INTRODUCTION
Even though applied sequential trials of antidepressant treatments, there are 20%-30% depression patients fail to respond to standard treatments [1,2]. The definition of treatmentresistant depression (TRD) is considered as fail to respond to at least two different antidepressants prescribed at adequate dosages and durations or do not achieve clinical remission [3]. TRD may result in poorer cognitive performance [4], worse psychosocial functioning and higher suicidality [5]. Studying the potential neurobiological markers of TRD may help better recognized patients who are treatment resistance and develop novel effective therapeutics.
Nowadays, there are lots of neuroimaging researches studied major depressive disorder (MDD). However, studies about the structure, blood flow and tissue metabolism of the brain in TRD are fewer. Among the existing researches, the results of are inconsistent or contrary. For example, Duhameau et al. [6] used arterial spin labelling perfusion MRI to find that six TRD patients exhibited hyperperfusion in the left dorsomedial prefrontal cortex (DMPFC) and anterior cingulate cortex. Yamamura et al. [7] also discovered TRD patients showed increased spontaneous neural activity in inferior frontal gyrus using resting-state functional magnetic resonance imaging. While recently Li et al. [8] showed that prefrontal cortex (PFC) hypometabolism paly a key role in the TRD neuropathology with positron emission tomography scans. These inconsistent results are unsurprising, as whether variable such as antidepressants and past depressive episodes affect on prefrontal activation is unknown. Even so, these studies provide the clues that the PFC function alteration may be involved in the possible mechanisms in TRD patients. Indirect evidence supported dysfunction of PFC is that by taking repetitive transcranial magnetic stimulation of the dorsolateral PFC (DLPFC), the symptoms of TRD patients have showed to improve [9-11].
PFC not only can exert top-down control over limbic system as a regulatory mechanism for depression [12], but also is a key neural basis part of cognitive function [13]. Li et al. [8] proved attentional performance were significant difference between TRD patients and non-TRD patients. Unfortunately, the patients sample in this study was just grouped according to if patients have history of medication resistance. It should be worth noticed that more and more studies reported MDD lead poorer cognition without symptomatic remission [4,5]. Therefore, we cannot conclude that the cognitive function of TRD patients were more severe than non-TRD. In addition, which abnormalities of PFC related to diminished cognitive functioning is worth studying.
Near-infrared spectroscopy (NIRS) is a noninvasive optical neuroimaging technique that can measure oxygenated hemoglobin (oxy-Hb) and deoxygenated hemoglobin (deoxy-Hb) concentrations in brain tissue which reflected the neural activity [14]. Due to the advantage of relatively nonconstraining, low consumption, portable and repetitive operation, it has be widely used to investigate brain function during cognitive task in several psychiatric disorders especially depressive disorder [15]. However, the specific region which impair depressive symptoms still remain unclear. For example, Akiyama et al. [16] used NIRS found that left frontal activations is significantly smaller during verbal fluency task (VFT) in MDD patients compared with health controls. Whereas most research showed bilateral prefrontal significantly lower activation [17-19]. In addition, recent study suggest remitted depressive patient showed left frontotemporal lower hemodynamic activations [20]. One major reason that may explain the inconsistency is that samples contains clinical subtypes such as refractory depression. To better research the different neural activity between TRD patients and non-TRD patients, this study use NIRS to examine the difference hemodynamic response in PFC area during VFT. As the widely used task in neuropsychological cognitive assessment, VFT has been proved to detect PFC activation in health people and mental disorder patients combined with NIRS and can assess executive control functions by self-monitor [21,22]. In addition, it was the most commonly used task in cognitive neuroimaging study. Therefore, it was selected as the cognitive task in this study.
The aim of this study was to evaluate cognitive performance and prefrontal hemodynamic response between TRD and non-TRD patients use NIRS during VFT. It was hypothesized that impaired performance and decreased prefrontal activation would be observed, furthermore, prefrontal activation pattern associated with cognition would differ in TRD and non-TRD patients.
METHODS
Subject
The study was approved by the ethics review committee of Yu Quan Hospital, and written informed consent was obtained from all participants prior to the commencement of the study. Patients with MDD were recruited from inpatient departments of Yu Quan Hospital from September 2013 to August 2016. The diagnoses of all patients were established by the Structured Clinical Interview according to the DSM-IVTR (SCID). Exclusion criteria include: 1) age less than 18 or over 60 years; 2) left-handed which is evaluated by Edinburgh handedness inventory; 3) major physical illnesses such as malignant tumor, chronic renal failure, severe heart disease, and severe respiratory disease; 4) other psychiatric disorders and neurological disorders; 5) substance abuse; 6) took medication within the 3-month period prior to the study; and 7) received electroconvulsive therapy. Finally, 40 patients were include in the present study. Twenty-three right-handed healthy controls (HC) were recruited from the local community by advertisements. Age, gender and educational level were matched between MDD groups and HC. The control subjects were screened using the non-patient edition of the SCID to confirm the lifetime absence of a history of psychiatric or neurological disorders and were interviewed to exclude family history of psychiatric illness.
