INTRODUCTION
Borderline personality disorder (BPD) is a pervasive pattern of instability in interpersonal relationships and self-image; it causes marked impulsivity, begins by early adulthood, and presents itself in a variety of contexts [1]. Owing to the nature of BPD, frequent risky behaviors are exhibited in various situations. BPD is commonly comorbid with alcohol and substance abuse related disorders. Overall, 72% of patients with BPD reported self-harm experiences in their life, whereas 31% reported suicide attempts [1-3]. Furthermore, studies have revealed that people with a borderline personality tendency (BT) express stronger reactive aggression as a response to others’ behaviors, compared to healthy controls (HC) [4-6].
Risky behaviors in patients with BPD are caused by executive dysfunction such as emotion dysregulation and impulsivity [7-9]. According to the biosocial model by Linehan [10], risky behaviors of patients with BPD occur as a result of attempting to control overwhelming negative emotions [11]. Further, expansion of this biosocial model suggests that the dysfunctional behaviors exhibited by patients with BPD are a result of impulsivity and emotion dysregulation [12].
An alternative model that views personality types as continuums have been proposed in the diagnosis of personality disorders [1]. In addition, BT group is viewed as a boundary group before developing into BPD [13]. If personality traits are understood as quantitative dimensional concepts, then it is possible to infer decision-making patterns of BPD using research on individuals with BT.
The Game of Dice Task (GDT) [14] is a decision-making task that is used to measure executive functions and associated behavioral responses. This task requires participants to make a long-term beneficial decision, through a continuous decisionmaking process, involving feedback with rewards and losses. As the goal of the task is to maximize the final balance, participants should continuously choose “safe decisions” with small, yet highly probable rewards and less probable losses to secure an optimum balance in the long run. Therefore, GDT allows individuals to assess the decisions’ degree of risk and safety.
In addition, GDT analyzes the subsequent process after feedback. For example, if a participant makes a risky decision in the previous trial and receives negative feedback (loss), one can assess whether they would maintain the risky decision or switch to a safer option in the next trial. As decision-making problems of patients with BPD occur due to poor processing of feedback, particularly negative feedback to decision-making [15], this task enables a deeper analysis of whether individuals with BT would exhibit BPD characteristics in a decisionmaking task.
A previous study that employed GDT for BPD patients found that they made riskier decisions and were less likely to stay with or switch to the safe decision based on the feedback, compared to the control group [16]. However, there has been only one study using GDT for patients with BPD, and no additional research has been conducted with respect to this demographic. Therefore, studies are needed to explore the effect of situational factors, such as social situations, on decision-making patterns in individuals with BT.
Social exclusion refers to feeling lonely, isolated, or excluded from an individual or a social group [17]. Typically, most people experience psychological distress and functional problem after social exclusion [18,19]. In particular, patients with BPD experience distress when they feel socially excluded during a social interaction. This is a major psychopathological feature of BPD, which differentiates it from other personality disorders, characterized by excessive fear of abandonment cues and unstable interpersonal patterns [20,21].
Furthermore, prior findings suggest that patients with BPD report stronger and more negative emotions such as anger and humiliation, compared with HC when they socially excluded [21,22]. Not only that, but the social exclusion experience affects social cognitive abilities in patients with BPD [23-25]. Prior studies also reveal that individuals with BT showed significant reduction in identification accuracy of neutral expression after experiencing social exclusion; however, this accuracy did not significantly change after experiencing the opposite situation, social inclusion [24]. In summary, patients with BPD who experienced social exclusion compared to social inclusion demonstrated severe psychological distress and difficulties in social cognitive functions.
Prior studies have confirmed the negative psychological effects of social exclusion in individuals with BPD. However, most studies either relied on self-reports of patients with BPD or focused on their internal psychological variables. Furthermore, experimental studies investigating the effect of psychological distress in patients with BPD on their behaviors are scarce. Although some studies report aggressive behaviors when patients with BPD experience exclusion in an interpersonal context [26-28], no study has examined how decision-making patterns related to executive functions can cause risky behaviors under certain social situations.
This study aimed to investigate how individuals with high BT, compared with low BT, make decisions in different social situations. The hypotheses are as follows: 1) individuals with high BT will make riskier decisions compared to the low BT; 2) the group that experienced social exclusion will make riskier decisions compared to the group that experienced social inclusion; and 3) there will be an interaction between the group and social situation condition; specifically, 3-1) for the social exclusion condition, individuals with high BT will make riskier decisions compared to low BT and 3-2) for the social inclusion condition, no significant difference between the decisionmaking patterns of those with high and low BT will be found.
