knowledge about a traumatizing event experienced by a significant other” [23]. The scale consists of 17 items. The 25-item Connor-Davidson Resilience Scale, which measures individual resilience in the face of stressful events, was developed and evaluated. To assess individual stress, the 10-question Perceived Stress Scale (PSS) was applied [24]. The Rosenberg Self-esteem Scale was used to measure self-esteem in this study [25]. The scale has 10 items, which are answered using a 4-point Likert scale. To evaluate quality of life among nurses, the 16-item World Health Organization Quality of Life Scale-Abbreviated Version (WHOQOL-BREF) was administered [26]. The Duke-UNC Functional Social Support Questionnaire (FSSQ), a 14-item, self-administered, multidimensional questionnaire, was used to assess functional social support [27]. The higher an individual’s score is, the lower the level of social support.
Statistical analysis
Descriptive data showed that nurses in this population were distributed across various categories of hospitals, which are defined by staffing levels. Correlation analyses were performed to determine the relationships between emotional exhaustion with sociodemographic, occupational, and psychological characteristics, the 3 main dimensions of burnout measured by the MBI [5]. There is a general consensus in the literature that emotional exhaustion is the central or core dimension of burnout [28,29]. Comparative analysis between the high- and low-exhaustion groups in this study was conducted using an independent t-test. The cutoff for MBI scores indicating emotional exhaustion was applied to divide participants into 2 groups. Linear regressions were calculated to evaluate factors related to emotional exhaustion as a dependent variable.
RESULTS
Psychological measures
A total of 386 nurses/nurse assistants completed the survey. They were predominantly female (96.6%) and had a mean age (standard deviation) of 30.1 (7.3) years. Table 1 shows the sociodemographic and occupational characteristics of the study population, and Table 2 shows the psychological characteristics of all study participants.
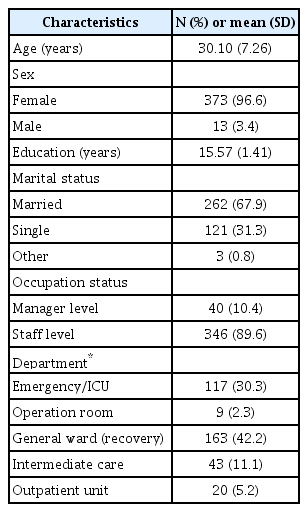
Sociodemographic and occupational characteristics of study participants (N=386)
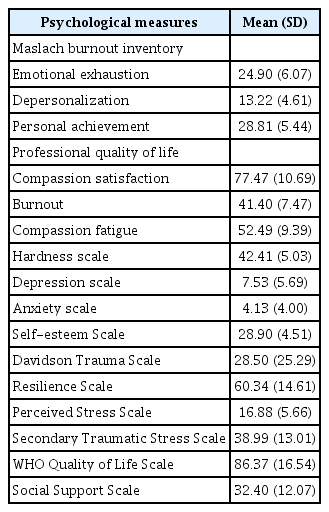
Psychological characteristics of participants
Correlation analysis
Table 3 presents the correlations between the MBI and emotional exhaustion (subscale of MBI), burnout (Professional Quality of Life subscale of the WHOQOL-BREF), and psychological measures. Emotional exhaustion scores were positively correlated with depression, anxiety, traumatic experience, perceived stress, and social support. Exhaustion was inversely correlated with hardiness, self-esteem, resilience, and quality of life.

Correlations between burnout and psychological measures in the participants
Comparison between high- and low-exhaustion participants
Table 4 shows the comparisons of demographic and psychological characteristics between participants in the low- and high-exhaustion groups. In the high-exhaustion group, the ratio of women to men was higher than that in the low-exhaustion group (p=0.04). Scores on the depression, anxiety, Davidson Trauma, Connor-Davidson Resilience, perceived stress, secondary traumatic stress, and social support measures were significantly increased in the high-exhaustion compared with the low-exhaustion group (higher social support scores indicated lower social support). The high-exhaustion group showed reduced hardiness, Rosenberg Self-esteem, and WHO Quality of Life scores compared with the low-exhaustion group.
