INTRODUCTION
Suicide is a global public health crisis. Close to 800,000 people die due to suicide every year worldwide [1]. The suicide rate in South Korea is 24.6 per 100,000 people, which is the highest of any nation in the Organisation for Economic Co-operation and Development [2]. Prevention is the only way to reduce suicide; therefore, it is important to identify and reduce modifiable risk factors for suicide [3]. Previous studies on suicide in occupational settings have identified certain risk factors and suggested interventions.
In modern society, people who work non-day time hours are required to manage the demands for 24-hour consumer service. Approximately 15-30% of employee are engaged in a shift-work system [4,5], with some indication that the prevalence of shift work is increasing [6]. However, shift work disrupts circadian rhythms and interferes with social obligations and/or family life that occur during the day. This leads to increased vulnerability to the development of stress-related mental health problems, including suicide [7].
Work hours that result in non-standard sleep can impair an individualŌĆÖs ability to sleep and cause shorter sleep durations, severe sleep debt, and daytime sleepiness with a more prolonged recovery time [8]. A recent review has reported that shift workers have shorter total sleep times than daytime workers [9]. In contrast, H├żrm├ż et al. [10] have suggested that shift work with/without night shifts are associated with increased fatigue and longer sleep times (Ōēź9 hours/day). Sleep disturbances related with shift work are a central mechanism for the relationship between shift work and suicide [7]; therefore, it is important to investigate the dose-response relationship between sleep duration and suicidal ideation and find the appropriate sleep duration that reduces the risk of suicidal ideation.
In addition, working hours should be also considered as a factor to think together with sleep because long working hours counteract sufficient sleep time in a shift work system. Lee et al. [11] have reported that long working hours (>45 hours/week) are associated with suicidal mortality in general workers. They argued that long working hours increases the risk of poor mental health, social isolation, and family conflict. Given shift work interferes with appropriate sleep and social activities that occur during the day [7], shift workers with long working hours can be more vulnerable to the risk of suicide than non-shift workers. However, few studies have investigated the appropriate length of work time for shift workers to reduce this risk.
The aim of this study was to use a nationally representative survey to address three questions. First, are work hours and sleep duration associated with the risk of suicidal ideation in shift workers? Second, what is the appropriate length of work hours and sleep duration to reduce the risk of suicidal ideation? Third, is there an interaction between work hours and sleep duration in their associations with the risk of suicidal ideation?
METHODS
Participants
This study used data collected from the Korean National Health and Nutrition Examination Survey (KNHANES), which is a nationally representative, cross-sectional survey that has been conducted annually by the Korea Centers for Disease Control and Prevention (KCDC) since 1998 [12]. The KNHANES consists of health interviews, health examinations, and dietary surveys to evaluate the health and nutritional status of the Korean population. Participants of the KNHANES are selected using a complex, stratified, multi-stage cluster sampling design among non-institutionalized civilians in South Korea [12]. Self-reported sociodemographic characteristics, such as age, sex, marital status, education level, income, alcohol consumption, smoking status, sleep duration, quality of life, and personal medical history, are collected during the health interview. Anthropometric and blood biochemical data are measured during the health examination. All participants provide written informed consent, and the survey protocol was approved by the KCDC Institutional Review Board (IRB Nos. 2007-02CON-04-P, 2008-04EXP-01-C, 2009-01CON-03-2C, 2010-02CON-21-C, 2011-02CON-06-C, 2012-01EXP-01-2C, 2013-07OCN-03-4C, 2013-12EXP-03-5C, 2015-01-02-6C, 2018-01-03-P-A) (KCDC, 2020).
