INTRODUCTION
The Yale-Brown Obsessive-Compulsive Scale (Y-BOCS)1,2 has been used widely and is accepted as the gold standard for measuring obsessive-compulsive disorder (OCD) symptom severity and treatment outcome.3 Unlike other OCD measures that aggregate various symptom frequencies or intensities to create on overall severity score, the Y-BOCS has an advantage in that it is not influenced by the type or number of obsessions or compulsions and is sensitive to symptom change as items intended to measure putative state variables.1,4 Several psychometric studies of the Y-BOCS have yielded generally positive results that showed that the Y-BOCS has high internal consistency and adequate content, construct, and criterion-related validty.4-7
The Y-BOCS consists of two parts: the Symptom Checklist for evaluating the presence of current and past symptoms, and the ten-item Severity Scale (rated 0-4 per item) that assess obsessions and compulsions separately in five dimensions (time spent, interference, distress, resistance, and control). Separate Obsession (items 1 to 5) and Compulsion (items 6 to 10) subscale scores (range 0-20) are summed to yield a total Y-BOCS score (range 0-40).
Although Goodman et al.1,2 developed the Y-BOCS as a clinician-administered measure with the purpose of making a more objective evaluation during the acute stages of illness, several self-report versions of the Y-BOCS were subsequently developed, including computer-administered and paper-and-pencil forms.8-11 The self-report Y-BOCS is a time-saving, less costly substitute for the interview format for assessing OCD symptoms.10 For example, the clinician-administered version typically takes 30 min to complete and requires that raters be trained both to administer the scale and in OCD symptomatology, while the self-report version requires approximately 10 min to complete without help from others.8,10,11 The self-report Y-BOCS has good internal consistency and test-retest correlations compared with the interview version.10 Convergent validity between the interviewer-rated and self-report versions is moderate to high with correlations ranging from 0.45-0.6511 to 0.73-0.88.8,10
Despite the growing use of the self-report Y-BOCS, especially in computerized cognitive-behavior therapy such as OCFighter,12 there are still significant gaps in the psychometric literature regarding the validity of this measure. In particular, it is important to examine the factor structures of the Y-BOCS to make inferences about the nature of OCD symptom severity and to establish a valid measure for that construct. For example, it is necessary to examine whether OCD symptom severity is best conceptualized according to the Obsession and Compulsion subscale composition originally proposed by Goodman et al.1
Although many studies have examined the factor structure of the clinician-administered Y-BOCS, the results have been inconsistent, including one-, two-, or three-factor models. Some confirmatory factor analysis studies confirmed the original two-factor model,13-15 whereas other investigators identified different two-factor solutions using Disturbance and Symptom Severity factors16 or Severity and Resistance/Control factors,5 in that the common features of the Obsession and Compulsion subscales load together on the same factor. In addition, there is a single-factor structure called Global Impairment17 and a three-factor model comprising Severity of Obsession, Severity of Compulsion, and Resistance to Symptoms factors.18,19
To our knowledge, only one study20 has examined the factor structure of the self-report Y-BOCS, supporting the original two-factor (Obsessions and Compulsions) model. However, that study did not include a clinical OCD sample. In addition, two previous studies10,11 using the self-report Y-BOCS focused mainly on the level of agreement between the clinician-administered and self-report versions, and did not use other measures of OCD or other symptom measures.
Therefore, we developed Korean self-report version of the Y-BOCS and examined its psychometric properties including factor structure, distinguishing between non-clinical and clinical samples. A non-clinical sample was included because obsessive compulsive phenomena are also common in non-clinical populations and the study of normal individuals might provide valuable information about the nature of OCD.7,21,22 Most studies of people with subclinical OCD have relied on self-report measures, such as the Maudsley Obsessional-Compulsive Inventory (MOCI)23 and Padua Inventory (PI).24 However, the self-report Y-BOCS can provide additional information about the severity and diagnosis of OCD in non-clinical samples.7
In addition, it can suggest meaningful data with discriminant validity to compare normal subjects and clinical OCD patients in terms of the total score of the Korean self-report version. Although the Y-BOCS was originally not intended as a diagnostic instrument,2 a cutoff score of 16 has been used as the threshold of clinical symptom severity.25 We examined whether the cutoff score of the self-report version was identical to that of the interviewer-rated version.