Study design
Before started antidepressant treatment, each participants underwent NIRS imaging. Antidepressants were empirically prescribed according to the clinical judgment of the treating psychiatrist. Three classes of antidepressants include tricyclic antidepressants, serotonin-norepinephrine reuptake inhibitors, and selective serotonin reuptake inhibitors were used.
Treatment resistant is defined as a poor response to at least two different classes of antidepressant trials with each trail in adequate dosages and duration (6 weeks) [23]. Specifically, after antidepressant treatment, patients who have less than 50% Hamilton Depression Rating Scale (HAMD, 24-item) [24] score reduction were considered as TRD patients and more than 50% were considered as non-TRD patients.
The activation task
Present task procedure was similar to previous study [25,26]. We took semantic category versions of the VFT to stimulate prefrontal activation which is reflected prefrontal hemodynamic responses. Simultaneously measured oxy-Hb changes during VFT. The procedure was four block (vegetables, domestic applications, four-legged animals, and fruits) with each block include 15 second pre-task baseline, 30 second task and 15 second pro-task baseline. Each participants were sat comfortably in the front of screen presented task with a distance of 50 cm. During pre-task and pro-task period, they were asked to stare at the symbol of “+” on screen quietly, while during the task period, they were asked to generate as many Chinese words as possible that belonged to the designated species. The total numbers of correct words generated during VFT period were represented the participants’cognitive performance scores. In addition, we took index of the accuracy (%) of the correct words to evaluate behavioral performance.
NIRS measurements
Forty-five channels NIRS machine (FOIRE-3000, Shimadzu Corporation, Kyoto, Japan) was used to measures oxy-Hb and deoxy-Hb during cognitive task. The 14 pairs of probe arrangement used 7×4 installation modes with each channel (ch) contain a pair of emitter and detector probe at the distance of 3 cm. The most inferior probes were positioned along the Fp1-Fp2 line according to the International 10-20 system of electroencephalogram electrode placement [27]. With the probe arrangement, NIRS can measure oxy-Hb and deoxy-Hb concentration changes of PFC. The time resolution was set 0.1 sec. Before export data, baseline corrections and filtered were used to reduce artifact motion.
Statistical analysis
We used one way analysis of variance (ANOVA) to analyze continuous variables include demographic characteristics (age and education level), clinical variables (illness duration, past depressive episodes, HAMD score) and VFT performance (the correct number of items, accuracy) among the three groups. As to categorical variables (gender) among groups, we used contingency table analysis. ANOVA was also used to analyze oxy-Hb changes differences among the three groups.
The value of oxy-Hb changes (calculated by subtracting the mean oxy-Hb of the task period from that mean oxy-Hb of the pre-task period), as a much reliable statistical indicator [28,29], stronger correlation with blood oxygenation level-dependent signal measured by functional MRI [30] and better signal to noise ratio than deoxy-Hb change [31], is selected to directly reflect regional cerebral blood flow changes and cognitive activation. For further post hoc test, we took Bonferroni test. Homogeneity of variance was tested to compare the distribution shape of the different groups. Benjamini-Hochberg’s procedure was adopted for multiple comparisons analyses of 45-channel testing correction. The q value of the maximum false discovery rate (FDR) was set at 0.2 so that the false positive rate was no higher 20% on average (FDR-corrected).
To examine the relationships between oxy-Hb changes in each channel and clinical variables, Spearman’s rank correlation coefficients were calculated for TRD patients and non-TRD patients.
All statistical analyses were performed using the Statistical Package for the Social Sciences for Windows (SPSS version 22.0; IBM Corp., Armonk, NY, USA).
RESULT
Demographic characteristics and clinical variables
As shown in Table 1, the age, gender, and education level were not significant different among TRD, non-TRD and HC groups. Between TRD and non-TRD groups, illness duration and severity of depressive symptoms before treatment as assessed with HAMD showed not significant differences, but HAMD score after treatment were significant differences. In addition, HAMD score before treatment were significant differences between TRD and HC groups and between non-TRD and HC groups. However, HAMD score after treatment were not significant different between non-TRD and HC groups, but still exhibit statistically significant differences between TRD and HC groups.
VFT performance
The VFT performance of the three groups was shown in Table 1. As it presented, the correct number of items among the three groups was statistically significant differences in the four categories. When compared two of the three groups, both the TRD and non-TRD groups generated a significantly less number of items in all categories compared to the HC group; however, no significant differences between the TRD group and non-RD group in all categories. The accuracy among the three groups were not significantly different.