Selection of ŌĆ£healthyŌĆØ shift workers
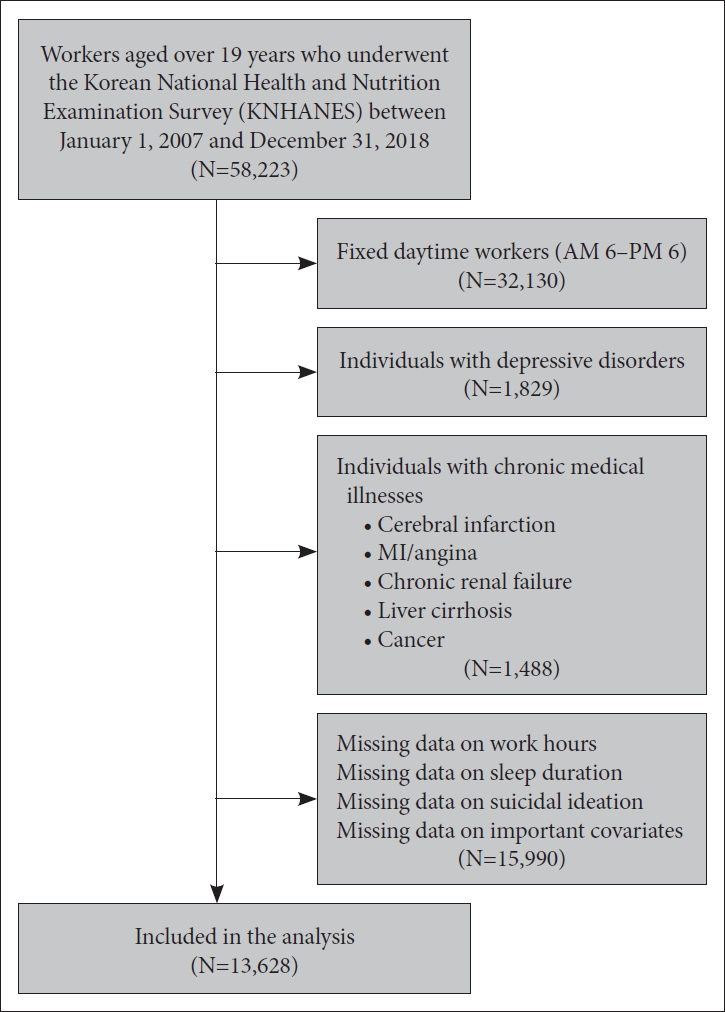
The current study used a cross-sectional design of 58,223 workers aged 19 and older who had participated in the KNHANES between January 2007 and December 2018. The definition of shift work by Knutsson [13] is ŌĆ£an arrangement of working hours that uses teams (shifts) of workers, in order to extend the hours of operation of the work environment beyond that of the conventional office hours.ŌĆØ Therefore, individuals who reported being employed with fixed standard time schedules (06:00-18:00) were excluded (n=32,130). We selected ŌĆ£healthyŌĆØ shift workers without any evidence of a depressive disorder (n=1,829) or physical illness (cerebral infarction, myocardial infarction/angina, chronic renal failure, liver cirrhosis, and cancer; n=1,488) to reduce reverse causation. We excluded participants with missing data (n=15,990). Finally, 13,628 participants were included in our analysis (Figure 1).
Assessment of sleep duration
Participants were asked, ŌĆ£How many hours do you usually sleep a day?ŌĆØ We categorized the responses into five groups: <6, 6 to <7, 7 to <9, 9 to <10, Ōēź10 hours/day. Based on a joint consensus statement of the American Academy of Sleep Medicine and Sleep Research Society [14], we defined individuals sleeping between 7 and <9 hours/day as a reference group.
Assessment of working hours
Participants were asked, ŌĆ£How many hours do you usually work per week, including overtime?ŌĆØ The Labor Standard Act in Korea defines standard working hours as 40 hours/week, with extensions up to 52 hours permitted with the workerŌĆÖs consent [15]. Based on this Act, working hours were divided into three groups: Ōēż40, 40.1-52, and >52 hours/week.
Assessment of suicidal ideation
Participants were asked, ŌĆ£Over the last year, have you ever felt that you would be better off dead?ŌĆÖŌĆÖ Answers in the affirmative were taken to indicate suicidal ideation.
Potential confounding variables
Age, sex, marital status (married, never married, and others), education (less than elementary school, middle school, high school diploma, and college degree or higher), income (1st, 2nd, 3rd, and 4th quartiles), alcohol consumption frequency (Ōēż1 time/month, 2-4 times/month, 2-3 times/week, and Ōēź4 times/week), and smoking status (never smoker, former smoker, and current smoker) were collected using the self-reported questionnaires. The level of anxiety and depressive symptoms was measured using the anxiety/depression items on the Euro-QoL-5D [16]. We excluded individuals with depressive disorders; however, some clinically depressed individuals may not have been diagnosed at the time of survey. Therefore, anxiety/depressive symptoms were included as a covariate. BMI was calculated by dividing weight (kg) by height squared (m2).