In summary, in this study we evaluated the 1) factor structure of the Korean self-report version, 2) internal consistency of the Korean self-report version items, 3) convergent and discriminant validity of the Korean self-report version, and 4) categorical classification between non-clinical and clinical samples with the total score of the Korean self-report version.
METHODS
Participants and procedures
Psychometric studies of Korean self-report version of the Y-BOCS were conducted on two independent samples: a non-clinical student population and clinical OCD patients. The data collection and procedures used in this study were all approved by the institutional review board of Seoul National University College of Medicine (C-1206-101-415).
The non-clinical sample included 208 undergraduates from a single university who were solicited in an introductory psychology course. All participants provided written informed consent and a small gift (e.g., a lollipop) was offered for participating in this study. They completed a questionnaire booklet anonymously in about 20 min. This consisted of Korean self-report version of the Y-BOCS, MOCI, and PI to measure OCD symptoms, and the Beck Depression Inventory (BDI)26 and Beck Anxiety Inventory (BAI).27 Two participants who were taking medication for depression or anxiety were not included, since this was intended to represent a non-clinical sample. Consequently, data for 206 participants were analyzed. Among the non-clinical sample, 65.0% were males and 35.0% were females who were all Asian, with a mean age of 21.41 years (SD=2.76).
Data for the clinical sample were collected from the medical records of 204 patients who attended an outpatient clinic for pharmacological management or cognitive-behavioral therapy for OCD in a university hospital. All participants had a principal diagnosis of OCD according to the criteria defined in the Diagnostic and Statistical Manual of Mental Disorders, 4th ed.28 The diagnoses were ultimately determined by psychiatrists experienced in OCD based on a psychological evaluation and several clinical interviews during treatment. Finally, data for 199 patients were analyzed because patients were excluded who had the following diagnoses: current or past psychosis (n=2), current alcohol or substance dependence (n=1), or neurological disorders (n=2). Although the OCD patients completed the same questionnaire booklet, except for the PI before and after treatment, the pre-therapy data were analyzed here. The participants were all Asian and 119 (59.8%) were male. Their age ranged from 16 to 54, with a mean 28.41 years and their educational attainments equaled to and higher than those of high school graduates (years of education: mean=14.29, SD=2.08).
Measures
Korean self-report version of the Y-BOCS used here is based on the paper-and-pencil version of the Y-BOCS developed by Baer,9 which consisted of a 58-item Symptom Checklist eliminating open-ended 'other' items and a 10-item Severity Scale rated over the last week on a five-point Likert scale. While Baer modified the wording of questions 4 and 5 to clarify their meaning and to emphasize the goal of successful behavior therapy treatment for OCD,9 our self-report version is faithful to the original clinician-administered Y-BOCS proposed by Goodman et al.1,2 and somewhat different from Baer's version in items 4 and 5. We used the self-report version with Baer's permission and had it translated into Korean independently by two clinical psychologists and back-translated by a third bilingual psychologist.
To assess convergent validity, the Korean self-report version ratings were correlated with the following commonly used measures of OCD: the MOCI23 and PI.24 The MOCI consists of a 30-item true/false questionnaire to identify the presence or absence of specific OCD symptoms; it is internally consistent and has satisfactory test-retest reliability.29 The alpha coefficients for the MOCI were 0.78 for the non-clinical sample and 0.80 for the clinical sample in our study. The PI is a 60-item self-report questionnaire, developed to assess the most important OCD symptoms, including intrusive thoughts and ruminations.24 All items are rated on a 5-point scale from 0 (not at all) to 4 (very much), for a total possible score of 240. The internal consistency for PI was high as 0.95 for the non-clinical sample in our study.