Comparison of oxy-Hb changes among group
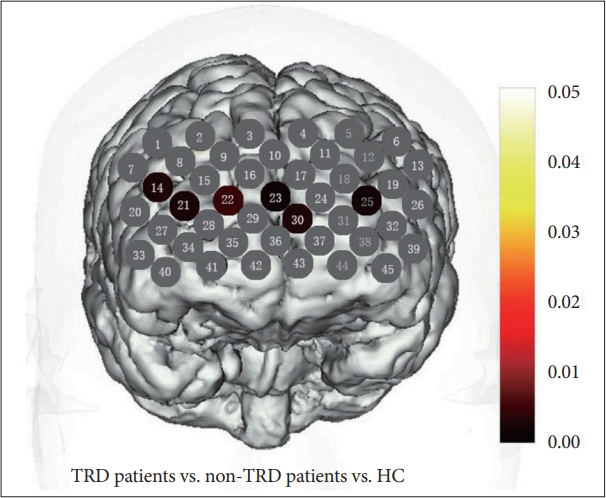
Oxy-Hb change were homogeneous in 34 channels (p>0.05), except channels 7, 10, 19, 20, 26, 29, 31, 35, 37, 42, 43. In the 32 channels, ANOVA revealed significant differences among groups in channels 14, 21-23, 25, 30 (FDR-corrected p<0.2) (Figure 1). When use Bonferroni to conduct the post hoc analysis, non-TRD patients exhibited significantly lower oxy-Hb activation than HC groups in channels 21 (FDR-corrected p<0.2) (Figure 2A). TRD patients exhibited significantly lower oxy-Hb activation than HC groups in channels 14, 21- 23, 25, 30 (FDR-corrected p<0.2) (Figure 2B). Both patients exhibited a reduced activation in channels 21 when compared with HC groups. In direct comparison within TRD and non-TRD groups, the mean oxy-Hb changes in TRD patients were significantly smaller than those in non-TRD patients in channel 23 and 30 (FDR-corrected p<0.2) (Figure 2C and D).
Correlation between oxy-Hb changes and clinical assessments
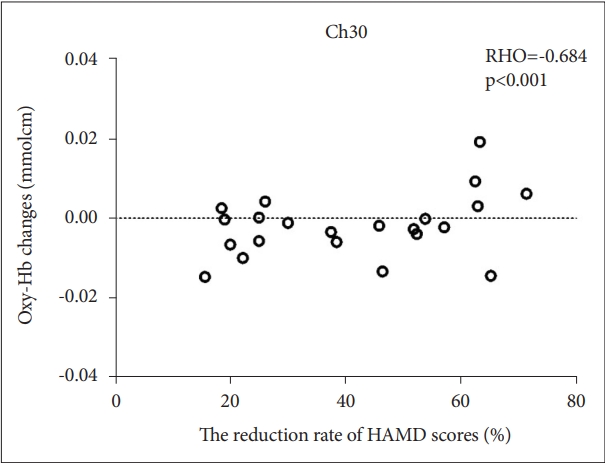
In TRD and non-TRD group, a significant negative correlation between mean oxy-Hb changes and HAMD scores in channel 21 (FDR-corrected p<0.2) (Figure 3), which approximately located in right DLPFC. A significant positive correlation between mean oxy-Hb changes and the reduction rate of HAMD scores in channel 21 (FDR-corrected p<0.2) (Figure 4), which approximately located in DMPFC. Furthermore, no significant correlation was observed between the oxy-Hb changes and illness duration (FDR-corrected p>0.2) in tested channels in TRD and non-TRD group.
DISCUSSION
This study used NIRS imaging to measure the hemodynamic response associated with cognitive activation in TRD patients and non-TRD patients. The comparison of VFT performance and PFC activation among TRD, non-TRD and HC group showed that both TRD and non-TRD patients exhibited significantly worse performance and smaller oxy-Hb activation in DLPFC. Within TRD and non-TRD groups, there were no significant difference in VFT performance, however, the activation of oxy-Hb changes in TRD patients was significantly smaller than non-TRD patients in DMPFC. Furthermore, depressive symptoms severity as assessed by the HAMD showed significant negative correlation with right DLPFC in TRD patients and non-TRD patients.
To our knowledge, this study is the first report using NIRS imaging to evaluate cognitive performance and prefrontal hemodynamic response in the PFC area between TRD and non-TRD patients during VFT. NIRS may assist to understand the neural basis of treatment resistant in MDD patients.