We collected data regarding shift work patterns, occupations, and employment status. Shift workers are divided in KNHANES as follows: ŌĆ£fixed-evening shift (14:00-24:00), fixed-night shift (21:00-08:00), regular day and night rotating shift, 24-hours rotating shift, split shift (working 2 shifts in 1 day), irregular rotating shift, and others. We used ten categories of workers based on the International Standard Classification of Occupations of Internal Labor Organization [17]: ŌĆśmanagers,ŌĆÖ ŌĆśprofessionals,ŌĆÖ ŌĆśoffice workers,ŌĆÖ ŌĆśservice workers,ŌĆÖ ŌĆśsales workers,ŌĆÖ ŌĆśagricultural, forestry and fishery workers,ŌĆÖ ŌĆścraft and related trades workers,ŌĆÖ ŌĆśplant and machine operators and assemblers,ŌĆÖ ŌĆśelementary occupations,ŌĆÖ ŌĆśarmed forces,ŌĆÖ and ŌĆśothers.ŌĆÖ Employment status was divided into four groups: ŌĆśwage workers,ŌĆÖ ŌĆśowneroperators and employers,ŌĆÖ ŌĆśunpaid family worker,ŌĆÖ and ŌĆśothers.ŌĆÖ
Statistical analysis
Descriptive statistics were used to display the baseline characteristics according to suicidal ideation. The t-test and chi-square test were used to identify differences between individuals with or without suicidal ideation. Logistic regression was used to calculate the odds ratios (ORs) for the risk of suicidal ideation according to sleep duration or working hours. The relative confounding effect of each of the variables outlined above was investigated in turn, before a final multivariate model including all covariates was constructed. Regression models were mutually adjusted for sleep duration and working hours to examine whether they affected each otherŌĆÖs relationship with the risk of suicidal ideation.
Interactions between sleep duration and working hours were also examined. In addition, considering sex and age difference, interactions by sex and age were analyzed. All statistical analyses were performed using STATA version 14.0 (StataCorp LLC., College Station, TX, USA). A two-tailed p-value <0.05 was considered significant.
RESULTS
Table 1 displays the characteristics of the participants according to their risk of suicidal ideation. We found that 1,443 out 13,628 (10.59%) had suicidal ideation. The groups that expressed suicidal ideation were more likely to be older, women, never smokers, have lower education and BMI, higher income levels, alcohol consumption frequency, and anxiety/depressed symptoms when compared with those without suicidal ideation. In addition, the suicidal ideation group was more likely to report shorter sleep durations than the non-suicidal ideation group.
Table 2 displays the occupational characteristics of the participants according to their risk of suicidal ideation. Participants without suicidal ideation were more likely to have fixed-evening, fixed-night, regular day and night rotating, 24-hours rotating, split, or irregular rotating shifts when compared with those without suicidal ideation. The groups that had suicidal ideation were more likely to be sales workers, agricultural, forestry and fishery workers, elementary occupations, owner-operators and employers, and unpaid family workers when compared with those with no reported suicidal ideation. In addition, the suicidal ideation group was more likely to report longer working hours than the non-suicidal ideation group.
Table 3 shows the results for the relationship between sleep duration and risk of suicidal ideation. There was little difference in the OR for suicidal ideation before versus after adjusting for sleep duration (models 3 vs. 4). In the final model, which was adjusted for confounders including sociodemographic factors, occupation characteristics, anxiety/depressive symptoms, and sleep duration, shift workers who slept <6 and Ōēź10 hours/day had a 36% (95% CI=15-60%, p<0.001) and 42% (95% CI=3-95%, p=0.031) increased risk of suicidal ideation, respectively, compared with those who slept 7 to <9 hours/day (reference group). There was no significant association between sleeping 6 to <7 or 9 to <10 hours/day and the risk of suicidal ideation compared with the reference group. There was a negative relationship between continuous sleep duration and the risk of suicidal ideation; however, the odds ratio was almost 1 (OR=0.93, 95% CI=0.89-0.97, p=0.001).
Table 4 shows the relationship between working hours and the risk of suicidal ideation. There was little difference in the OR for suicidal ideation before versus after adjusting for working hours (model 3 vs. model 4). In the final model, which was adjusted for a range of confounders including sociodemographic factors, occupation characteristics, anxiety/depressive symptoms, and working hours, shift workers who worked >52 hours/week had a 30% (95% CI=13-49%, p<0.001) increased risk of suicidal ideation compared with those who worked Ōēż40 hours/week (reference group). There was no significant association between working 40.1-52 hours/week and the risk of suicidal ideation in shift workers when compared with the reference group. There was a positive relationship between continuous working hours and the risk of suicidal ideation; however, the odds ratio was almost 1 (OR=1.006, 95% CI=1.003-1.009, p<0.001).
There was no evidence of an interaction between sleep duration and working hours with the risk of suicidal ideation (p=0.931). There were interactions by sex or when stratified by age group (greater than or less than 45 years old) in the association between long working hours and the risk of suicidal ideation; the relationship was stronger for men than for women (p<0.01) and for those aged <45 years than for those aged Ōēź45 years (p<0.01). However, there were no interactions by sex (p=0.459) or age (p=0.303) in the association between sleep duration and suicidal ideation.
DISCUSSION
The results of this study showed that both too little (<6 hours/day) and too much (Ōēź10 hours/day) sleep and working >52 hours/week were associated with the risk of suicidal ideation.
