The Psychometric Properties of the Korean Version of the Verbal Abuse Questionnaire in University Students
Article information
Abstract
Objective
The aim of the present study was to examine the psychometric properties of the Korean Verbal Abuse Questionnaire (K-VAQ) that consists of 15 items related with life-time verbal aggression exposure.
Methods
A total of 5814 university students who agreed to take part in the study completed the K-VAQ, the Korean version of the Life Event CheckList (LEC-K) and Impact of Event Scale-Revised (K-IES-R). Internal consistency was checked by using item-total item correlation and Cronbach's alpha coefficient. Exploratory and confirmatory factor analyses were performed, and convergent and concurrent validity levels were examined. Finally, a cluster analysis was conducted to verify the validity of the cutoff point of the K-VAQ.
Results
The Cronbach's alpha correlation coefficient was 0.9. The K-VAQ showed a single factor structure which explained 55.34% of the total variance. The K-VAQ was significantly associated with the LEC-K (r=0.24) and K-IES-R (r=0.28), indicating good convergent validity and concurrent validity. The cluster analysis provided four clusters of trauma experiences: high, moderate, low, and minimal, with K-VAQ ranges of 43-81, 20-42, 7-19, and 0-6, respectively. In a further investigation, a K-VAQ score of 40 was found to be the appropriate cutoff point to delineate the highly verbally abused group, as used in the previous studies. A sum of 36.5% of the highly verbally abused group reported to show substantial symptoms of PTSD (K-IES-R score >22).
Conclusion
The present findings suggest that the K-VAQ has good psychometric properties for assessing verbal aggression among the Korean population.
INTRODUCTION
Verbal aggression is one of the most common forms of emotional abuse. The fraction of 31.3% of Korean women report to have had parental verbal violence history,1 while 65.3% of Korean children aged between 9 and 12 in protective care report to have experienced emotional abuse.2 In the U.S., the prevalence of emotional abuse during childhood is 14% in men and 10% in women adults.3 However, the effects of exposure to verbal aggression on its victims have been commonly overlooked regardless of their seriousness and harmfulness. Young adults with a history of verbal abuse (VA) are susceptible to display various psychiatric symptoms, including depression, anxiety and dissociation;4,5 VA can also cause children to display negative cognitive styles including self-criticism and hopelessness, which are related to psychopathology.6,7 The effects of VA on mental health are comparable to those of other types of abuse, sexual or physical, which are more commonly considered to be severe,4 and these harmful effects are persistent regardless of whether the abuse was perpetrated by parents or peers.8 Additionally, VA is thought to cause scars on the brain; reduction of fractional anisotropy of white matter tracts in sufferers, including corpus callosum, arcuate fasciculus, cingulum bundle, has been reported.8,9
The harmful effects of VA, compared to physical and sexual abuses, are frequently ignored by those individuals who significantly influence children.10 Also, in middle and high school, many adolescents, nearly two out of three, routinely use profane words without the awareness of their severity.11 To reduce the victims' vulnerability to psychiatric disorders, it is important to develop appropriate measurements and to educate VA's seriousness to the general population, especially children, young adolescents, and even young adults. However, since there is no reliable scale with which to evaluate specific experiences of VA in Korea, developing appropriate measurements of VA experiences can be the first step to recognize the victims.
The verbal abuse questionnaire (VAQ) covers various domains of VA and is a useful tool for detecting a history of VA and measuring the severity of VA experiences. Also, the VAQ is widely applicable regardless of whom the perpetuator is in any specific case. Previous studies have shown that it has adequate internal consistency for both parental VA and peer VA.4,8 Therefore, we considered that this scale can be easily and widely applied to various populations, thus developed a Korean version of the verbal abuse questionnaire (K-VAQ). This study was conducted to verify the psychometric properties of the K-VAQ and to evaluate its utility for application to the Korean population.
METHODS
Participants
The data in this study was obtained from the online annual medical and psychiatric checkups of 5,814 unselected college students, both undergraduates and graduates, of the Korea Advanced Institute of Science and Technology (KAIST). The subjects were assessed between April of 2013 till January of 2014, and all participants voluntarily agreed to complete the questionnaires. The mean age of the subjects was 23.9 [standard deviation (SD)=4.49], and the majority of the sample subjects (77.5%) were male. This study was approved by the Ethics Committee of KAIST.