To examine discriminant validity, the Korean self-report version ratings were correlated with measures of depression (the BDI)26 and anxiety (the BAI).27 The BDI is a 21-item self-report scale that assesses the severity of affective, cognitive, motivational, vegetative, and psychomotor components of depression. The total score ranges from 0 to 63 and scores ≥20 suggest the presence of clinical depression. The BDI has excellent reliability and validity and is widely used in clinical research.30 The BAI contains 21 items that assess anxiety symptoms and all items are rated on a 5-point Likert scale.27 The scale has adequate internal consistency and test-retest reliability.27
Analysis
All analyses were conducted using SPSS (ver. 20.0) and AMOS (ver. 20.0), separately for the non-clinical and clinical samples.
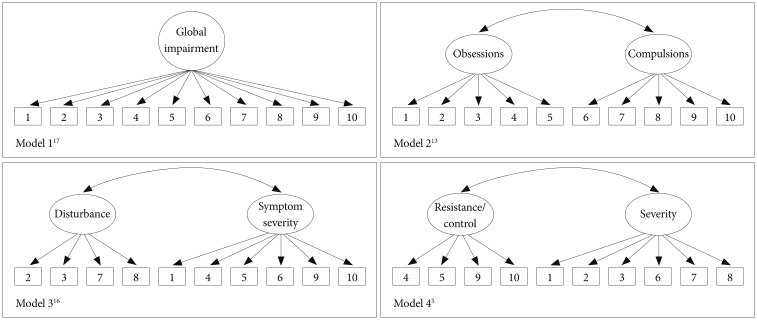
To determine the factor structure of the Korean self-report version, confirmatory factor analysis (CFA) was undertaken. Four models were specified: 1) a single-factor model;17 2) a two-factor model representing Obsessions vs. Compulsions;13-15 3) a two-factor model representing Disturbance vs. Symptom Severity;16 and 4) a two-factor model representing Severity vs. Resistance/Control.5 A three-factor model18,19 representing Obsessions (items 1-3 and 5), Compulsions (items 6-8 and 10) and Resistance to Symptoms (items 4 and 9) were not included in the CFA models, because AMOS cannot identify a factor determined using less than three items. Although a single-factor model17 was originally constructed using a 16-item version of the Y-BOCS in an exploratory factor analysis, this study examined the fit of the CFA model with the ten core items. All CFA analyses were conducted using maximum-likelihood estimation and the error terms for frequency, interference, distress, resistance, and control of obsessions were correlated with the respective items referring to compulsion, following the suggestions of previous studies.5,13,15,19
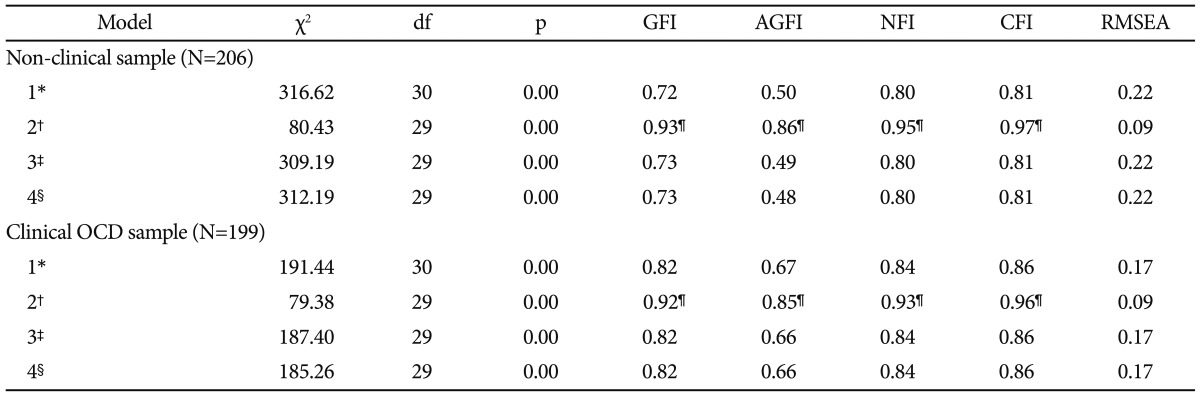