Impaired executive function in patients groups
VFT is a kind of neuropsychological test to assess executive functions [32]. Compared with HC group, both TRD and non-TRD patients generated significantly fewer correct words in the four categories. This finding demonstrate the executive functions of MDD patients were impaired. Producted less number of correct words during VFT may imply that deterioration of semantic storage and dysfunction of frontal cortex which related to the ability to retrieve a series of nouns [33]. The result is consistent with previous studies which proved MDD patients exhibited poorer performance of executive function than normal control [34-37]. As far as we know, there are studies reported no impairment of VFT performance between MDD patients and normal control [18,38-40]. In these studies, the different time setting may explain the discrepancies. In our version of VFT, the time setting was four categories words within 4 minutes and 30 seconds for each category task period. Using the version of VFT with the same four categories words but increase time during silence, our lab showed that there were no significant differ between MDD patients and normal controls [18]. The reason may be that the patients get relax with extended time and the subject can keep generating words regularly without the influence of task period.
However, TRD and non-TRD patients performed similar. This finding may suggest that the extent of executive function impairment were similar and the trait of treatment resistant have a minimal impact on this kind of cognitive performance in keep generating words regularly. The result is differ with previous study which suggest attentional deficits in TRD patients [8] and may represent different aspect cognitive function abnormal in TRD patients, but need more research to support the result.
Hypofrontality during VFT task in TRD and non-TRD patients
In the present study, we found TRD and non-TRD patients showed smaller oxy-Hb activation in DLPFC prefrontal compared with HC group. This finding is in accord with previous functional neuroimaging studies which examined activation of depression patients’ prefrontal regions during cognitive tasks [39-41]. Hypoactivity in the prefrontal area during VFT task period has been suggested that depression patients cannot able to obtain a corresponding increase oxygen in blood supply to compensate for consumed, which is crucial for proper neuronal activity. DLPFC plays an important role in regulating emotions [42] and cognition [43,44]. Thus dysfunction of the area lead to insufficiencies in emotion regulationand cognitive aspect in depression patients. Furthermore, the severity of depression of TRD and non-TRD patients had a negative correlation with oxy-Hb changes in the region of right DLPFC. This may suggest neural vulnerability in terms of the severity of depression symptoms. The lower oxy-Hb activation in the right DLPFC trend to increase gradually in the severity of depression symptoms. The dysfunction of DLPFC may return to normal after antidepressants prescribed at adequate dosages and durations. That is to say, with the depression symptoms alleviated, oxy-Hb changes in the right DLPFC will be increased.
The function of DMPFC and treatment resistant
We observed a lower oxy-Hb activation mainly located in DLPFC and DMPFC (ch 14, 21-23, 25, 30) in the TRD patients compared with HC. While compared with non-TRD patients, TRD patients exhibited a lower oxy-Hb activation in channel 23 and 30 of the DMPFC. In addition, the reduction rate of HAMD scores of TRD and non-TRD patients had a positive correlation with oxy-Hb changes in the region of DMPFC. In this study, patients were in first episode and medicine free. Then this result may present a profile that biological factors paly essential role in TRD patients.
Previous studies have shown abnormal connectivity of medial prefrontal regions and thalamus is related to refractoriness in depression patients [45]. The lower activation of oxy-Hb in medial prefrontal regions predict poor response to SSRI in depression patients [46]. Samson et al. [47] showed greater activation in DMPFC response better to pharmacological treatment. Disrupted connectivity of medial PFC was continued exist in depression patients after 12 weeks of antidepressant treatment [48]. All this study emphasize the importance role of medial prefrontal regions in the refractory depression patients.
As a central role in affect regulation, DMPFC has been identified as dorsal nexus—a unique region of cortical network which converge cognitive control, emotion regulation and self-reflection [49]. Recent studies have shown that reduced activation in the middle frontal gyrus is an indicator of trait-related brain abnormalities in MDD patients [50]. So we speculate that abnormal activation in DMPFC area may be the pathological basis of refractoriness and may characterize a subgroup of depression people associate with refractoriness.
Limitation
There are some limitations should be pointed out in our studies. Firstly, the study data is cross-sectional, whether abnormal activation prefrontal area change after antidepressant need further data in longitudinal studies. Secondly, the refractoriness of participating in present study were confirmed by the definition—a poor response to at least two different classes of antidepressant trials with each trail in adequate dosages and duration (6 weeks), not according to if patients have history of medication resistance. Thirdly, we didn’t exclude the MDD patients with anxiety.
Conclusions
In conclusion, TRD patients and non-TRD patients exhibited significantly worse performance and smaller oxy-Hb activation in DLPFC compared with HC subjects. Within TRD and non-TRD groups, there were no significant difference in VFT performance. However, the activation of oxy-Hb changes in TRD patients was significantly smaller than non-TRD patients in the bilateral DMPFC. This preliminary exploratory study suggest different prefrontal activation patterns between TRD patients and non-TRD patients. fNIRS may serve as a useful tool for distinguishing TRD patients from depressed patients by measuring prefrontal activation patterns patterns. Furthermore, depressive symptoms severity as assessed by the HAMD showed significant negative correlation with right DLPFC in TRD patients and non-TRD patients.