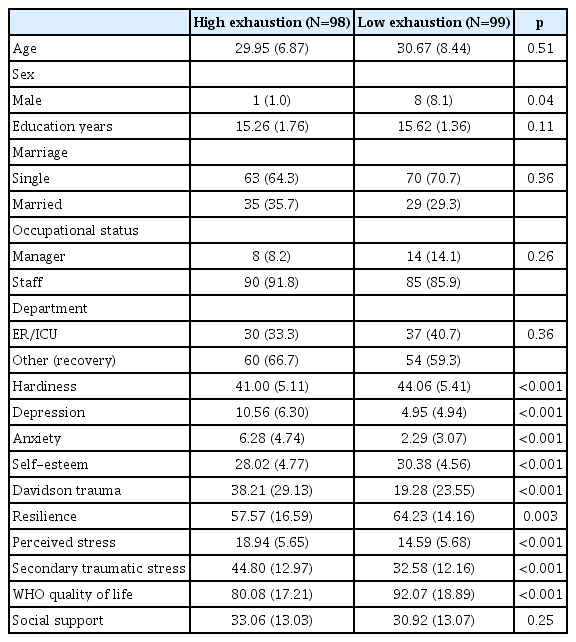
Comparison between high and low exhaustion participants
Regression analysis
Table 5 presents the multiple linear regression coefficient (β) values for the relationships of emotional exhaustion, measured by an MBI subscale, with sociodemographic, work-related, and psychological characteristics. Demographically, emotional exhaustion was independently associated with female gender (p=0.03) and being married (p=0.01). Furthermore, emotional exhaustion was associated with several psychological factors. It was inversely associated with resilience (p=0.03) and positively associated with depression (p<0.001), perceived stress (p=0.04), and secondary traumatic stress (p=0.004). The adjusted R2 for the regression model was 0.40.

Linear regression coefficient (β) for the scores of exhaustion by socio-demographic and psychological characteristics
DISCUSSION
In the present study, several sociodemographic and psychological factors were associated with emotional exhaustion among nursing personnel. Further, each dimension of burnout was associated with different sociodemographic and occupational characteristics. As we hypothesized, the level of emotional exhaustion was associated with psychological characteristics of the study population.
We found an association between gender and exhaustion, although this analysis was limited by the small number of male nurses (n =9). Previous studies of nurses have reported conflicting results regarding the relationship between gender and exhaustion [8,30,31]. These differences may indicate that these associations are confounded by occupational role, hierarchical position, and other occupation-related factors [1,32].
In our regression analysis, being married was associated with greater emotional exhaustion. It has been reported that being married may result in greater responsibilities/time demands, which induce family–work conflicts and thereby increase the risk of exhaustion [33,34]. Additionally, studies conducted with civilian nurses have reported that having children is positively associated with burnout, likely because parenting creates additional responsibilities and contributes to family-work conflicts [33,34]. In contrast, other studies have reported that being married was not associated with exhaustion [30,35]. Further studies will be needed to resolve these discrepancies.
Contrary to expectations, we found no significant differences in emotional exhaustion between recovery room and emergency department/intensive care unit (ED/ICU) nurses. Previous studies showed that nurses working in the ED/ICU displayed greater emotional exhaustion than did nurses working in the recovery room. Those authors suggested that this was because the recovery room had fewer patients who were usually more stable and had better prognoses [8]. A partial explanation for our non-significant results may be that our recovery room sub-population was different from that in the previous study. Further studies are needed to clarify this relationship.
As hypothesized, comparison of the high- and low-exhaustion groups showed that resilience, self-esteem, and hardiness were inversely related to exhaustion. In contrast, depression, anxiety, traumatic experiences, and stress were associated with greater exhaustion. Furthermore, we hypothesized that psychological characteristics such as resilience, depression, perceived stress, and secondary traumatic experiences, which were associated with burnout among nurses, could significantly explain exhaustion. The present study showed that greater resilience was associated with reduced emotional exhaustion. This result was in agreement with previous reports [36,37]. Of even greater importance, resilience significantly predicted emotional exhaustion in our regression analysis. A recent study evaluating the relationship between resilience and burnout showed that resilience was a useful predictor of emotional exhaustion [36].
Our study revealed that conditions such as depression and anxiety were also related to greater emotional exhaustion. Similarly, emotional exhaustion was associated with greater health problems in the form of anxiety and depression [38]. Indeed, depression was the strongest predictor of emotional exhaustion in our regression analysis. A previous structural equation modeling study by Glass and colleagues concluded that a perceived lack of job control may indirectly drive depression by means of emotional exhaustion [39]. A literature review noted that depression and burnout are distinct concepts, and the causal relationship between them remains unclear [40]. Although the present study showed that depressive symptoms may predict emotional exhaustion, other studies have concluded that burnout can serve as a predictor of depressive symptoms in work life [41,42]. Longitudinal studies are needed to clarify the causal relationship between depression and burnout.