METHODS
Participants and procedure
This study included Korean women aged 18-30 years, living in a metropolitan area. To screen individuals for high and low BT groups, the Personality Assessment Inventory-Borderline Features Scale (PAI-BOR) was used. Screening surveys were distributed both online and offline, and 556 respondents completed the survey. The mean age of respondents was 21.67 (standard deviation [SD]=3.46) years, and the mean score of PAI-BOR was 26.97 (SD=10.05).
The Korean validation study for PAI-BOR categorized a raw score of 39 or above as having BT [13]. This criterion was also applied to the current study. The low BT were those with scores below 1 SD, based on a prior study [29]. The exclusion criteria included those who were currently taking psychiatric medication, those who were hospitalized or treated for neurological, psychological, developmental, or other serious disorders within the last year, or those who were psychology major students (except first-year students).
Sixty-seven participants who met the study’s inclusion criteria participated in the main experiment. Participants were allocated to one of the two social situation conditions (exclusion vs. inclusion). The data of nine participants were excluded from the analysis due to dropouts, reverse scoring, and errors in the program or in the Cyberball game performance (guessing the existence of confederates), thus leaving 58 participants. The mean age of participants was 20.95 (SD=2.69) years, and the age range was 18-29 years.
Participants experienced their allocated social situation condition through the Cyberball game. Next, they performed GDT and completed the manipulation check questions and demographic information. The latter included their age, years of university, and monthly income (including allowance). The study was approved by Chung-Ang University Institutional Review Board (Approval Number: 1041078-202101-HRSB-014-01C).
PAI-BOR
To screen high and low BT, the PAI-BOR, developed by Morey [30] and validated for Korean university students by Hong and Kim [13] was used. PAI-BOR measures key personality characteristics of BPD patients and identifies the level of personality characteristic on a continuum. The subscales consist of affect instability, identity problems, negative relationships, and self-harm, measured using a 4-point Likert scale (0=not at all true, 1=slightly true to 3=very true). Possible scores range from 0-69, and higher scores indicate higher BT.
Cyberball game: manipulation of social situations
To manipulate social situations, the Cyberball game, developed by Williams et al. [31] was used. For the Cyberball game, participants were told that they would be playing an online computer ball game with two other participants to perform “a computer task for visual image training.” The two other participants were virtual, computer-generated people. Participants allocated to the social exclusion condition exchanged the ball equally with virtual players for the first three times; however, they did not receive the ball from the fourth time onward; meaning they received the ball only 3 out of 30 times. In the social inclusion condition, participants received the ball 10 out of 30 times (33.3%).
Manipulation check questions comprised ball possession rate and feelings of exclusion. Scores for exclusion feelings were calculated as mean scores for two exclusion/ignorancerelated items. They were measured using a 7-point Likert scale (1=not at all to 7=very much).
Decision-making task: GDT
To measure participants’ decision-making patterns, GDT [14], was utilized. In this task, participants were required to guess the number on the dice thrown, after which they received either a reward or a loss. Here, participants’ goal was to gain as much money as possible, starting from the game money of 1,400,000 KRW. If any of the selected dice combinations, (one-, two-, three-, or four-digit combinations) matched the number on the dice thrown, participants received a reward. However, in the absence of a match, they incurred a loss.
In addition to the total number of games, rules for reward and loss probabilities were clearly stated on the game screen for the participants. Before throwing the dice, participants were required to choose a single option from the six available which included a single number, three options including two numbers, two options including three numbers, or three options including four numbers. If any of the numbers in the chosen option matched the number on the thrown dice, participants received rewards as follows: 1,400,000 KRW for a single combination, 700,000 KRW for a 2-digit combination, 280,000 KRW for a 3-digit combination, and 140,000 KRW for a 4-digit combination. However, in the absence of a match, participants would lose the same amount of money that they could have gained.
The feedback following the participants’ decision was presented as rewarded or lost money on the screen, and the balance was immediately changed according to the result. Participants could receive a large reward if they chose options with a single number or two; however, the probability of this occurrence was less than 34%, while there would be a greater probability of losing a huge amount of money. Therefore, this would be a risky decision in the long-term. Nevertheless, choosing options with three or four numbers could mean that the probability of receiving a small reward was greater than 50%, and even if the participants lost money, it would be a small amount with a lower probability. Therefore, this was considered a safe decision.