Assessment
Verbal Abuse Questionnaire
The Verbal Abuse Questionnaire (VAQ) can evaluate 15 types of verbal abuse, including scolding, yelling, swearing, blaming, threatening, demeaning, ridiculing, insulting, criticizing, screaming, belittling, and devaluating, among other types. This questionnaire uses a nine-point scale to measure the frequency of each item (0=not at all to 8=everyday) during life-time, and the total score is the sum of the 15 items (range, 0-120). The VAQ can also be applied to various types of VA. The VAQ shows adequate internal consistency for both parental VA (Cronbach's alpha=0.98 for maternal and Cronbach's alpha=0.94 for paternal) and peer VA (Cronbach's alpha=0.95 in females and Cronbach's alpha=0.96 in males).4,8 In our study, the severity of parental VA was measured to standardize the VAQ scale.
Life Events Checklist
The Life Events Checklist (LEC) is the most widely used scale to evaluate general traumatic events with adequate levels of reliability and validity.12,13 It is a 17-item self-report questionnaire with items ranging from natural disasters to stressful events. It is rated using five nominal responses: 'happened to me', 'witnessed it', 'learned about it', 'not sure', and 'does not apply'. Recently, the reliability of the Korean version of the LEC (LEC-K) was verified (Cronbach's alpha=0.67).14
Impact of the Event Scale-Revised
Horowitz et al.15 developed the Impact of the Event Scale (IES) in 1979, which consists of 15 items that reflect two main symptom clusters of PTSD (intrusion and avoidance). However, another main symptom cluster of PTSD, hyperarousal, could not be evaluated using the original IES. A revised version of the IES (IES-R), which contains five items related to hyperarousal, was newly developed in 2007.16 In the IES-R, the items evaluate the severity of PTSD symptoms experienced during the previous week by using a five-point scale (0 to 4). The Korean version of the IES-R has shown a good reliability in the previous research (Cronbach's alpha=0.93, test-retest reliability coefficient r=0.91), and with a cutoff point of 22, also showed good sensitivity (0.95) and specificity (0.80) to predict PTSD diagnosis.17
Procedures
After obtaining the permission from the original author of the VAQ scale, a forward-backward translation process was conducted. First, one psychiatrist and one bilingual student fluent both in Korean and English jointly translated the original VAQ into Korean. Secondly, a clinical psychologist, who had completed a doctoral degree in England and another psychiatrist who was fluent in English translated the Korean version back to English. Finally, a committee consisting of three psychiatrists, one psychologist, one neurologist, and one bilingual student reviewed and adjusted the K-VAQ to make it more apprehensible and adaptable to the Korean culture.
Statistical analysis
Participants' demographic characteristics were assessed using descriptive statistics. For internal consistency including item-total item correlation, the Cronbach's alpha coefficient was calculated. Exploratory factor analysis was performed using principle axis factoring (PAF) extraction methods with varimax rotation. Convergent and concurrent validity were assessed using Pearson's correlation coefficient. The aforementioned analyses were conducted using SAS software (version 9.3; SAS Institute, Cary, NC, USA). Confirmatory factor analyses were performed using the Mplus 7.1 software package. Five model-fit indices were chosen to determine the goodness-of-fit of the model: 1) the chi-squared statistic, 2) the non-normed fit index (NNFI, 0.95 or greater), 3) the root mean-square error of approximation (RMSEA, 0.06 or less); 4) the standardized root mean residual (SRMR, 0.08 or less), and 5) the comparative fit index (CFI, 0.95 or greater).18,19
Additionally, a cluster analysis was conducted to verify the validity of the cutoff point of 40 of the VAQ; this value was also used in previous studies.4,8,9 Both the K-VAQ and the LEC-K, which represent previous traumatic experiences, were used in the cluster analysis to divide the subjects according to their trauma intensity. To select a suitable number of clusters in the k-means clustering analysis, the bend point in a sum-of-squared error (SSE) plot was investigated using the R package.20 Also, group differences in the PTSD symptoms as measured by the K-IES-R were evaluated by means of a one-way analysis of variance (ANOVA).