The model fit for the CFA was evaluated using multiple fit indices, including the chi-square, goodness-of-fit index (GFI), adjusted goodness of fit index (AGFI), normed fit index (NFI), comparative fit index (CFI), and root mean square error of approximation (RMSEA).31 GFI, CFI, and NFI values >0.9 were considered to represent an optimal adequate model fit.31 The AGFI values were considerably greater than the cutoff of 0.80 recommended by Cole.32 Recommendations for the RMSEA suggest that values close to 0.06 represent a good fit,33 values less than 0.08 indicate an acceptable fit, and values between 0.08 and 0.10 represent a poor model fit.34
The internal consistency of the Korean self-report version was assessed using Cronbach's alpha. For all 10 severity items, corrected item-total correlations were calculated with 1) the corresponding factor score confirmed as the best-fitting model from the CFA and 2) Y-BOCS total score. Pearson product-moment correlations were computed to examine the associations among the Korean self-report version, MOCI, PI, BDI, and BAI. Following a previous study, an alpha level of p<0.01 was chosen as the criterion for significance to reduce type I error.7
Finally, we compared the Korean self-report version scores of the OCD patients with the scores of the non-clinical students. Discriminant analysis was performed to examine whether Korean self-report version of the Y-BOCS could differentiate the clinical OCD sample from the non-clinical sample.
RESULTS
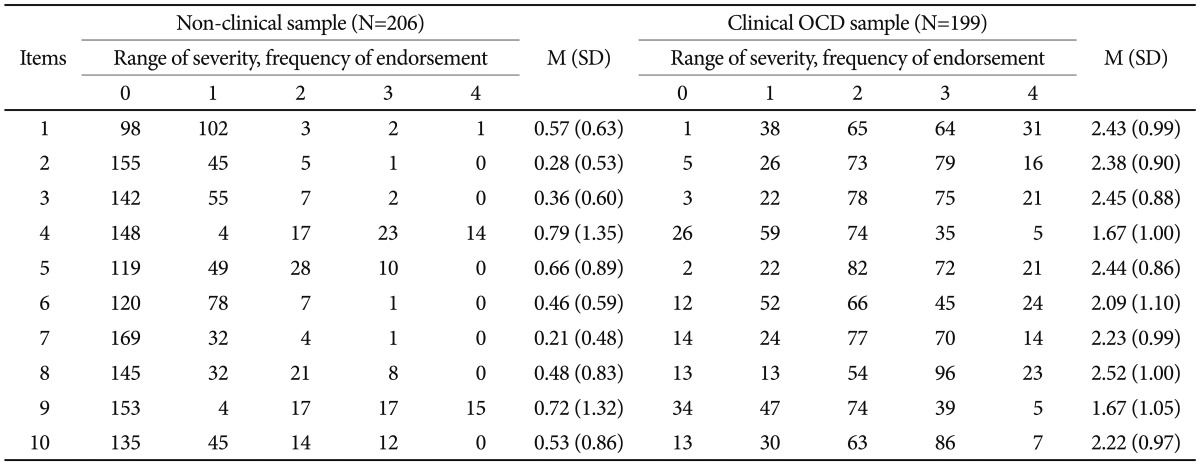
The individual item scores and endorsement frequencies are shown in Table 1. Most of the non-clinical samples scored of 0 or 1 on all items, whereas the clinical OCD sample scored across the range of severity. However, the distributions of the scores for items 4 (resistance to obsession) and 9 (resistance to compulsion) were considerably different from all of the other items in the clinical sample, and these were scored 0 (symptom not present) in 13.1% and 19.1% of the cases rated, respectively.