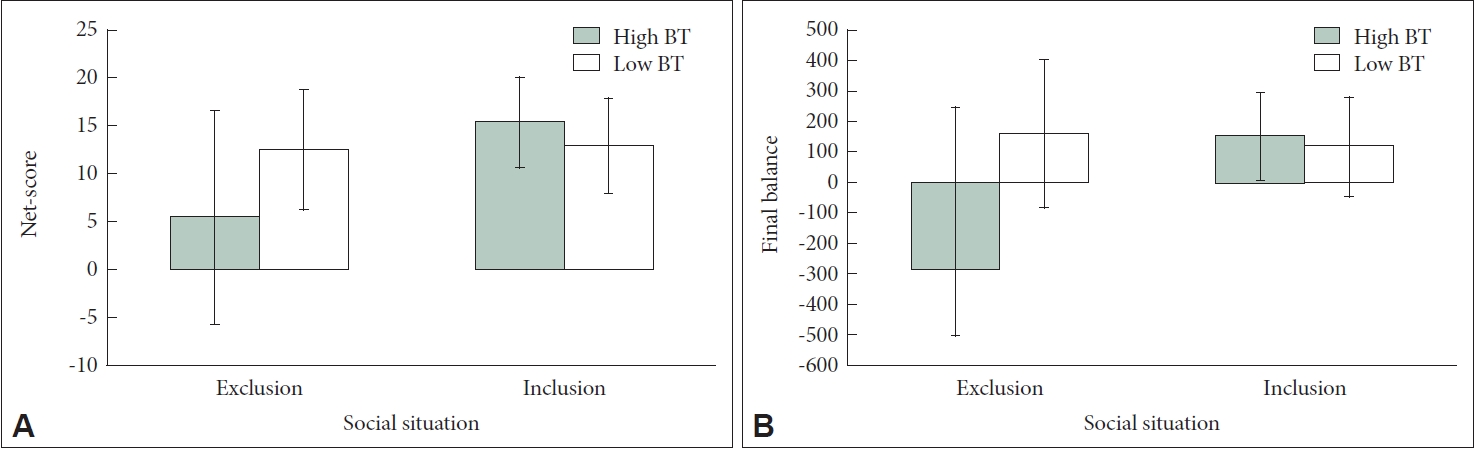
The performance results for this task were measured through the net-score, which was calculated by subtracting the frequency of risky decisions from that of safe decisions. Higher net-scores indicate safer decisions, whereas lower net-scores indicate riskier ones. Additionally, since a smaller final balance implied riskier decision-making, the final balance of the task was also analyzed.
Through this task, participants’ feedback processing was examined by analyzing whether participants stayed with or switched their decisions after receiving feedback from the previous trial. We investigated how their decision-making frequency changed during the eight types of cases presented.
Data analysis
This study used the Statistical Package for Social Sciences Version 26.0 (IBM Corp., Armonk, NY, USA) for data analysis. First, an independent samples t-test and a two-way analysis of variance (ANOVA) were conducted to assess participants’ characteristics and homogeneity. An independent samples t-test was conducted for manipulation check of the social situation. To compare decision-making patterns of each social situation condition, a 2 (group: high BT vs. low BT)×2 (social situation: social inclusion vs. exclusion) ANOVA and post-hoc analyses were conducted. To additionally analyze feedback processing, a 2 (group) × 2 (social situation) ANOVA and post-hoc analyzes were conducted for each of the eight possible cases.
RESULTS
Homogeneity tests of participant characteristics and manipulation check
The two-way ANOVA that was used to assess the homogeneity in participants’ characteristics for each group and condition revealed non-significant differences for both age and monthly income [Age: FGroup(1, 54)=0.39, p>0.05; FCondition(1, 54)=0.09, p>0.05; FGroup×Condition(1, 54)=2.01, p>0.05 and Monthly Income: FGroup(1, 54)=1.68, p>0.05; FCondition(1, 54)=1.39, p>0.05; FGroup×Condition(1, 54)=0.01, p>0.05].
The independent samples t-test used to determine the level of similarity in individuals with BT between the two conditions revealed non-significant differences [mean (M), Mexclusion=28.31, SDexclusion=16.19; Minclusion=27.93, SDinclusion=14.13; t(56)=0.10, p>0.05]. Therefore, homogeneity was verified for BT between the two conditions.