RESULTS
Internal consistency
The Cronbach's alpha correlation coefficient for the K-VAQ was 0.93. The corrected item-total correlation coefficients ranged from 0.49 to 0.78, indicating an acceptable range.21
Exploratory Factor Analysis
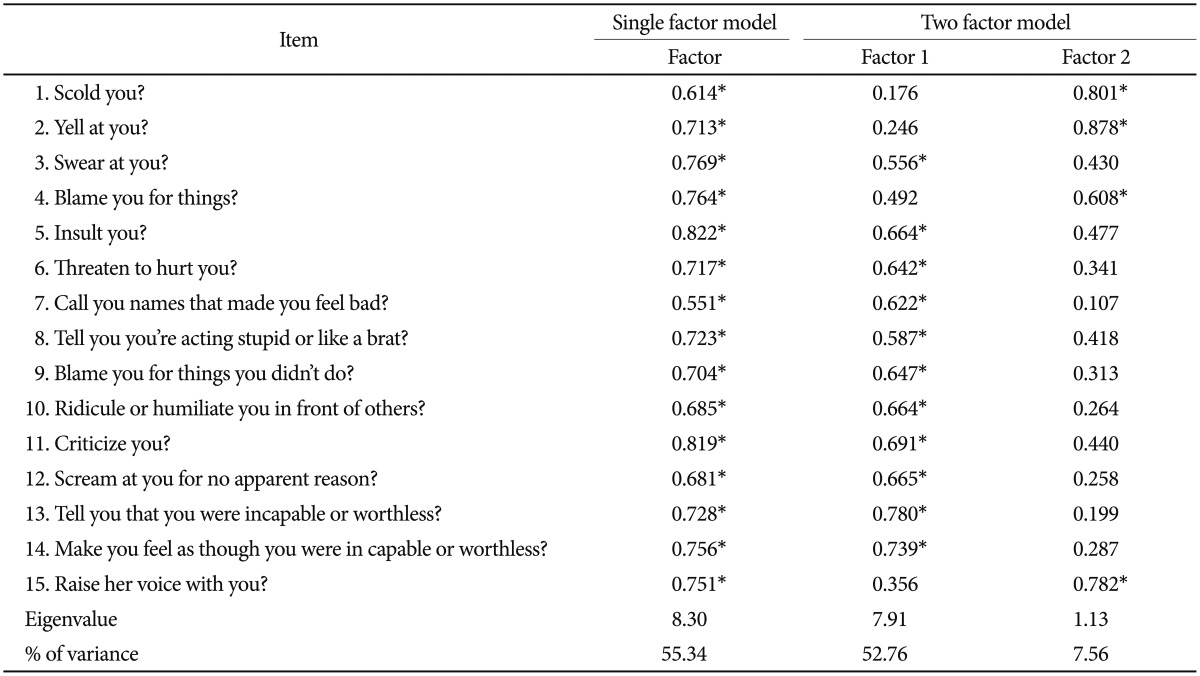
The Kaiser-Meyer-Olkin Measure (KMO) value for sampling adequacy was 0.952, and the chi-value of Bartlett's test of sphericity was 59551.220 (p<0.001), which indicates that the data in the present study is satisfactory for use in a further exploratory factor analysis. The eigenvalue (>1) and a scree plot showed that two factors explained 60.32% of the total variance; Factors 1 and 2 accounted for 55.34% (eigenvalue: 8.30) and 9.80% (eigenvalue: 1.47), respectively. Factor 1 included eleven items reflecting swearing, insults, humiliation, threats, screaming and blaming. Factor 2 consisted of the four items of raising ones' voice, yelling, scolding, and blaming. All rotated factor loadings exceeded 0.50. However, we noted that, while items 1, 3 and 15 generally reflected the contents of raising voices, item 12 ("scream at you for no apparent reason") of Factor 1 also implies a raised voice. The contents of item 4 classified in Factor 2 ("blame you for things") also overlap those of item 9 ("blame you for things you didn't do") of Factor 1. Furthermore, the variance of Factor 2 appeared to be small compared to that of Factor 1. In light of these findings, alternatively, we performed the same analysis using a fixed number of factors as a single factor. As a result, a single factor accounted for 55.34% (eigenvalue: 8.30) of the total variance. All factor loadings were over 0.50, confirming that all items could be classified as a single factor. Table 1 presents the single factor and two factors, each with factor loading values, eigenvalues, and the percentage of variance explained in each case.