Confirmatory factor analysis
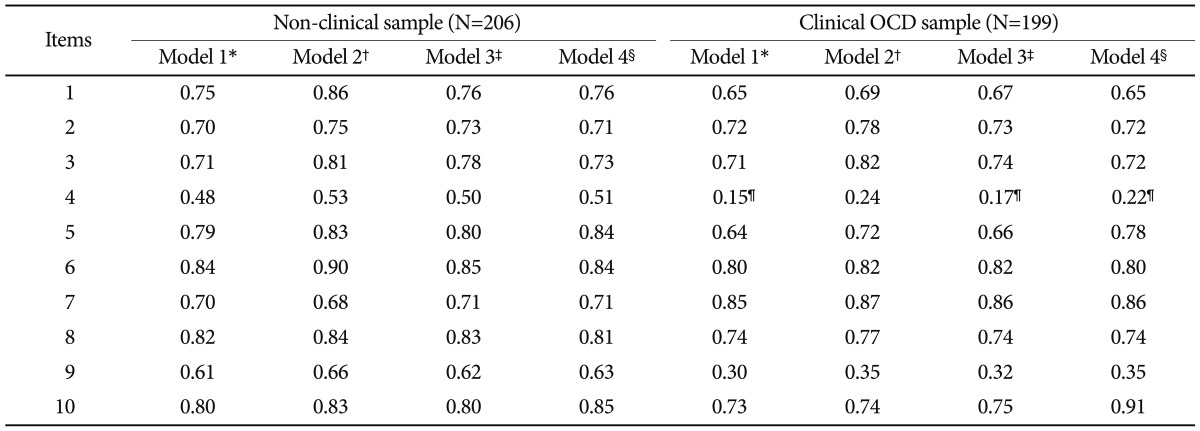
One single-factor model and three two-factor models were fit. These models are represented pictorially in Figure 1, with the relative fit indices in Table 2. The best-fitting model was clearly that of McKay et al.13 with nearly all fit indices falling in an acceptable range in both the non-clinical and clinical samples. The Obsessions and Compulsions factors in model 2 were very strongly correlated in the two samples, with r=0.75 and r=0.79, respectively. The factor loadings for item 4 did not reach significance in any CFA model, except model 2 in the clinical OCD sample (Table 3).
Internal consistency
The internal consistencies for the Total, Obsession subscale, and Compulsion subscale scores were adequate in two samples: for the non-clinical sample, α=0.89, 0.79 and 0.84, respectively; for the clinical OCD sample, α=0.87, 0.77 and 0.83, respectively. The corrected item-total correlations are shown in Table 4. All were significant at p<0.01. However, items 4 and 9 showed relatively weak correlations, while the other items showed moderate-to-strong correlations in the clinical OCD sample.
Convergent and discriminant validity
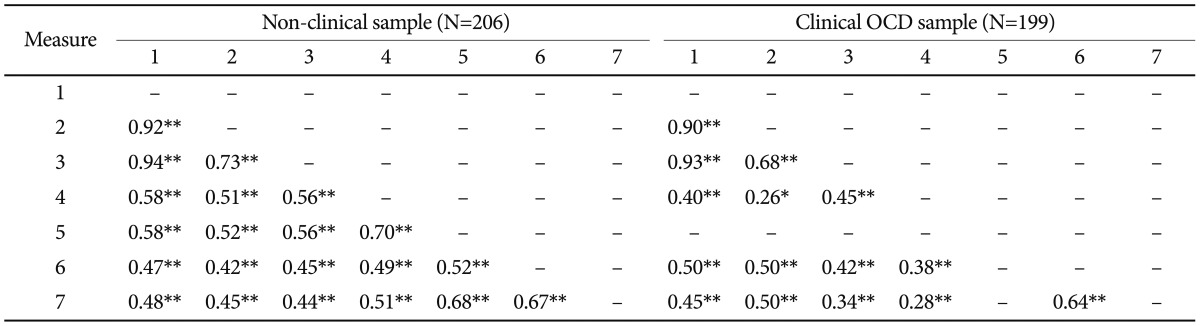
The correlations between study measures were all significant at p<0.01 (Table 5). For the non-clinical sample, the total score and two subscale scores of the Korean self-report version showed moderate correlations with two other measures of OCD. These significant correlations could be due to a small number of individuals who have true OCD, but are not yet diagnosed. To determine whether this could have happened, we recalculated the correlations with subjects scoring ≥16 on the Y-BOCS total score dropped from the analysis (14 subjects); however, all remained significant with the MOCI, r=0.45, p<0.01 or with the PI, r=0.44, p<0.01. Significant correlations between the Korean self-report version and MOCI were identified in the clinical sample; however, the correlation with regard to the Obsession subscale was relatively weak.