To check whether the Cyberball game induced intended social situations, an independent samples t-test was conducted. The results revealed that the social exclusion condition reported a lower ball possession rate [Mexclusion=8.22, SDexclusion=7.11; Minclusion=38.97, SDinclusion=10.03; t(50.46)=-13.47, p<0.001] and higher feelings of social exclusion [Mexclusion=7.34, SDexclusion=2.22; Minclusion=2.98, SDinclusion=2.20; t(56)=7.51, p<0.001]. Therefore, the social situation manipulation was considered successful.
Risky decision-making of groups within each social situation
To analyze the differences in decision-making patterns of individuals with high and low BT for each social situation condition, a two-way ANOVA was conducted. First, the net-score of GDT was set as a dependent variable. Although there was no significant main effect of group, significant main effect of condition and interaction effect between group and condition were found [FGroup(1, 54)=1.51, p>0.05; FCondition(1, 54)=7.68, p<0.01; FGroup×Condition(1, 54)=6.54, p<0.05]. As the interaction effect was significant, a simple effects analysis was conducted (Figure 1A). For the social exclusion condition, individuals with high BT made riskier decisions compared to low BT [t(20.16)=-2.10, p<0.05], whereas in the social inclusion condition, there was no significant difference between the groups [t(27)=1.43, p>0.05].
When the final balance was set as dependent variable, the main effect of condition was not significant; however, since the main effect of group and interaction effect between the groups and conditions were significant [FGroup(1, 54)=3.86, p=0.055; FCondition(1, 54)=3.35, p>0.05; FGroup×Condition(1, 54)=6.23, p<0.05], a simple effects analysis was conducted (Figure 1B). For the social exclusion condition, individuals with high BT had a smaller final balance compared to low BT [t(16.53)=-2.69, p< 0.05], whereas for the social inclusion condition, the difference was not significant [t(27)=0.45, p>0.05].
Feedback processing of groups within each social situation
To analyze feedback processing for the groups and conditions, all possible cases of decisions made in the trial (stay with decision vs. switch decision) after the previous trial (safe decision vs. risky decision) and its feedback (reward vs. loss) were identified. Following this, one-way ANOVAs were conducted for each case. Different results were produced for each case (Table 1).
First, there was a significant main effect of condition and interaction effect in the case of staying with the safe decision after positive feedback [FGroup(1, 54)=0.10, p>0.05; FCondition(1, 54)=7.89, p<0.01; FGroup×Condition(1, 54)=3.95, p=0.052]. Since the interaction effect was significant, the simple effects analysis was conducted. The results revealed that individuals with high BT were less likely to stay with a safe decision after positive feedback for social exclusion compared to the social inclusion condition [t(23.32)=-3.09, p<0.05]. However, the difference between the conditions was not significant for low BT [t(28)=-0.64, p>0.05].
Next, a significant interaction of group and condition was identified, in the case of switching to a risky decision after negative feedback [FGroup(1, 54)=2.15, p>0.05; FCondition(1, 54)=3.16, p>0.05; FGroup×Condition(1, 54)=6.26, p<0.05]. The simple effects analysis revealed that individuals with high BT were more likely to switch to a risky decision in the social exclusion condition compared to the social inclusion one after receiving negative feedback [t(15.34)=2.33, p<0.05]. However, this difference was not significant for low BT [t(28)=-0.81, p>0.05].
In addition, a significant main effect of condition in the case of switching to the safe decision after negative feedback for making a risky decision was reported [FGroup(1, 54)=0.20, p> 0.05; FCondition(1, 54)=5.54, p<0.05; FGroup×Condition(1, 54)=0.30, p>0.05]. Participants in the social exclusion condition (M=1.41, SD=1.21) were more likely to switch to a safe decision after receiving negative feedback for making a risky decision, compared to the inclusion condition (M=0.72, SD=1.00).
Furthermore, a significant main effect of condition in the case of staying with a risky decision after receiving positive feedback for making a risky decision was identified [FGroup(1, 54)=0.05, p>0.05; FCondition(1, 54)=4.92, p<0.05; FGroup×Condition (1, 54)=0.52, p>0.05]. Participants in the social exclusion condition (M=0.66, SD=1.40) were more likely to stay with a risky decision after receiving positive feedback for making a risky decision in the previous round compared to participants in the inclusion condition (M=0.07, SD=0.26).