Exploratory Factor Analysis of Korean version of the verbal abuse questionnaire (N=5814)
Confirmatory Factor Analysis
Exploratory factor analyses were conducted for single-factor and two-factor models. The single-factor model showed a very good fit for the data, [χ2(43)=809.897, p=0.000, NNFI= 0.987, CFI=0.969, RMSEA=0.055, and SRMR=0.02]. The two-factor model showed a poor fit for the data, [χ2(87)= 3987.609, p=0.000, NNFI=0.934, CFI=0.921, RMSEA=0.088, and SRMR=0.49] (Table 2). In addition, the difference between two models was significant [Δχ2=3177.712 > χ2.05 (40)= 55.76 ~ χ2.05 (50)=67.50. Δd.f=44]. These results confirmed that the single-factor model is more suitable for verbal aggression compared to the two-factor model.

The fit of confirmatory factory analyses of the single factor and two factor models (N=5814)
Convergent and concurrent validity
The Pearson correlations were calculated in order to determine convergent and concurrent validity between the K-VAQ, the LEC-K and the K-IES-R. These results are shown in Table 3. The total scores of the K-VAQ were significantly associated with the total scores of the LEC-K, indicating good convergent validity. The total scores of the K-VAQ showed highly significant association with the K-IES-R, confirming good concurrent validity. Table 3 shows the correlations between the K-VAQ and the related assessments.
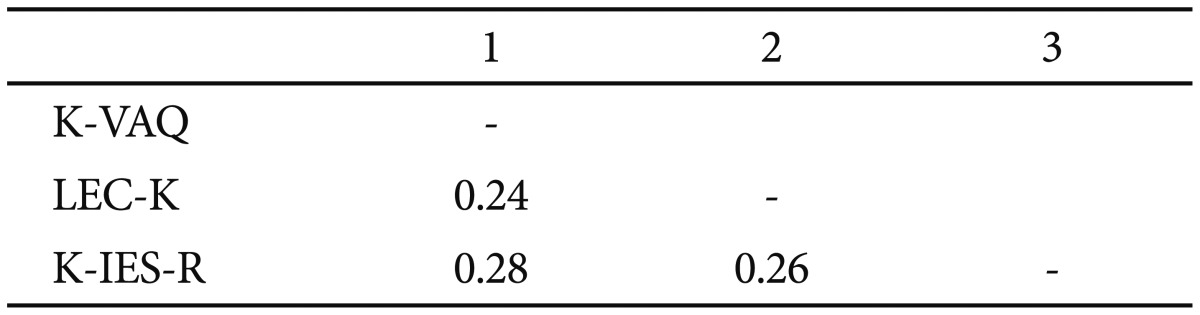
Pearson Correlations of the measures variables (N=5814)
Cluster analysis
The subjects were divided into four groups according to the bend point in the SSE plot with an appropriate number of subjects in each group (Figure 1). We excluded four outliers who showed extremely high K-VAQ scores (90, 91 and two at 105) and arranged the subjects according to the severity of their trauma experiences. Finally, we categorized the subjects into four groups: high, moderate, low and minimal trauma experienced groups. Each group can be distinguished from one another by its range of the K-VAQ scores (high=43-81, moderate=20-42, low=7-19, and minimal=0-6) (Figure 1). Based on the results of the cluster analysis, we divided the subjects into four groups according to their K-VAQ scores, applying the previous cutoff score of 404,8,9 (highly=40 or above, moderately=20-39, low=7-19, minimally verbally abused=0-6). The trauma-related symptoms measured by the K-IES-R showed significant differences among the four different verbal-abuse groups [F(3, 5806)=123.03, p<0.001] (Figure 2). A large proportion (36.5%) of the highly verbally abused group reported K-IES-R scores that exceeded the cut-off point (K-IES-R score >22),17 while the moderately, low and minimally verbally abused groups showed a small number of the subjects with K-IES-R scores above the cut-off point (17.6%, 7.6% and 4.4%, respectively). These differences in the frequency were statistically significant in a chi-square test [χ2(3)=212.42, p<0.001]. Also, in a post-hoc analysis, the highly verbally abused group showed a higher PTSD symptoms than the moderately verbally abused group [χ2(1)= 12.16, p<0.001].