Previous studies have reported that both short and long sleep durations are associated with the risk of suicide [18,19]. Littlewood et al. [20] have reported that restoring sleep duration can offer temporary relief from waking problems; therefore, they argue that short sleep durations may counteract helpful interventions that are used before establishing a permanent resolution of suicidal ideation. Conversely, in terms of the relationship between long sleep duration and suicide, cytokines, such as IL-6, can function as mediators between long sleep duration and suicide. IL-6 is somnogenic and associated with a pro-inflammatory state that contributes to a higher suicide risk [18]. In addition, the overuse of opioid and sedative/hypnotic drugs that result in longer sleep may mediate the association with increasing suicidal ideation; participants who overuse opioid and sedative/hypnotic drugs are more likely to report psychiatric difficulties and chronic pain related to suicide [21].
Shift work causes a desynchronization between homeostatic sleep pressure and circadian rhythmicity [22]. Shift workers can sleep during daytime periods; however, the circadian alert signal is high at this time, which results in short, fragmented sleep and homeostatic sleep debt. Conversely, when shift workers need to be awake, the circadian alert signal is low, causing sleepiness, long sleep duration in their workplace. Taken together, shift workers may be more vulnerable to experiencing shorter or longer sleep durations that have negative effects on suicidal ideation. Therefore, maintaining an appropriate sleep duration can be a crucial modifiable factor that can reduce the risk of suicidal ideation in shift workers.
In terms of the relationship between long working hours and suicide mortality, Lee et al.ŌĆÖs [11] study using nationally representative longitudinal data have reported that those working Ōēź45 hours/week have a higher risk of suicide when compared with individuals working 35-44 hours/week. However, their upper limit of working hours is lower than the result of our study. There are several reasons that account for the difference in working hours that increases the risk of suicide between studies. We included shift workers only, whereas Lee et al. [11] assessed all employees, including non-shift workers. In addition, the dependent variables are also different between our study (suicidal ideation) and Lee et al. [11] (suicidal mortality) and we excluded individuals with depressive disorders. A current systematic review study has reported that individuals working 4 hours-on/8 hours-off rosters averaged 1 hour more sleep per night than those working 6 hours-on/6 hours-off and 1.3 hours more sleep than those working 8 hours-on/8 hours-off in a shift work system [23]. Maintaining an appropriate sleep duration is associated with reducing mental health problems, including suicide for shift workers [22]; therefore, long working hours that result in sleep deficits are additional risk factors in the development of suicidal ideation. Furthermore, long working hours have negative effects on the relationships with family and friends [11]. Most activities occur during the day; therefore, shift work is more likely to interfere with social obligations and/or family life, which can cause social isolation and family conflict that is associated with suicidal ideation [7,24].
There were interactions by sex in the association between long working hours and the risk of suicidal ideation. In the current study, the relationship was stronger for men than for women. According to the expectations of cultural gender roles in East Asian cultures, men tend to focus on paid work because their self-identity is often derived from the breadwinner role [25]. Therefore, male shift worker can be more vulnerable to external social and economic stressors related to the workplace than female employees [26]. In addition, in the interactions by age groups in the relationship between long working hours and suicidal ideation, the relationship was stronger for those aged <45 years than for those aged Ōēź45 years. Previous studies have reported that mood fluctuation, mean levels of neuroticism decrease as people age [27]. In addition, increased positivity with age is evident in job attitudes; older workers tend to report higher satisfaction with their job, pay, and supervisor, and higher levels of organizational identification and loyalty [28]. Accordingly, it can be understandable that younger employees are more vulnerable to suicidal ideation than those aged Ōēź45 years under long working hours.
The results of this study should be interpreted with caution because of several potential limitations. First, study design was cross-sectional; therefore, inflated associations and reverse causality are possible. Second, self-reported questionnaires were used to identify whether participants experienced suicidal ideation or not, and their working and sleep hours; therefore, our results may be affected by response bias. Third, we measured suicidal ideation alone as an outcome. Even if suicidal ideation is a distinct risk factor of suicide, information on suicidal behavior or actual suicide is more desirable in examining the association between sleep duration, working hours, and suicide. Fourth, this study included only subjective sleep duration as a dependent variable; however, as sleep quality should be used to evaluate restorative sleep. A future study that includes sleep quality-related parameters is required. Fifth, psychosocial job stress, including poor physical working conditions, high job demands, low job control, effort-reward imbalance, inadequate social support, job insecurity, organizational injustice, and discomfort in an organizational climate have been reported as crucial risk factors of suicide. The present study did not include different job stresses as covariates. Sixth, the rate number of individuals who reported ŌĆ£othersŌĆØ when reporting their shift work pattern was high. This suggests that individuals may be misclassified because of incorrect responses. Seventh, this study did not include any multiple person-level characteristics that are associated with adaptability to shift work as covariates. For example, chronotype, which is an individualŌĆÖs innate circadian preference (morning/evening types) can influence an individualŌĆÖs ability to adapt to shift work.