Finally, significant main effects of group and condition were found, and interaction in the case of staying with a risky decision after receiving negative feedback for making a risky decision [FGroup(1, 54)=6.43, p<0.05; FCondition(1, 54)=4.95, p<0.05; FGroup×Condition(1, 54)=10.10, p<0.01]. In particular, individuals with high BT (M=1.61, SD=2.85) were more likely to maintain a risky decision after receiving negative feedback for making risky decision compared to low BT (M=0.37, SD=0.81), and participants in the social exclusion condition (M=1.48, SD=2.76) were more likely to make such decisions compared to the inclusion condition (M=0.45, SD=1.06). Furthermore, the simple effects analysis revealed that individuals with high BT in the social exclusion condition were more likely to stay with a risky decision after receiving negative feedback for making a risky decision, compared to those in the inclusion condition [t(15.47)=2.74, p<0.05]. However, no significant difference between conditions for low BT was reported [t(17.07)=-1.62, p>0.05].
No significant results were found for the remaining cases [FGroups(1, 54)<3.65, ps>0.05; FConditions(1, 54)<2.64, ps>0.05; FGroup×Conditions(1, 54)<2.78, ps>0.05].
DISCUSSION
This study investigated differences in decision-making patterns among individuals with high and low BT under different social situations. The social situations were induced using the Cyberball game [30], in either the social exclusion or social inclusion condition. Decision-making patterns were investigated using GDT [14], which measured safe or risky decisionmaking. In addition, the feedback processing was analyzed to assess the processing of feedback following decision-making as well as its effect on the next decision.
First, individuals with high BT made riskier decisions compared to low BT, in particular, individuals who experienced social exclusion made riskier decisions compared to those who experienced social inclusion. The high rejection sensitivity of individuals with BPD may have caused the executive dysfunction when they faced social exclusion. This characteristic makes it more likely for BPD patients to experience negative emotions such as rejection and abandonment anxiety when interacting with others [32].
In addition, the results of feedback processing revealed that individuals with high BT did not effectively process negative feedback after risky decision-making when social exclusion was experienced, compared to low BT. Furthermore, when individuals with high BT experienced social exclusion, they were more likely to make risky decisions in subsequent trials after receiving negative feedback (loss), regardless of the decision made in the previous trial.
BPD can lead to decision-making problems due to poor processing of feedback received from decision-making tasks [16,33]. According to previous studies, BPD patients are unable to differentiate between positive and negative feedback in the brain; moreover, they experience significant reductions of brainwave reactions, which indicate learning of negative feedback, suggesting biological deficits in feedback processing [15].
Based on the results from this study, some limitations and directions future studies can be suggested. First, participants of this study were individuals with high levels of BT rather than patients with BPD. Additionally, only female participants were included in the study. Therefore, decision-making patterns of males with BT were not examined. Thus, future studies using clinical groups with a larger sample size and male participants should be conducted.
Second, this study utilized the Cyberball game for participants to experience certain social situations, where they met with the confederates as in-game characters. This is qualitatively different to real-life, face-to-face interactions. Therefore, in future studies, the social exclusion experience in face-to-face situations should be considered.
Despite the limitations, the findings of the current study have the following implications. First, this is the first study to investigate how social situations affect risky decision-making in individuals with high BT. To expand the results of previous studies on risky decision-making in patients with BPD, the current study set social situations that can be particularly suitable for individuals with high BT as a moderating variable to investigate their decision-making patterns in a new context.
Second, this study is meaningful as it behaviorally measured the psychological changes of individuals with high BT after experiencing social exclusion. Problematic behaviors such as alcohol or substance abuse and risky sexual behaviors cannot be measured in an experimental setting due to ethical reasons. Most studies have utilized self-report measures to assess factors that can affect behaviors such as negative emotions, threat to needs, and intention for risky behaviors [20].
Third, the current study meaningfully analyzed how individuals with high BT process the feedback on their decisions using GDT. It also identified vulnerability in feedback processing following certain social situations that led to the manifestation of risky behaviors.
Finally, the results of this study can be utilized in counseling and treatment settings of individuals with high BT. For example, the therapist should carefully approach negative consequences that individuals with high BT can experience because of their decisions and behaviors. This is especially true when they have experienced social stigma, ostracism, or social exclusion.