Our analysis related to hardiness and self-esteem was consistent with previous reports, which found that both were negatively associated with emotional exhaustion [15,38,43]. Self-esteem and hardiness may play a role in buffering or protecting against exhaustion, but a direct causal role cannot be demonstrated by our correlational and comparative analyses.
A systematic review showed that nurses were highly likely to experience secondary traumatic stress and compassion fatigue related to their work [44]. Stebnicki and colleagues explained that nurses’ everyday practice predisposes them to being “wounded by their work,” as they routinely deal with their patients’ suffering, trauma, serious illness, and death [45]. In our results, both early traumatic experiences (Davidson Trauma Scale) and secondary traumatic experiences were associated with emotional exhaustion. Interestingly, only secondary traumatic experiences directly explained emotional exhaustion in our regression analysis. The dominant theoretical model regarding the emergence of compassion fatigue draws on a stress–process framework [46,47]. Key elements of this model include empathic ability, empathic response, and residual compassion stress [46,47]. Nurses’ empathic concern and empathic ability produce an empathic response, which may result in compassion stress and depletion of emotional energy [48]. Compassion stress can cause emotional exhaustion in nursing personnel. Therefore, interventions designed to reduce compassion fatigue among nurses have a critical role to play in preventing professional exhaustion.
We found no association between emotional exhaustion and social support. Previous studies showed that social support could have a buffering effect against emotional exhaustion in nursing personnel [49,50]. Our conflicting results in this regard might reflect the use of different instruments to measure social support. Moreover, a variety of distinctions have been made among various types of social support and the functions they serve [51]. Further research to clarify types of social support in work and non-work relationships is needed.
This study has some limitations. First, there was a lack of information on several occupational covariates that might be associated with burnout, such as additional work performed or workload; we therefore could not include them in the analysis. However, the present study included some variables (e.g., department and occupational status) that may act as proxies for such characteristics. Further studies that include additional explanatory variables related to burnout and larger sample sizes are needed. Second, the scales used were self-report measures. However, these were reliable and validated instruments that have been widely used in other studies. Additionally, the interpretation of our regression analysis was limited in that it included variables that were correlated with one another. The intention was to identify more factors related to emotional exhaustion. To overcome this limitation, further research using a different methodology, such as structural equation modeling, to elucidate the direct/indirect causal relationships between psychological factors and emotional exhaustion is needed. Finally, our results may not be generalizable to populations of other ethnicities. However, our results are generally in line with the limited number of previous studies on nurses, despite differences in instruments, reference standards, definitions of burnout, and ethnicities. This coherence greatly supports the validity of our findings regarding associations between psychological conditions and emotional exhaustion in nursing professionals.
Despite the above limitations, several study findings are important. First, this study covered various nursing settings, including operating rooms, recovery units, intermediate care and outpatient units, and ED/ICU. Additionally, this is one of the first published studies to explore the various sociodemographic and psychological correlates of emotional exhaustion among nursing personnel with the aim of understanding their role in this high-risk profession. Identification of the sociodemographic and psychological factors associated with emotional exhaustion may assist in identifying groups at high risk of exhaustion, as well as potentially modifiable risk factors that contribute to emotional exhaustion, a critical step for developing effective preventative strategies for this vulnerable population. For example, because resilience, perceived stress, and secondary traumatic experiences could predict emotional exhaustion, nurses with less resilience and higher perceived stress could be supported by additional assistants or might receive stress management training to prevent burnout. Third, this study used a large sample size to achieve its goals. Finally, the present study will help to determine where interventions might be effective in preventing emotional exhaustion in nursing personnel. Identifying the target of interventions could help nurses who are at risk of exhaustion to choose proper psychological interventions.
To our knowledge, this is the first study to elucidate the relationships of various psychological factors with emotional exhaustion in a Korean population. Our data showed that psychological characteristics, such as resilience, depression, and secondary traumatic experiences, may play causal roles in emotional exhaustion. Our results offer insight into possible interventions to address these psychological characteristics and thereby prevent emotional exhaustion in nurses.
Acknowledgements
Our study was supported by the grants from the National Center for Mental Health Research & Education, the Seoul National Hospital, Republic of Korea(HM15C1113) and Soonchunhyang University Research Fund.