To examine the discriminant validity of the Korean self-report version, Pearson correlations were calculated for the total and two subscale scores in relation to the BDI and BAI. The Korean self-report version was as strongly related to the BDI and BAI as to other measures of OCD symptoms in both the non-clinical and clinical samples. In particular, the Obsession subscale scores had noticeably lower correlation with the MOCI than with the BDI and BAI in the clinical sample.
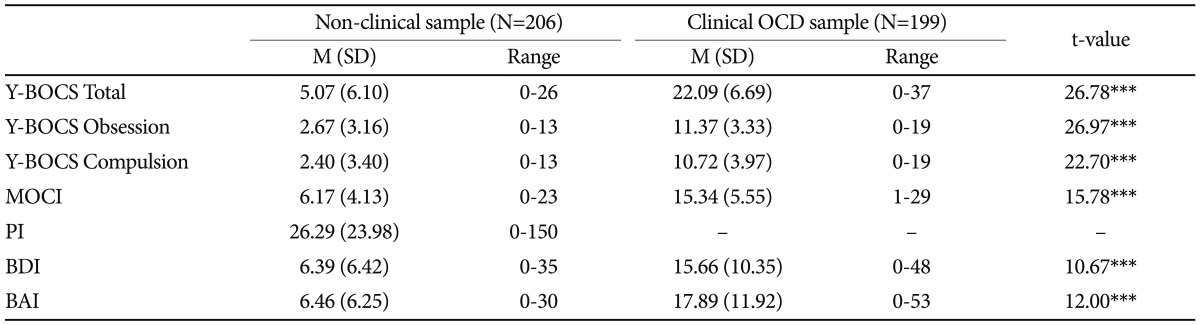
The results of study measures in the non-clinical and clinical samples are presented in Table 6. As expected, the clinical sample had significantly higher scores for all measures than did the non-clinical sample. The discriminant function using the Korean self-report version was highly reliable, χ2 (10)=522.28, p<0.001, and was able to correctly classify 93.3% of the OCD patients and 95.6% of the normal students in the original model. When we examined the number of subjects in each group who fell above or below the commonly used cutoff score of 16 for the original Y-BOCS, 31 (84.4%) of 199 OCD patients fell below the cutoff and 14 (93.2%) of 206 non-clinical students scored above the cutoff, showing very good specificity, but relatively low sensitivity.
DISCUSSION
Despite the growing use of the self-report Y-BOCS, psychometric studies of this scale remain limited. This study developed Korean self-report version of the Y-BOCS and examined its construct validity in two samples: 206 normal students and 199 outpatients diagnosed with OCD. First, we conducted confirmatory factor analyses to determine the underlying factor structure of the Korean self-report version. Then, we investigated the reliability and validity of the corresponding Y-BOCS factors by examining correlations with other measures of OCD and related clinical symptoms. Finally, we examined whether the standard cutoff score of 16 is useful for categorical classification in the Korean self-report version.