Sum-of-squares plot (A) and Korean version of the Verbal Abuse Questionnaire (K-VAQ) scores according to groups (B). All subjects were divided into four groups according to the bend point in the sum-of-squared error (SSE) plot (A). Every group has an adequate number of subjects and specific ranges of the K-VAQ score (B).
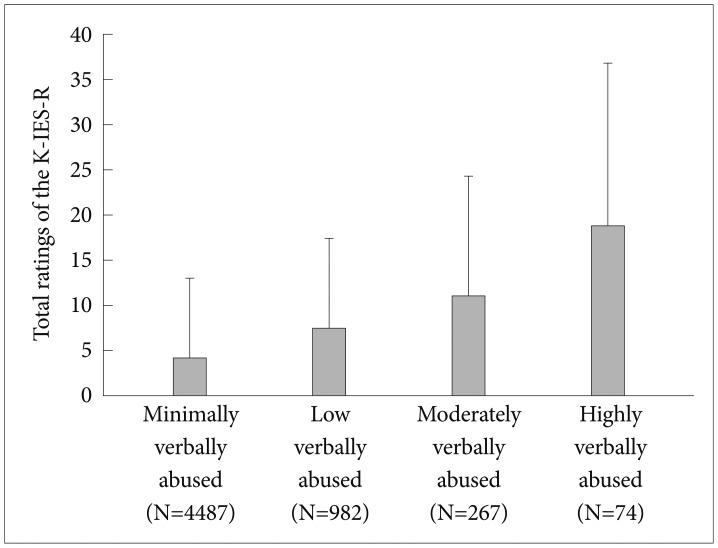
The ratings of the Korean version of the Impact of the Event Scale-Revised (K-IES-R) among the four groups. The K-IES-R scores showed significant differences among the four groups [F(3, 5806)=123.03, p<0.001]. In a post-hoc analysis, the mean (SD) of the K-IES-R scores in highly verbally abused group [18.89 (17.92)] was significantly greater than those of other groups [moderately: 11.17 (13.22), low: 7.55 (9.97) and minimally verbally abused groups: 4.34 (8.65)]. All other group differences were also statistically significant (Bonferroni corrected p<0.001).
DISCUSSION
In our study, the K-VAQ showed adequate psychometric properties when used to measure the participants' parental VA experiences. The internal consistency of the K-VAQ (Cronbach's alpha=0.93) showed an acceptable value, similar to previous studies using the original version of the VAQ (Cronbach's alpha=0.98 for maternal and Cronbach's alpha=0.94 for paternal). Also, the item-total item correlation coefficients were within the optimal range (r>0.3).22
In the exploratory factor analysis, two factors were originally extracted, accounting for 55.34% (eigenvalue: 8.30) and 9.80% (eigenvalue: 1.47) of the total variance, respectively. These results are consistent with the study conducted by Teicher et al.4,23 However, unlike the results of the original study,4,23 item 4 was additionally identified as one of the factors in the factor 2 category, along with items 1, 2, and 15. These four items in the factor 2 category consisted of 'raised voices' (items 1, 2, and 15) and 'blame' (item 4). However, we found that some items in factor 1 also included a similar content. For example, item 12 in the factor 1 category implies 'a raised voice' ('scream at you for no apparent reason'). The content of item 9 ('blame you for things you didn't do') was similar to that of item 4 ('blame you for things'). This suggests that the K-VAQ is not clearly classified into two factors. Alternatively, we found a single factor that accounted for 55.34% of the total variance. All factor loadings for each item exceeded 0.05, indicating that all items of the K-VAQ can be classified as a single factor.
To determine the dimensions of the K-VAQ scale, both one-factor and two-factor models were verified using structural equation modelling (SEM). This concluded that the single-factor model is more suitable than the two-factor model. The original version of the VAQ also used the total score of all questions to screen for the presence of a history of VA. This also did not categorize into two subscales. Therefore, our analysis support that the single-factor model can be useful to evaluate VA.
The convergent validity of the K-VAQ was confirmed with significant results from the correlation analysis between the K-VAQ and the LEC-K, a general scale used to evaluate traumatic life events.14 Although the LEC-K did not contain those items that were directly associated with verbal abuse, our results imply the existence of common characteristics in both measures. To substantiate, existing evidences show that verbal abuse leads to elevated psychiatric symptoms, similar to those from physical abuse or catastrophic natural disasters (e.g., earthquake, war).8 In this sense, our result shows a possibility that verbal abuse could be a form of psychological trauma that has detrimental impacts on one's mental health. Likewise, concurrent validity was proven by the significant correlations between the K-VAQ and the K-IES-R. Recent studies noted that there were significant relationships between emotional abuse and symptoms of PTSD. Emotionally abusive experiences can significantly predict PTSD symptoms in adolescents of child protective services24 and in general adults.25 Nurses of the psychiatric department who were verbal abused by patients also reported elevated PTSD symptoms as measured by the IES-R.26 Our results are in line with such previous studies by demonstrating that verbally abusive experiences in university students are significantly associated with PTSD symptoms as measured by the K-IES-R.
Moreover, we evaluated the validity of original VAQ's cut-off score. To measure the appropriate cutoff score of the K-VAQ, we conducted a cluster analysis. In the previous research, a cutoff point of 40 was utilized, representing the top 10% of scores in randomly selected participants. This cutoff point showed face validity.4 The upper 10% criterion was not applied to our study because our data was acquired from a yearly health examination conducted by a university. A large number of students marked zero on the K-VAQ measure (n=2194), and 77% of our subjects (n=4487) were classified into the minimal trauma experience group. Therefore, a cluster analysis was appropriate to confirm the cutoff point in our data. Within our subjects, there were eight who had K-VAQ scores between 40 and 42; they reported similar ratings on the K-IES-R [mean (SD)=18.13 (20)] and similar frequency of K-IES-R scores that exceeded the cut-off point (38%) to those of the group which reported K-VAQ scores of 43 or above [the K-IES-R mean (SD) score=18.99 (17.82), frequency of K-IES-R scores above the cut-off score=36.4%]. Hence, including these eight subjects in the highly verbally abused group did not disrupt the characteristics of the group; the highly verbally abused group showed significant differences in PTSD symptoms compared to moderately verbally abused group. In sum, previous criteria using VAQ scores of 40 or above8,9 can be acceptable to find those who had strong verbal abuse experiences that threaten their mental health. Further studies may maintain a connection to the previous studies using this cutoff score. Another potential area for research is of determining whether there are potential mental health problems in subjects who have K-VAQ scores of 20 or above.
There are several limitations to this study. First, the study was performed with university students from a top-ranked university in Korea. Most of the participants were young, male and highly educated. Our subjects might have been raised in a good environment, including high level of social and economic status (SES). Given that childhood maltreatment are influenced by low SES,27 future studies are warranted to include participants with various SES. Among the participants, 37.7% (2194/5814) reported no verbal abuse experience in their lifetime. We are interested in investigating whether this statistics would reflect the representativeness of the general population in a future study. Second, our anonymized data were extracted from a yearly health examination; the degree of test-retest reliability was not evaluated here. Further study is needed to measure the longitudinal stability of the K-VAQ scale and to generalize this scale to various age ranges.
Despite these limitations, this study suggests that the K-VAQ has good psychometric properties. As our sample size was quite large and young adults were suitable subjects, given that VA from parents or peers mainly occurred during their childhoods, our results are likely to be reliable. The K-VAQ can be widely administered to measure the severity of various types of VA and can be used as a screening tool for the presence of VA. This scale can be useful for teachers, clinicians, health care workers, psychologists, or anyone in close contact with young students.
Acknowledgments
Thanks to H.C. Park's help to translate the English version of the VAQ to Korean one.
This work was supported by grants NRF-2012R1A1A2001 and NRF-2006-2005372 (to B. Jeong) from National Research Foundation, and in part by grant for KAIST Future Systems Healthcare Project from the Ministry of Education, Science and Technology (N01130009, N01130010, G04110085 to B. Jeong).