The factor structure found in this study is consistent with the original two-factor model proposed by Goodman et al.1,2 and empirically supported by McKay et al.13,14 Although Garnatt and Norton20 suggested the same two-factor model for the self-report Y-BOCS, their study was limited in that no outpatient sample with a diagnosis of OCD was included. Our study is meaningful in that it is the first to report that the self-report Y-BOCS has Obsessions and Compulsions factors not only in non-clinical students, but also in a clinical OCD sample. Using the self-report version, the OCD symptom severity needs to be assessed based on Obsession and Compulsion subscale scores separately, as well as the total score. These findings should be replicated in other large samples, considering the inconsistent results regarding the factor structures of the original Y-BOCS in previous studies.13-20
The two subscale scores and total score of the Korean self-report version showed good to excellent internal consistency. The alphas for the Korean self-report version in both the non-clinical and clinical samples were equivalent to or slightly better than the alphas for the clinician-administered Y-BOCS, which ranged from 0.696 to 0.91.1 Regarding validity, the Korean self-report version showed results comparable to the interviewer-rated version, indicating good convergence, but relatively poor divergent validity.2,6,7
The correlation of the interviewer-rated Y-BOCS with the MOCI was 0.58 in a non-clinical sample7 and ranged from 0.436 to 0.531 in a clinical sample, similar to our results for the Korean self-report version. However, a low correlation of the MOCI with the Obsession subscale score was observed in the clinical sample only, which differed from the findings of the previous study. Since the MOCI focuses to evaluate observable obsessive-compulsive rituals such as checking, cleaning, slowness, and doubting,23 it might be insensitive to the severity of the obsessions. It is also possible that the moderate correlation of the MOCI with the Obsession subscale became weak due to low convergence for the Obsession subscale between the self-report and interview versions.11 Obsessions may be more difficult to assess than compulsion in the self-report version, perhaps because the respondents might more easily confuse them with other phenomena, such as worries.35
The original Y-BOCS was equally or more highly correlated with depression or anxiety (e.g., BDI, BAI, and Hamilton Depression and Anxiety Scale) than with measures of OCD (e.g., MOCI, PI-Revised, and Obsessive-Compulsive Inventory-Revised).2,4-7 Some investigators have suggested that the incomplete convergence between the clinician-administered Y-BOCS and the other self-report measures of OCD might be related simply to differences in the methods of administration.2,4 However, the relationship between measures of OCD symptoms, anxiety, and depression most likely reflects the distress and debilitation associated with severe OCD,6 in that similar results were obtained for the Korean self-report version in our study. Consequently, neither the self-report version nor the interviewer-rated version appear useful for discrimination of the severity of OCD from the severity of depression or anxiety in patients with OCD with marked secondary depression.2
Consistent with previous studies,5,6,19,20 item 4 (resistance to obsessions) was problematic in this regard, as it had the lowest item-total correlation and a non-significant factor loading in various CFA models, especially in the clinical sample. A contemporary cognitive-behavioral model of OCD36 suggested that individuals with greater insight into the senselessness of their symptoms are less likely to attempt to resist or control them. Item 4 showed relatively good internal consistency and validity in the non-clinical sample that has little reason to resist obsessions or compulsions. Recently, the 'resistance to obsessions' item was eliminated from the Y-BOCS-second edition,4 because it was not a manifestation of psychological health, as was its original intention.1
Finally, we identified relatively low sensitivity and excellent specificity (84.4% vs. 93.2%) of the Korean self-report version upon application of a cutoff score of 16. For clinical purposes, specificity can be sacrificed somewhat for the sake of sensitivity so as not to miss a true patient.37 According to two previous studies using the self-report Y-BOCS,10,11 clinical OCD samples consistently tended to rate their own OCD symptom severity as being less severe than when clinician rated, with differences of ca. 2-3 points in the total score. Steketee et al.10 reported a possible need to adjust self-report scores upward to match interview findings. We also suggest that the clinical cutoff score should be lower than 16 for the Korean self-report version. Using cutoff scores of 13 or 14, the respective sensitivities and specificities in our samples were 90.5% and 84.0% or 89.4% and 86.9%.
This study has several limitations and further research is required. First, the clinical OCD data were collected in a retrospective manner and no structured interviews for diagnosis of OCD were conducted. Second, examination of the Korean self-report version ratings in non-OCD psychiatric samples should be conducted to determine their discriminate validity. Especially, it needs further study including the patients with generalized anxiety disorders, panic disorders, or other relevant anxiety disorders. Finally, the treatment sensitivity of the Korean self-report version should be examined.
In conclusion, our results indicate that Korean self-report version of the Y-BOCS is a psychometrically sound, valid measure for assessing obsessive-compulsive symptoms in both non-clinical and clinical samples. The originally proposed division of OCD severity into obsessions and compulsions in the Korean self-report version appears accurate and adequate. While the self-report Y-BOCS is more cost-effective than the clinician-administered version, the cutoff score for it needs adjustment based on further research.